Transcription
Vet Clin Food Anim 21 (2005) 623–635Pain Management in CattleDavid E. Anderson, DVM, MS*,William W. Muir, DVM, PhDDepartment of Veterinary Clinical Sciences, College of Veterinary Medicine,The Ohio State University, Columbus, Ohio 43210, USACrises are often encountered in ruminant veterinary practice and mayinclude abomasal volvulus, intestinal accidents, cesarean section, fracture,extreme distortion of acid-base balance, and hydration as encountered incattle that have severe enteritis. These diseases often cause pain or distress.Pain and the biologic responses to it are part of a highly integratedmultidimensional system that causes all animals to react, respond (fight,flight, freeze), and protect themselves from their environment. Whether ornot animals ‘‘feel’’ (perceive) pain the same as humans is immaterial becausemost of the neural elements and biologic consequences (physiologic,neuroendocrine, behavioral) of pain are the same among all mammalianspecies. One clinically useful definition of animal pain states that ‘‘pain is anaversive feeling or sensation associated with actual or potential tissuedamage and resulting in physiologic, neuroendocrine, and behavioralchanges that indicate a ‘stress’ response’’ [1].The importance of the sensation of pain in maintaining and protectingthe normal physiologic condition of the body has led some to consider painas a homeostatic emotion that initiates feeling and motivation [2,3]. Thelatter consideration is why pain perception (nociception) is not consideredto fully represent the pain experience and helps to explain the relationshipbetween painful experiences and pain behaviors in animals. In this context,pain can be broadly categorized as adaptive or maladaptive [4]. Adaptivepain increases the potential for survival by protecting the animal from injuryand promoting healing. Maladaptive pain, by contrast, is a disease createdby pathologic processes that result in the persistence of pain long after theinitiating causes have been removed. The pain system includes sensors,* Corresponding author.E-mail address: Anderson.670@osu.edu (D.E. Anderson).0749-0720/05/ - see front matter Ó 2005 Elsevier Inc. All rights clinics.com
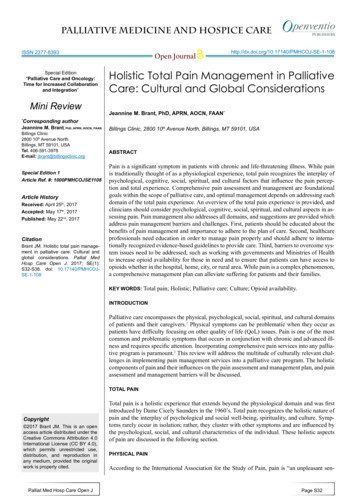
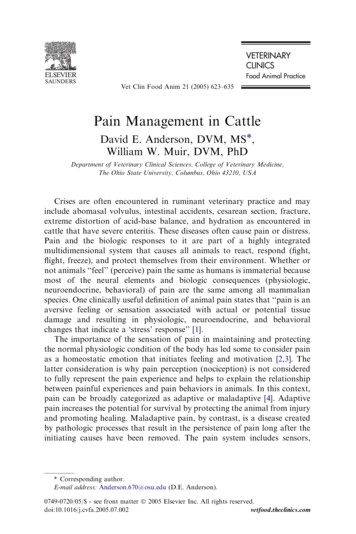
624ANDERSON & MUIRneural pathways, and processing centers [5]. This conglomeration of neuralelements is responsible for detecting, transmitting, and actualizing biologicand behavioral responses to noxious events (Fig. 1). Understanding thephysiologic and pathophysiologic processes responsible for pain and itsconsequences (stress, distress, sickness response) is key to restoring normalphysiologic (homeostatic) pain responses and the development of rationalpain therapies [6,7].Use of drugs to treat pain can produce unwanted side effects, includingbut not limited to disorientation, abnormal behavior, cardiorespiratory andimmunologic depression, and a generalized ‘‘sickness’’ response. Drugtherapy for pain or distress must be considered in the context of overall casemanagement to optimize the patient’s quality of life, restore function, andminimize adverse events. In ruminants, this must be done in consideration ofdrug residues and in accordance with the Animal Medical Drug Use andClarification Act [8,9].Fig. 1. Physiologic (nociceptive) pain: noxious stimuli is tranduced, transmitted, modulated,projected, and perceived. The brain also generates responses that travel by way of descendingnerve pathways that facilitate or inhibit (modulate) sensory input to the spinal cord.
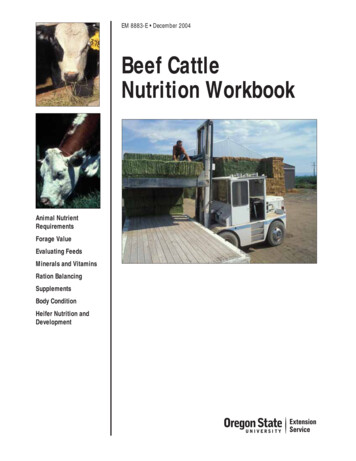
PAIN MANAGEMENT IN CATTLE625Perception of painPhysiologic or ‘‘ouch’’ pain uses normal sensory pathways and serves toprotect the animal from tissue damage [7]. High-threshold pain receptors(nociceptors) located on the endings of afferent thinly myelinated orunmyelinated Ad and C nerve (pain) fibers encode noxious stimulidepending on the modality, intensity, duration, and location of the stimulus.The noxious stimulus is translated into electrical impulses that aretransmitted to the dorsal horn of the spinal cord resulting in the releaseof glutamate from presynaptic nerve terminals. Glutamate activates postsynaptic a-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA)and kainate (KA) receptors [3]. The AMPA and KA receptors are theprimary mediators of fast excitatory pain transmission. In the absenceof tissue damage, pain is considered to be ‘‘physiologic,’’ warning theanimal of potentially harmful stimuli. Pathologic pain is considered to bepresent when tissue or nerve damage occurs and frequently involves thedevelopment of peripheral sensitization, central sensitization, and disinhibition (Fig. 2) [5]. Tissue damage and the associated inflammatory responseassociated with it produce various chemicals that function as nociceptoractivators or sensitizers and include hydrogen and potassium ions,prostaglandins, histamine, bradykinin, nerve growth factor, cytokines, andchemokines. Together these factors act as a ‘‘sensitizing soup,’’ changinghigh-threshold nociceptors to low-threshold nociceptors and activatingquiescent ‘‘silent’’ or ‘‘sleeping’’ nociceptors resulting in peripheral sensitization and a zone of primary hyperalgesia (see Fig. 2) [5,10]. Localvasodilation, and plasma extravasation results in a further amplification ofthe inflammatory response and the spread of hypersensitivity to surroundingtissues (secondary hyperalgesia). When tissue injury is severe Mgþ2 isdisplaced from the normally Mgþ2 blocked N-methyl-D-aspartate(NMDA) receptors located in on dorsal horn neurons (Fig. 2) [4,5]. Theactivation and modulation of NMDA receptors (NMDARs) by theexcitatory neurotransmitter glutamate is believed to be a key componentin the development of central sensitization, secondary hyperalgesia and painamplification [5]. Sensitization of dorsal horn neurons can last for hours andis believed to be responsible for pain outside the area of tissue injury(secondary hyperalgesia) and allodynia (pain from nonpainful stimuli).During various disease states, increases in dorsal horn sensory neuronexcitability is also contributed to by the production of sensitizing substances(eg, prostaglandins) by glial cells in response to increases in cerebrospinal(CSF) cytokines (TNFa, IL-1) [10–12]. Central sensitization is fundamentally different from peripheral sensitization in that, with time, low-intensitynonpainful stimuli carried by low threshold Ab sensory nerve fibers begin toproduce painful sensations. Central sensitization increases the responsiveness (hyperalgesia, allodynia) of dorsal horn neurons to sensory inputs,expands receptive fields, and is believed to be responsible for the discomfort
626ANDERSON & MUIRFig. 2. Pathologic pain: peripheral sensitization, central sensitization, structural reorganization,and disinhibition are several of the more prominent mechanisms responsible for development ofmoderate, severe, and chronic pain conditions.and agony produced by severe injury. The extension of central sensitizationfrom the spinal cord to the brain leads to the development or modificationof memory patterns and is responsible for changes in animal behavior.Severe or continuous pain leads to biochemical (transcriptional) changes indorsal horn neurons promoting the development of chronic pain statescaused by changes in the neurons (neuroplasticity) phenotype [5,11–14]. Thedevelopment of peripheral sensitization, wind-up, and central sensitizationrepresent a continuum of the pain process, which exists as consequence ofcontinuous, unrelenting, and untreated pain.
PAIN MANAGEMENT IN CATTLE627Stress and distressPain is responsible for stress and can lead to distress [15,16]. Stress is anadaptive pattern of behavioral, neural, endocrine, immune, hematological,and metabolic changes directed toward the restoration of homeostasis. Thestress response prepares the animal for an emergency reaction and fosterssurvival in circumstances of immediate threat (fight or flight). Acute painis capable of producing a significant stress response by initiating activationof the sympathetic nervous system, secretion of glucocorticoids (primarilycortisol), hypermetabolism, sodium and water retention, and alteredcarbohydrate and protein metabolism [17–19]. The maintenance of normalhomeostatic balance to an acute stress producing event (pain) is maintainedby negative feedback controls. These controls act at multiple levels within thebrain (amygdala), sympathoadrenal and hypothalamic-pituitary-adrenalaxes thereby elevating catecholamines and glucocorticoids and leading toenhanced arousal, appraisal, cardorespiratory and cognitive performance todeal with the immediate threat. Increased corticotrophin releasing hormone,plasma cortisol and vasopressin often directly correlate with the degree ofstress or pain and help to restore homeostasis. Significant or prolonged painresulting in severe stress, however, eventually becomes maladaptive, producing depression and immunosuppression (sickness syndrome), which, ifnot controlled, can lead to distress and the activation of self-sustainingcascades of neural and endocrine responses that derail physiologichomeostasis [20]. Prolonged stress impairs the animal’s ability to interact,learn and, as stated earlier, changes the animal’s behavioral phenotype [1].Severe pain produces behavioral, autonomic, neuroendocrine, and immunologic responses that can result in self-mutilation, immune incompetence, anda poor quality of life potentially leading to gradual deterioration and death.Apparent anxiety may be observed in ruminants. This form of ‘‘painfree’’ distress may adversely affect the animal’s response to therapy [21,22].Anxiety states are most commonly observed in cattle that experience limitedor adverse human contact (eg, a beef heifer with a dystocia that has not beenhandled since calfhood or beef neonates that are abruptly separated fromthe dam). Anxiety states are frequently observed in cattle that are isolated installs or a hospital environment. Anxiety from social isolation is commonamong species like sheep, llamas, and alpacas with intense herd instincts buthas also been observed among dairy cattle and goats. Use of anxiolyticdrugs in these circumstances may provide as a result more satisfactoryeffects than analgesic drug therapy alone.Emergency management of painThe intensity and duration of the painful stimulus is of great importancein selecting drugs for pain treatment. For example, musculoskeletal pain
628ANDERSON & MUIRmay be approached differently for a cow presented for sole abscess andseptic arthritis of the distal interphalangeal joint compared with the moreacute pain of a fracture. In chronic foot disease, it is much more difficult togain ‘‘control’’ of pain perception because the adaptive pain response makesthe cow less responsive to ‘‘acute’’ pain therapy. Alternatively, a cowpresenting with an acute fracture is likely to respond more favorably to drugadministration. The intensity and duration of pain are vital to drugresponse. Analgesic therapy given after the onset of pain may be less potentand have a shorter duration of effect at equivalent doses. Thus, ‘‘preemptive analgesia’’, which refers to administration of drug therapy, oftenmultimodal therapy, in anticipation of pain rather than in response torecognition of pain is expected to be more effective.The easiest type of pain to treat is that which we induce. The magnitudeof surgical pain is influenced by the procedure, the methods used, and theexperience and skill of the practitioner. Some strategies to minimize painbefore it occurs (eg, pre-emptive) are obvious: local anesthesia, generalanesthesia, sedation, and tranquilization. Careful assessment of cardiovascular status and hemodynamic balance must be done during the drugselection process. Drugs that adversely effect homeostasis or that may becounterproductive in management of shock should not be used to addresspain. Some thought should be given to the physiologic processes that areinduced by tissue injury and may lead to ‘‘pathologic’’ pain after surgery.Sedatives, tranquilizers, narcotics, and anesthetics inhibit detection orintensity of pain by interfering with pain pathways, but these drugs do nottreat the processes (eg, inflammation) to stop continued noxious stimuli.Thus, nonsteroidal anti-inflammatory (NSAIDs) drugs are a critical link tomultimodal therapy of pain. Often, a surgical stimulus (eg, castration incalves) is so brief that little difference can be observed or measured betweenanimals having or not having local anesthesia applied; however, NSAIDscan provide prolonged post operative analgesia with a quantifiable benefit.Analgesic therapyPain management in critical patients often is done using a multimodalapproach. Multimodal therapy refers to use of a combination of drug classesand routes of administration to obtund or prevent pain. Drug treatmentmost commonly used in ruminants includes local anesthesia, epiduralanesthesia, nonsteroidal anti-inflammatory drugs, transdermal analgesia,and continuous infusions.Local anesthesiaLocal anesthetics are the most common pre-emptive analgesic drugs usedin food animal practice [23]. These drugs, especially lidocaine HCl 2%, areused to prevent incisional pain during surgery. These drugs act locally, or
PAIN MANAGEMENT IN CATTLE629regionally when perineural anesthesia is performed, but have no systemic orbehavioral effect. Local anesthetics block nerve fibers (B-fibersOC-fibersOA-fibers) [24]. These nerve-fiber types represent: B ¼ motor/touch; C ¼nonmyelinated ¼ pain/temp sensation; and A ¼ motor/proprioceptive. Theacuteness or severity of the perception of pain is influenced by the stimulus andperception diminishes pain / cold / warmth / touch / deep pressure.Local anesthetic drugs act by inhibiting Na-channels to impede nervedepolarization and conduction and must disassociate in an alkalineenvironment for this to occur. In infected, ischemic, or injured tissues, thequality of local anesthesia is often poor because the more acidic environmentprevents disassociation of drug (eg, septic cellulitis associated withcomplicated sole ulcer complex in dairy cows). The acidic environmentassociated with the cellulitis may no allow local administration of lidocaineto be effective for continued pain sensation. One solution to this problemis to administer the ‘‘block’’ remote to infected tissues. Lidocaine HCL 2%is painful in and of itself, but this noxious characteristic can be eliminatedby adding sodium bicarbonate to neutralize the solution.Local anesthetics can be used in a variety of techniques, including surfaceactive, local block, ring block, selected peripheral nerve block, and regionalblocks (eg, paravertebral, epidural). The authors have used topicalapplication of local anesthetic drugs, including lidocaine spray and lidocainesustained release pads. The topical sprays, designed for application onhuman skin, failed to provide sufficient anesthesia to obtund the response toneedle insertion for paravertebral blocks. Bovine skin, especially dorsal skin,may be too thick or resistant to absorption of the anesthetic to induce localanesthesia. Lidocaine sustained-release patches were designed for topical usein humans for relief of isolated pain. These patches release lidocaine overa period of 12 to 24 hours. The authors prospectively evaluated thesepatches in cows after cruciate ligament surgery, septic arthritis, andincisional pain. Results were highly variable, but most cows showedminimal detectable improvement.Epidural anesthesiaEpidural anesthesia has been the focus of many research projects in cattlethat attempt to minimize the pain o f surgery [25–31]. Caudal epiduralanesthesia is easily applied in cattle and various drugs have been shown tobe beneficial (Table 1). Lidocaine HCl 2% can be used for perineal analgesia(low volume: !1 mL/50 kg body weight) or pelvic and abdominal analgesia(high volume: O1 mL/kg). High volume epidurals using lidocaine have thedisadvantage of ataxia and loss of motor control of the rear limbs. Thesedrugs are advantageous because they have no cardiovascular effect.Several other drugs have been used for epidural analgesia in cattle. Ofparticular interest are drugs, such as alpha-2 agonists. These drugs causeanalgesia by stimulation of alpha-2 receptors that cause inhibition of
630ANDERSON & MUIRTable 1Usage of epidural anesthesia for paralumbar analgesia or laparotomy in cattleDrugDosageOnset of analgesiaDuration ofanalgesiaLidocaine 2%Xylazine0.2 mg/kg (5 mL)0.05 mg/kg(5 mL in saline)0.07 mg/kg1.0 mg/kg2–3 mg/kg dilutedto 8 mL in saline5 minutes20–40 min10–115 min2–3 h2 mg dose: 19 min2 mg dose: 192 min3 mg dose: 9 min3 mg dose: 311 minpeak effect during60–180 min5 mL: 17 min10 mL: 34 min20 mL: 62 min45 to 127 minmean, 83 min412 minClonidineKetamine 5%Procaine hcl 5%MedetomidineDetomidineRomifidineþ morphine5 mL (250 mg)10 mL (500 mg)20 mL (1000 mg)300 mg (6 mL)5 mL: 6.5 min10 mL: 5 min20 mL: 5 min8–20 min15 mg/kg (5 mL)40 mg/kgR: 50 mg/kg5 min12 h maximumM: 0.1 mg/kgAbbreviations: M, morphine; R, romifidine.norepinephrine and substance P release. These drugs may optimize analgesiabut minimize motor nerve interference such that the patient may remainstanding and stable throughout surgery. Use of alpha-2 agonists underemergency conditions is discouraged because the risk for profoundcardiovascular instability or recumbency exceeds the benefits observedwith the use of these drugs.Opioids have been commonly used for epidural analgesia in humans,horses, and dogs. These drugs have been used in cattle with variable clinicalresults. Opioids inhibit neurotransmitter release and increase potassiuminflux into the neuron thus hyperpolarizing the membrane. Morphine maybe the most common opioid used for epidural analgesia but has not resultedin profound analgesia in ruminants (Table 2) [32]. In our clinical use ofepidural morphine for postoperative analgesia in fracture management orseptic arthritis patients, convincing efficacy does not exist despite promisingresearch trials in cattle [27].Nonsteroidal anti-inflammatory drugsNSAIDs inhibit cyclo-oxygenase enzyme (COX). COX acts on arachidonic acid to liberate prostaglandins and other mediators of inflammation.COX inhibitors prevent production of these factors. Nonspecific COXinhibitors include flunixin, ketoprofen, and phenylbutazone. Selective COX-
631PAIN MANAGEMENT IN CATTLETable 2Opioids used for analgesia in ruminantsDrugDoseRouteFrequencyMorphine0.5–1 mg/kg0.05–0.1 mg/kg3.3–4.4 mg/kg0.005 mg/kg (sheepand goats)0.05 mg/kgIV epiduralq 12 hq 24 hMeperidineBuprenorphineButorphenolSC or IMIMq 12 hSCq6hAbbreviations: IV, intravenous; q, every; SC, subcutaneous.Data from Jenkins WL. Pharma cologic aspects of analgesic drugs in animals: an overview.J Am Vet Med Assoc 1987;191:1231–40.2 inhibitors are rapidly evolving and include etodolac and carprofen. TheNSAIDs may have different effects because of the presence of variablereceptors. Clinical observations suggest that flunixin meglumine providesexcellent visceral analgesia but has less potent effects for many musculoskeletal injuries. Alternatively, phenylbutazone seems to provide excellentmusculoskeletal pain relief but offers little benefit for treatment of visceralpain. The authors have used etodolac for several years for management ofchronic musculoskeletal pain in ruminants. Their clinical experiencesuggests that, although COX-2 drugs may be safer for long-term usebecause they are less likely to interfere with homeostasis of abomasalmuscosa or renal perfusion, they are less potent analgesics (Table 3).Much of the pain research has shown tremendous benefits of pre-emptiveanalgesia. A consistently, less impressive effect of administration ofanalgesic medication exists after the noxious stimulus has becomeestablished. Zulauf and colleagues [33] showed that if NSAIDs wereadministered before Burdizzo castration, during the first 72 hours, lowerserum cortisol, greater feed intake, and less scrotal swelling resulted.Stafford and colleagues [34] compared various surgical castration techniques(ring versus band versus surgery versus clamp) with or without localanesthesia or NSAIDs. Local anesthesia alone did not prevent cortisol rise,but local anesthesia plus NSAIDs did obtund the response. Mellor andcolleagues [35] showed a marked increase of cortisol and noradrenaline afterTable 3Nonsteroidal anti-inflammatory drugs used in ruminantsDrugDoseRouteFrequencySalysilic acid (Aspirin)Flunixin meglumineKetoprofenPhenylbutazone100 mg/kg1 mg/kg2 mg/kg5 mg/kg10 mg/kgPOIVIVPOPOqqqqqAbbreviations: IV, intravenous; PO, per OS (by mouth); q, every.1212122448hhhhh
632ANDERSON & MUIRcastration, dehorning, and tail amputation that was obtunded as long aslocal anesthesia was present. Dehorning calves 4 to 8 weeks of age withsedation and local anesthesia was only beneficial when combined with anNSAID [36]. In another setting, local anesthesia of the cornual nerve,whereas dehorning calves was more effective than sedation with xylazineand butorphanol in lowering serum cortisol and heart rate [37]. In yetanother study examining pain with scoop dehorning, long-acting (3–4hours) local anesthesia with bupivicaine obtunded the cortisol response incalves when local anesthesia was present [38].Age of cattle does not seem to have as profound an effect on the stress ofminor surgical procedures as it does in swine. Taschke and Folsch [39]examined dehorning stress in calves from birth to 4 months. Age had noeffect but anesthesia significantly reduced cortisol and other adverseresponses. Eicher and colleagues [40] showed increased activity andincreased heat sensitivity distal to the band for about 2 hours after taildocking in calves 3 to 5 weeks of age. Ruminants, especially cattle, differ inbehaviors associated with pain. Ruminants often become subdued, spendmore time lying down, less time eating and ruminating, and fail to clean thenostrils as frequently when in pain or stressed. Galindo and colleagues [41]observed that lame cows had more lying time, less eating time, more lyingtime outside of cubicles, performed fewer aggressive behavior actionsdespite having the same frequency of receiving aggressive behaviorinteractions. These lame cows were licked more by other cows but lickedother cows less. Many social and environmental factors influence painperception and responses in cattle. Whay and colleagues [42] reported thatheifers developed hyperalgia in the peri-parturient period. Rushen andcolleagues [43] showed that cows subjected to social isolation, with orwithout naloxone therapy, had increased vocalization, heart rate, andcortisol while demonstrating other signs consistent with hypoalgesia orstress-induced analgesia.Continuous infusion analgesiaAnalgesic drugs may be administered by continuous intravenous or localinfusion. Recently, constant rate infusion (CRI) units have becomeavailable. These infusion units include a pressure bulb that can be filledwith the solution of choice infused at a set rate but limited only by diameterof the tubing used. The infusion system used most commonly by the authorsis the ‘‘Pain Buster,’’ which, when filled with a sufficient quantity of drug toadminister over a 24-hour period, delivers 2 or 4 mL of solution per hour.The CRI analgesic infusions have been used to provide extremely smalldoses of a drug combination designed to provide a balanced multimodalapproach. Filling the system once daily, a Holstein cow being treated forchronic septic arthritis of the flexor tendon sheath in the authors’ hospitalis given a combination of an antibiotic (ceftiofur, 10 mL), analgesic drug
PAIN MANAGEMENT IN CATTLE633(lidocaine, 10 mL), and saline (40 mL) at the rate of 2 mL/h. In a Holsteinheifer with second-degree burns over 40% of her body from a trailer fire, theCRI provided morphine, ketamine, and lidocaine until the heifer becamemore comfortable, began ruminating normally, and was able to lie downand rise more easily.SummaryCertainly, many advances in drug therapy are being made. Food animalveterinarians are partly responsible for the preservation of a safe foodproduct. To that end, caution must be practiced with cross-species applications of drugs and therapies. What is the cost-benefit relationship? Basedon the available literature, the single most important tool available inmodern veterinary medicine is pre-emptive analgesia. Veterinarians mustcapture ‘‘opportunities’’ to prevent the onset of pain, prevent noxiousstimuli or their perception, and limit the pain-stress-distress cascade thatresults in altered behavior and deviation from physiologic norms. Rationaltreatment of pain requires an appreciation of its consequences, a fundamental understanding of the mechanisms that are responsible for its production,and a practical appreciation of the analgesic drugs available. The goal ofpain treatment should be to restore normal (physiologic) pain responses andto eliminate pathologic pain processes. In this context, pain therapy shouldbe directed at the multiple mechanisms (mutilmodal therapy) responsiblefor its production and analgesic therapies should be instituted before(preemptive therapy) pain is initiated (eg, surgery) whenever possible [7,21].References[1] Broom DM. The evolution of pain. Vlaams Diergeneeskundig Tijdschrift 2000;69:385–411.[2] Craig AD. Pain mechanisms: labeled lines versus convergence in central processing. AnnuRev Neurosci 2003;26:1–30.[3] Craig AD. Interoception: the sense of the physiological condition of the body. Curr OpinNeurobiol 2003;13:500–5.[4] Woolf CJ. Pain: moving from symptom control toward mechanism-specific pharmacologicmanagement. Ann Intern Med 2004;140:441–51.[5] Muir WW, Woolf CJ. Mechanisms of pain and their therapeutic implications. J Am Vet MedAssoc 2001;219(10):1346–56.[6] Carstens E, Mober GP. Recognizing pain and distress in laboratory animals. ILAR J 2000;41(2):62–71.[7] Scholz J, Woolf CJ. Can we conquer pain? Nature 2002;5(Neuroscience Suppl):1062–7.[8] Sundlof SF. Legal and responsible drug use in the cattle industry: extra-label use. Vet Med1998;93:673–80.[9] Hunt SP, Mantyh PW. The molecular dynamics of pain control. Nat Rev Neurosci 2001;2:83–91.[10] Woolf CJ, Slater MW. Neuronal plasticity: increasing the gain in pain. Science 2000;288:1765–9.[11] Julius D, Basbaum AI. Molecular mechanisms of nociception. Nature 2001;413:203–10.
634ANDERSON & MUIR[12] Watkins LR, Milligan ED, Maier SF. Glial activation: a driving force for pathological pain.Trends Neurosci 2001;24:450–5.[13] Woolf CJ, Shortland P, Coggeshall RE. Peripheral nerve injury triggers central sprouting ofmyelinated afferents. Nature 1992;355:75–8.[14] Moore KA, Koho T, Karchewski LA, et al. Partial peripheral nerve injury promotesa selective loss of GABAergic inhibition in the superficial dorsal horn of the spinal cord.J Neurosci 2002;22:6724–31.[15] Clark JD, Rager DR, Calpin JP. Animal well-being. I. General Considerations. Lab AnimSci 1997;47(6):564–70.[16] Clark JD, Rager DR, Calpin JP. Animal well-being. II. Stress and distress. Lab Anim Sci1997;47(6):571–85.[17] Carr DB, Goudes LC. Acute pain. Lancet 1999;353:2051–8.[18] Desborough JP. The stress response to trauma and surgery. Br J Anaeasth 2000;85(1):109–17.[19] Weissman C. The metabolic response to stress: an overview and update. Anaesthesia 1999;73:308–27.[20] Chapman CR, Gavin J. Suffering: the contributions of persistent pain. Lancet 1999;353:2233–7.[21] Benson GJ, Thurmon JC. Species difference as a consideration in alleviation of animal painand distress. J Am Vet Med Assoc 1987;191:1227–30.[22] Woolf CJ, Max MB. Mechanism-based pain diagnosis: issues for analgesic drugdevelopment. Anesthesiology 2001;95:241–9.[23] Muir WW, Hubbell JAE, Skarda R, et al. Local anesthesia in cattle, sheep, goats, and pigs.In: Muir WM, Hubbell JAE, Skarda R, Bednarski RM, et al, editors. Handbook ofveterinary anesthesia. 2nd edition. St-Louis (MO): Mosby; 1995. p. 53–77.[24] Muir WW, Hubbell JAE, Skarda R, et al. Local anesthetic drugs and technques. In: MuirWM, Hubbell JAE, Skarda R, et al, editors. Handbook of veterinary anesthesia. 2nd edition.St-Louis (MO): Mosby; 1995. p. 39–52.[25] St-Jean G, Skarda RT, Muir WW, et al. Caudal epidural analgesia induced by xylazineadministration in cows. Am J Vet Res 1990;51:1232–6.[26] Caron JP, LeBlanc PH. Caudal epidural analgesia in cattle using xylazine. Can J Vet Res1989;53:486–9.[27] DeRossi R, Bucker GV, Varela JV. Perineal analgesic actions of epidural clonidine in cattle.Vet Anesth Analg 2003;30:64–71.[28] Lee I, Yoshiuchi T, Yamagishi N, et al. Analgesic effect of caudal epidural ketamine in cattle.J Vet Sci 2003;4:261–4.[29] Fierheller EE, Caulkett NA, Bailey JV. A romifidine and morphine combination for epiduralanalgesia in the flank in cattle. Can Vet J 2004;45:917–23.[30] Prado ME, Streeter RN, Mandsager RE, et al. Pharmacologic effects of epidural versusintramuscular administration of detomidine in cattle. Am J Vet Res 1999;60:1242–7.[31] Lin HC, Trachte EA, DeGraves FJ, et al. Evaluation of analgesia induced by epiduraladministration of medetomidine to cows. Am J Vet Res 1998;59:162–7.[32] Jenkins WL. Pharmacologic aspects of analgesic drugs in animals: an overview. J Am VetMed Assoc 1987;191:1231–40.[33] Zulauf M, Gutzwiller A, Steiner A, et al. The effect of a pain medication in bloodlesscastration of male calves on the concentrated feed intake, weight gain and serum cortisollevel. Schweiz Arch Tierheilkd 2003;145(6):283–90.[34] Stafford KJ, Mellor DJ, Todd SE, et al. Effects of local anaesthesia or local anaesthesia plusa non-steroidal anti-inflammatory drug on the acute cortisol response of calves to fivedifferent methods of castration. Res Vet Sci 2002;73(1):61–70.[35] Mellor DJ, Stafford KJ, Todd SE, et al. A comparison of catecholamine and cortisolresponses of young lambs and calves to painful husbandry procedures. Aust Vet J 2002;80(4):228–33.
PAIN MANAGEMENT IN CATTLE635[36] Faulkner PM, Weary
pain can be broadly categorized as adaptive or maladaptive [4]. Adaptive pain increases the potential for survival by protecting the animal from injury and promoting healing. Maladaptive pain, by contrast, is a disease created by pathologic processes that result in the persistence of pain long after the initiating causes have been removed.