Transcription
Protect, promote, and improve the health and prosperityof people in Tennessee.Healthy People, Healthy Communities,Healthy onRespect
This report provides an overview and evaluation of the TDH-supported County HealthAssessment pilot conducted with 16 rural County Health Councils in 2019.SectionPageTable of Contents3County Health Assessment Overview4Vital xt Steps173
Tennessee’s County Health Councils werelocally-led needs assessment process. The CHAestablished in the 1990’s as a way to bringguides Health Council members through datatogether community partners from differentcollection and review to determine up to threesectors to utilize local data and pursue commonpriorities for the County Health Council to addresssolutions for shared issues. More than twothrough cross-sector collaboration.decades later, these groups continue to buildrelationships, share resources, and promote work The Tennessee Department of Health completedthat enhances community health and well-being.a pilot CHA process January-July, 2019. Sixteencounties representing each of TDH’s 7 ruralHealth Councils exist in all 95 counties with TDHregions participated in the pilot. Through thisdirectly supporting those councils in the 89 ruralprocess, each county brought together diversecounties through funding and staffing support.stakeholders to look at data, identify disparities,Because County Health Councils are representedand select up to three priority areas to work on.by a diverse set of stakeholders in positions ofBuilding on local expertise and communityinfluence, they are ideal groups for facilitatingengagement, and with a focus on vulnerableconversations across sectors, connecting andpopulations, the CHA was able to drivecollaborating with stakeholders and decision-collaborative action on upstream drivers ofmakers on effective policies and systems changes, health.County Health Assessment Goalsconducting county health assessments toestablish shared priorities, and implementingcollaborative action plans to address those1. Increase overall stakeholder engagement andparticipation in Health Council meetings/activitiespriorities. While membership and mission ofCounty Health Councils may vary from county tocounty, typical sectors represented include2. Support local leadership by providing CountyHealth Councils with structure, support, andresources aimed at identifying and addressingcommon prioritieseducation, planning, local government, healthcare, mental health, juvenile justice, local nonprofits, social service organizations, andcommunity members.3. Facilitate the development of 3-year actionplans for each County Health Councilparticipating in the CHA processThe County Health Assessment (CHA) aims toincrease the impact of existing Health Councils by4. Provide a platform to integrate and align localand state-level strategic planningproviding a framework for councils to conduct a4
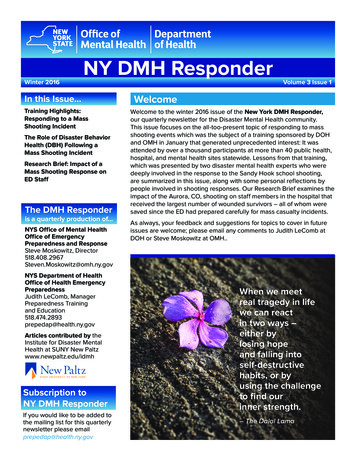
2019 CHA Pilot Counties by RegionWest RegionMid-Cumberland erlandRegionDeKalbFentressNortheast RegionHancockWashingtonSouth Central RegionSoutheast RegionEast he 16 pilot counties were selected by Regionalvalues, counties were able to observe where theyand County Leadership based on a number ofmight have the most room for improvement.factors including staffing levels, Health Councilcapacity, and alignment with existing assessmentIn the third and fourth months, counties designedcycles such as those of local non-profit hospitals.and implemented a primary data collection plan,Regional Leadership were asked to select 2-3conducted interviews and listening sessions, andcounties from each region to participate in theoccasionally distributed surveys to better learnCHA pilot. The East and West regions eachabout perceived strengths and opportunitiesconducted the CHA in three counties, while thewithin the community. In the final months, HealthMid-Cumberland, South Central, UpperCouncils reviewed and summarized the secondaryCumberland, Southeast, and Northeast regionsand primary data. This allowed them to prioritizeeach selected two counties to participate.up to three issues to guide their action planningfor the next three years.During the CHA process, Health Councils metmonthly, with each month’s meeting including aFinally, the Health Councils designed an actionspecific set of tasks. During the first month,plan based on local assets and gaps in order tocounties identified and engaged their team. In the address the priorities selected in their CHAsecond month, counties reviewed a list ofprocess. These plans will guide Health Councilavailable local data including Tennessee’s Vitalactivity in the upcoming months and years.Signs (see page 6) and other measures related toMoving forward, Health Councils will complete thehealth and wellness. By doing this and comparing CHA every three years with about one-third ofthe county-level data with state and nationalcounties completing the CHA each year.5
Tennessee’s Vital Signs are 12 metrics selectedthat priority. Each Vital Sign Action guide containsthrough an extensive public engagement processfour areas of focus including programming,meant to measure the pulse of Tennessee’sfunding opportunities, policy recommendations,population health. Taken together, they provideand community education & awarenessan at-a-glance view of leading indicators of healthcampaigns. While counties are not required toand prosperity. Tennessee’s Vital Signs includeselect from the Vital Signs, the impactful naturetraditional health metrics such as substance useof these indicators was evident in the array ofand physical activity. However, they also includepriorities identified by CHA pilot counties. Nearlymetrics related to social determinants of health,88% of the identified priorities following the CHAsuch as per capita personal income, access topilot were aligned with one of Tennessee’s 12parks and greenways, and 3rd grade reading level. Vital Signs (43 of 48) and all of the pilot countiesAs part of the CHA, counties review data related to prioritized at least one of the Vital Signs. TDH iseach of these indicators and are encouraged tocontinuing to develop online resources forconsider the impact of each on their community.Health Councils to find local data, utilizeFor counties that identify one of the 12 Vital Signsresources, and identify and implementas a CHA priority, TDH has developed an extensive community interventions for each of the Vitalmenu of evidence-informed strategies, known asSigns. This and more information aboutVital Sign Action Guides. These guides can helpTennessee’s Vital Signs can be found online atHealth Councils identify opportunities to addresswww.tn.gov/VitalSigns.6
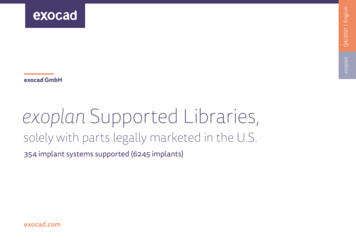
As a result of the data collection and review that CHA pilot counties participated in, Health Councilmembers voted on their top priorities to address over the next 2-3 years. The most commonlyidentified priority area was related to Drug Overdose, followed by Frequent Mental Distress &Obesity. Priorities are displayed below by county.Bradley CountyGibson CountyHenry CountyStewart CountyChester CountyGiles CountyMarshall CountyTrousdale CountyDeKalb CountyHamblen CountyMeigs CountyUnion CountyFentress CountyHancock CountyMonroe CountyWashington CountyOtherBradley - Access to Affordable Health CareChester - Lack of ChildcareMarshall - Minority HealthMonroe - Cardiovascular HealthWashington - Community Violence (SchoolSafety, Domestic Violence, Child/Elder Abuse,and Sexual Assault)7
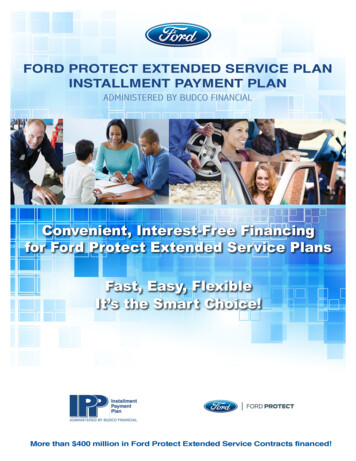
Evaluation of the CHA pilot was conducted by theHealth Council/Community MemberTDH Office of Strategic Initiatives using bothTDH Staffquantitative and qualitative methods captured inREDCap. A survey link was distributed to HealthCouncil members and TDH staff participating inthe pilot. Respondents had approximately four34 Responsesweeks to complete the evaluation survey, and allresponses remained anonymous.200Total SurveyResponses183CompletedSurveys145Participated inthe CHA111 ResponsesRespondents self-identified as either a HealthCouncil/Community Member or TDH Staff. Logicbranching was used to filter questions specific toTDH staff related to the utility of the resources/worksheets provided by the CHA team, as well asother questions specific to implementation of theCHA in relation to existing TDH programs. Thesurvey tool filtered out responses unique to thosethat participated in the CHA process compared tothose who may be on a listserv but do not activelyattend meetings to gauge communication aroundthe CHA. In addition, individuals had the option tovoluntarily identify the county they represented orsupported.8
The CHA evaluation survey had four main parts: CHA Process/Outcome Questions, CHA Resources Utility, CHA SupportNeeds, and Open-Ended Questions. Most questions wereframed on a Likert Scale and recoded using Microsoft Excel sothat ‘Strongly Agree’ 5, ‘Agree’ 4, ‘Neutral’ 3, ‘Disagree’ 4,94%of respondents Strongly Agreed or Agreedthat they enjoyed participating in theCHA with their Health Council.and ‘Strongly Disagree’ 1.Mean Response for Process/Outcome QuestionsQ1I enjoyed participating in the County Health Assessmentprocess with my Health Council.4.43Q2The County Health Assessment added value to the workof my Health Council.4.41Q3The County Health Assessment increased participantengagement during the Health Council meetings.4.30Q4The County Health Assessment increased the averageattendance of my Health Council meetings.3.71Q5The County Health Assessment process attracted newand important stakeholders who were previously not partof our Health Council.3.72Q6The County Health Assessment process providedguidance for my Health Council in identifying priorityhealth issues.4.42Q7The County Health Assessment process helped my HealthCouncil engage with low-income, under-served, orminority populations.3.5890%of respondents Strongly Agreed or Agreedthat the CHA added value to the work oftheir Health Council.88%of respondents Strongly Agreed or Agreedthat the CHA increased engagementduring Health Council meetings.96%of respondents Strongly Agreed or Agreedthat the CHA provided guidance for theHealth Council.9
Engaging with Minority and otherCounties reporting increased engagementwith underserved or minority populationsidentified the following specific groups:Underserved PopulationsThirty-four respondents representing 14different counties identified a minority or otherunder-served population they included orconsidered in their CHA. Some respondentsidentified multiple groups. Survey participantswere given an open-response field to indicatewhich group(s) they worked with and collectivelyidentified 14 different minority or vulnerablegroups.Several of the open-ended responses providedinsight towards opportunities for furtherengaging these populations, including alternatemeeting times, more purposeful engagement,alternative forms of primary data collection suchas town hall meetings, and recruiting additionalOther includes: African-Americans, LGBTQ, Veterans, Homeless,Underinsured, Immigrants, Non-English Speaking, SingleParents, Incarcerated, and Those Suffering from Addiction.community members to participate in theprocess.Primary Data CollectionAll 16 counties included in the CHA pilot choseto do additional primary data collection.12counties reported doing local surveys as partof their Primary Data Collection.Counties were given three options for collectingprimary data (Local Surveys, Key Informant12Interviews, and Focus Groups/ListeningSessions) and could use as many or as few asthey felt were necessary. Seven countiesimplemented all three data collection strategiesat some level and seven elected to takecounties reported conducting key informantinterviews as part of their Primary Data Collection.advantage of two strategies. Focus groups/listening sessions were the most commonly13reported strategy for primary data collection.40% of those reporting their Health Councilcollecting primary data ‘Strongly Agreed’ that theprimary data was helpful in understanding andselecting priorities while 60% ‘Agreed.’counties reported doing a focus group or listeningsession as part of their Primary Data Collection.10
CHA ResourcesTDH staff were asked to evaluate how helpfulWorksheet Descriptionsprovided resources were in conducting theWorksheet 1.1 Establish Your Point of ContactCHA, with ‘5’ being the most helpful and ‘1’Worksheet 1.2 List all Members of Your Health Councilbeing the least helpful. Staff could select ‘0’ ifthey did not use a particular resource. TheWorksheet 1.3 Invite Others Into the Processmean response for each resource is shownWorksheet 1.4 CHA Team Developmentabove. Staff rated the County Data Package,Worksheet 2.1 Review Vital Signs & Key Health SignalsCounty Demographic Profile, and the associatedWorksheet 2.1 Review Vital Signs & Key HealthWorksheet 2.3 Small Group DiscussionSignals the most useful. The Sample SurveyWorksheet 2.4 Key Informant InterviewsQuestions were also highly rated. InWorksheet 2.5 Develop a Primary Data Collection Plancomparison, the least useful resources wereidentified as Worksheet 3.2 Find Your PeerWorksheet 3.1 Review Existing AssessmentsCounties, and the VSA Selection Tool, with theWorksheet 3.2 Find Your Peer Countiesmean response for each below 2.5. ResourcesWorksheet 3.3 Multi-Voting Processthat were most frequently identified as notbeing used included Worksheet 3.2 Find YourWorksheet 4.1 Inventory for VSA SelectionPeer Counties, the VSA Selection Tool, andWorksheet 4.2 Identify Potential Vital Sign ActionsWorksheet 1.4 CHA Team Development.11
CHA Support NeedsBoth Health Council/Community Members and TDH staff members were asked to identify areas ofthe CHA where they could most benefit from additional support, where ‘5’ Most Additional SupportNeeded and ‘1’ Least Additional Support Needed. Overall results are shown below, as well assegmented results by Health Council/Community Members and TDH staff.Please identify the areas where you could benefit from additional support.OverallHealth Council/Community MemberTDH StaffOverall, the areas where additional support would be of most benefit were in Implementing InterventionStrategies, Selecting Intervention Strategies, and Developing Action Plans to Address Priorities. On average,Health Council/Community Members rated Implementing Intervention Strategies as the area of mostneed while TDH staff identified Selecting Intervention Strategies as the most important.Conversely, both Health Council/Community Members and TDH Staff both rated Facilitating Meetingsas the area needing the least support, followed by Reviewing the County Data Package.These results illustrate a general satisfaction with the application of the guidance for conducting CHAHealth Council meetings but suggest that the guidance itself could be improved, particularly for thosemeetings later in the CHA process. Qualitative feedback aligned with these results as interviews withTDH staff consistently highlighted additional guidance needed around actions to address prioritiesonce they are identified.12
Open-Ended QuestionsThe CHA Evaluation survey included four open-ended questions aimed at providing a deeperunderstanding of the impact of the CHA, as well as to give participants the opportunity to addressstrengths or opportunities that may not have been identified by other questions. A thematic reviewof the responses for each question was conducted, and frequencies for each overarching theme areshown below. In addition, selected comments have been included for reference.Selected comments: “What did you likemost about the CHA process?”“The cohesiveness that it provided for ourmembers. With this process, I saw a degreeof cooperation and participation that Ihave not seen, ever, with this group.”General- Process“Bringing more stakeholders to the tablethat did not regularly attend Health Councilmeetings.”Collaboration withOther SectorsIncreased Engagementof Health CouncilProvided Resources &Information“The CHA process was well laid out. Itprovided us the opportunity to explore ourareas of successes and to identify areas forimprovement.”Refocusing the HealthCouncil“It allowed our Health Council to refocus onour priorities within the counties.”“Opened my eyes to serious issues in ourcounty and gave us tools to work towardssolving/improving these issues.”Selected comments: “What did you likeleast about the CHA process?”“I feel like more time may have beenneeded. Everyone works and the councilmet 1x a month.”“Part of me wishes we could have gonethrough the process a little faster, but itworked well how it was laid out.”“We talked and talked more about thingswe could do, but we never settled in onanything or decided what are the nextsteps.”“Items with small print that made readinghard.”“I believe our data needed more input fromthe general community - not justcommunity leaders.”Timeline/ScheduleGeneral- ProcessFormat of ResourcesNot FeelingPrepared/SupportedLack of DiversityOtherNothing/Positive13
Selected comments: “How could theCHA process be improved?”“Helping the health departments in acohesive way to blend the CHA and PPI.Give counties ample time to formulate agood plan after the CHA process.”General- ProcessIncrease ParticipantDiversity“Inclusion of more diverse people in theprocess.”CHA Timeline“Include different dates and times to collectmore feedback from a diverse population.”Meeting Schedule“6 months is a quick turn around—moretime I think would be helpful!”Data Format/Delivery“This process needs to be shortened. Maybea few sessions could be combined. . .”Nothing/Positive“Have the data for the county analyzed withproblem or troubling areas identified, aswell as positive areas, and then start theprocess from there.”Selected comments:“Are there any additional comments youwould like to provide?”“Our Health Council is pretty active and theassessment just helped us more clearlylabel our focus with new terms.”“Thanks for making the CHA possible. It hasreally brought a group together and givenus more of a focus and ‘purpose’ formeeting.”“Great process to assist counties indetermining priority health issues!”“Maybe more talking points for meetingspecific. . . Having more communication inthat sense about what’s been working incounties during the process.”“The support from Central Office wasoutstanding. Many resources wereprovided. The initial training for staffregarding the CHA process was wellplanned.”General- PositivePositive - CentralOffice SupportGeneral- SupportConcernsCounty-LevelIndividualRecognition14
Overall feedback from both the evaluation surveymeetings highlight how the CHA improvedand one-on-one conversations with participantsengagement and participation during meetings.throughout the CHA pilot w positive andaddressed each of the goals laid out for theCounty Health Assessment. Both Health Council/Community Members and TDH staff expressedenjoyment and benefit from participating in theCHA. Specifically, Health Council/CommunityMembers overwhelmingly demonstratedGoal 2: Support local leadership by providingCounty Health Councils with structure, support,and resources aimed at identifying andaddressing common priorities.As a result of the CHA pilot, all 16 participatingCounty Health Councils identified three priorityappreciation of the CHA process, as evidenced byareas to focus on for the next 2-3 years, and 96%survey.feedback was particularly indicative the CHA wasthe many positive comments received through the (n 138) of responses indicated the CHA providedguidance in identifying priorities. Qualitativeopen-ended questions portion of the evaluationeffective in achieving this goal. Multiple responseshighlighted how the CHA brought additionalstakeholders to the table, as well as how theprocess pushed them to look at priority areasoutside of their traditional scope of work. Whenasked about the level of support and resourcesprovided, both Health Council/CommunityMembers and TDH staff agreed the structure andformat was an overall effective structure forGoal 1: Increase overall stakeholder engagement leading Health Councils through the CHA.and participation in Health Councils.Goal 3: Facilitate the development of 3-yearBoth quantitative and qualitative feedback suggest action plans for each County Health Councilparticipating in the CHA process.the CHA was effective in increasing the overallstakeholder engagement and participation duringHealth Council meetings. 88% of respondentseither ‘Strongly Agree’ or ‘Agreed’ (n 129) thatparticipant engagement in Health Councilmeetings increased as a result of the CHA.Conversely, only 3.5% (n 5) ‘Disagreed’ and 8.5%(n 11) were ‘Neutral’. Several of the open-endedresponses from Health Council members andfeedback taken from TDH staff in one-on-oneOnce counties have identified priorities, CountyHealth Councils are encouraged to work with theirlocal health department team to develop an actionplan that outlines how the Health Council willaddress those priorities over the next three years.Due to the timing of the CHA pilot, many of thepilot Health Councils are still in the process ofdeveloping their action plans, and although the15
development of these plans is still in progress,Several key themes emerged from the evaluationmany of the open-ended comments received onand throughout the pilot regarding opportunitiesthe evaluation survey highlighted Health Councilto improve the CHA process and make it bothmembers’ awareness and desire to ensure follow- more effective and efficient for Health Councilsup accountability related to their identifiedand local health departments.priorities.Clarification on the Planning Process andAction Plan Follow UpGoal 4: Provide a platform to integrate and align The most frequently provided feedback from TDHlocal and state-level strategic planningstaff members related to clarification andUsing the CHA as a platform to integrate and alignlocal and state-level strategic planning is a long-additional guidance needed for the CHA HealthCouncil Action Plan and its relation to existinghealth department programs such as Primaryterm goal of the CHA. The CHA pilot provided anPrevention. Staff from the Office of Strategicopportunity for this to begin by working toInitiatives is working closely with the Office ofintegrate the CHA with Primary Prevention andPrimary Prevention to develop more robustCounty Performance Plans. Once action plansguidance around the interaction of these twohave been developed for each of the 16 pilotplans and identify opportunities to clarifycounties, those priorities and activities can beexpectations related to their interaction. The CHAconsidered in the overall strategic planningTrainings being held in Fall 2019 will addressprocess for the Department.these concerns, and ongoing guidance willcontinue to be provided as updates aredetermined.TimelineFeedback related to the overall six month timelinewas varied. Some responses indicated that theprocess could have been completed in less thensix months, while others said they would havepreferred a longer process. Overall, this reinforcesOpportunities for Improvementthe guidance that meeting schedules are flexibleThe evaluation also provided important feedbackand each county should move through therelated to opportunities for improvementsuggested activities at their own pace.regarding the structure, support, and overallIn contrast, a general consensus was establishedprocess of the CHA. This feedback is being usedby the Office of Strategic Initiatives to enhance theoverall CHA process and streamline suggestedactivities, as well as to identify opportunities tointegrate locally identified priorities into theoverall strategic planning process for theDepartment.related to the suggested timeline of activitieswithin the six month time frame. The CHA team iscurrently exploring ways to adjust the suggestedtimeline of activities within the six month windowso that priorities can be established earlier andmore time can be dedicated to the actionplanning and implementation phases.16
TDH staff recognized the level of support andguidance received as one of the key factors in thesuccess of the CHA pilot. However, they alsoexpressed that increased support and guidancewould be most beneficial upon completion of theCHA as Health Councils and local healthdepartments work to identify and implement VitalInclusion of Minorities/Vulnerable Populations Sign Actions and other strategies. This support isReview of the CHA process by external partnersnecessary for the continued success of the CHA.and internal stakeholders, as well as feedbackfrom internal stakeholders and pilot participants,highlighted the need for greater diversity andinclusion of minority and other vulnerableIn 2020, Health Councils in 27 counties will bepopulations throughout the CHA process. Inconducting a County Health Assessment. Ofresponse, the Office of Strategic Initiatives isparticular interest, this includes 11 of the 13reviewing opportunities to incorporate additionaleconomically distressed counties, as defined byguidance on best practices for including thesethe Appalachian Regional Commission, that werepopulations in the CHA worksheets and othernot included in the CHA pilot (Fentress andprovided resources. In addition, suggestions forHancock Counties participated in the pilot).engaging these populations taken from theTrainings will be held in November andevaluation survey (such as the potential to holdDecember.CHA meetings at various times/places toaccommodate challenging schedules, having townhall forums to gather qualitative feedback, etc.)will be incorporated into the suggested guidancefor future County Health Assessments.General Process/Provided ResourcesThe 16 pilot counties will continue to work on thedevelopment and implementation of their actionplans to address their priorities. The activities andstrategies being implemented will be tracked byTDH and the Office of Strategic Initiatives withplans to share this information publicly on theThe most common feedback regarding the overall TDH County Health Assessment website. BeyondCHA process and the associated resources wascontinued development of the aforementionedrelated to the data package and it’s presentation.website, TDH and the Office of Strategic InitiativesWhile most individuals reported satisfaction withis working internally to identify opportunities tothe current format, several participants expressed strengthen and support County Health Councilsinterest in more visuals and assistance inacross the state. These efforts are being led inanalyzing both secondary and primary data.collaboration with partners such as the Office ofOpportunities to clarify some indicators andPrimary Prevention, the division of Communitypresent more meaningful data to localHealth Services, and local & regional stakeholders.stakeholders is a primary focus of the 2020 CHA.Additionally, the utility of the worksheets andother resources (see Page 11) will be consideredfor future CHA processes.For more information regarding Tennessee’sCounty Health Councils, the CHA, or Vital SignActions, please visit www.tn.gov/VitalSigns.17
Office of Strategic Initiatives Tennessee Department of HealthEric HarknessDirectorJW Randolph, MPHPolicy AnalystJonathon G. Smith, MPHCHA CoordinatorEmma ZijlstraCommissioner’s FellowCrystal LemusCommissioner’s FellowStrategy.Health@tn.govLearn more at www.tn.gov/VitalSigns18
Vital Signs (43 of 48) and all of the pilot counties prioritized at least one of the Vital Signs. TDH is continuing to develop online resources for Health Councils to find local data, utilize resources, and identify and implement community interventions for each of the Vital Signs. This and more information about