Transcription
University of GroningenIron status and heart failureKlip, IJsbrand ThomasIMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.Document VersionPublisher's PDF, also known as Version of recordPublication date:2016Link to publication in University of Groningen/UMCG research databaseCitation for published version (APA):Klip, IJ. T. (2016). Iron status and heart failure: From prediction to prognosis. Rijksuniversiteit Groningen.CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: ing-pure/taverneamendment.Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.Download date: 06-07-2022
ChapterSerum ferritin andrisk for new onsetheart failure andcardiovascular eventsin the communityIJsbrand T. KlipAdriaan A. VoorsDorine W. SwinkelsStephan J.L. BakkerJenny E. Kootstra-RosCarolyn S. LamPim van der HarstDirk J. van VeldhuisenPeter van der MeerAccepted Eur J Heart Fail 20165
AbstractAims:Heart failure (HF) is a common manifestation of patients with primary andsecondary causes of iron overload, whereas in patients with establishedHF iron deficiency impairs outcome. Whether body iron, either depleted orin overload, amplifies the risk for new onset HF among healthy individualsis unknown. The present study aimed to assess whether markers of ironstatus, or iron-regulatory hormone hepcidin are associated with new onsetHF or cardiovascular (CV) events in the general population.Methods and results:In 6386 subjects from the Prevention of REnal and Vascular ENd-stageDisease (PREVEND), a prospective, community-based, cohort study, markers of iron status and iron-regulatory hormone hepcidin were measured.Mean age was 53.1 12.0 years and 50.7% of the cohort was female. Duringa mean follow-up of 8.3 years, 199 subjects (3.1%) were newly diagnosedwith HF, 456 (7.1%) experienced a CV event and 356 died from all causes.A higher annual HF incidence per ferritin quartile was observed in women(P 0.001), but not in men (P for interaction 0.032). Multivariable analysesdemonstrated ferritin levels to remain independently predictive for newonset HF in women only (P 0.024). This association persisted within stratadefined by markers of the metabolic syndrome, markers of inflammationor other markers of iron homeostasis, including hepcidin. No associationbetween ferritin or hepcidin and incident CV events or all-cause mortalitywas observed in either sex.Conclusions:Increased serum ferritin levels independently amplify the risk for new onsetHF in women in the community. Studies need to elucidate the pathophysiological mechanisms through which ferritin levels associate with specificoutcomes.100
Iron markers and new onset heart failure in the VHMIPREVENDROSTSATUAE body mass indexcardiovascularheart failureheart failure with preserved ejection fractionheart failure with reduced ejection fractionhigh-sensitive C-reactive proteinleft bundle branch blockleft ventricular hypertrophymyocardial infarctionPrevention of REnal and Vascular ENd-stage DiseaseReactive oxygen speciesTransferrin saturationurinary albumin excretion5101
IntroductionIron is an essential micronutrient for a wide range of metabolic and biological processes. Systemic iron homeostasis is orchestrated by hepcidin,a liver-derived peptide that has emerged as the key circulating regulatorof iron absorption and tissue distribution.1 In response to low body ironstores, decreased erythropoiesis and hypoxia, hepcidin levels decrease allowing efficient iron mobilization. In contrast, inflammation and increasedbody iron stores cause excessive hepcidin production, which subsequentlyinhibits intestinal iron absorption and iron release from reticuloendothelialmacrophages.1In patients with primary and secondary causes of iron overload, cardiomyopathy is a common manifestation.2 In contrast, severe iron deficiencyhas also been associated with abnormalities in systolic and diastolic cardiacfunction, suggesting an U-shaped relationship between body iron storesand the process leading to heart failure.3,4 Prior epidemiological studieshave proposed an association between increasing body iron stores (mostlyexpressed as serum ferritin levels) and risk for cardiovascular (CV) diseasein the general population, whereas others have found conflicting results.5Likewise, the role of hepcidin as a risk modifier in cardiovascular disease isalso controversial.6,7Whether markers of iron status, either depleted or in overload, or regulatory hormone hepcidin predict the risk of new onset heart failure (HF)among healthy individuals is unknown. Therefore, we aimed to determinewhether markers of iron homeostasis antedate the development of HF andcardiovascular outcome. For these purposes, we used data obtained in thePrevention of REnal and Vascular ENd-stage Disease (PREVEND) study, alarge prospective, well-characterized, contemporary observational cohortwith a long-term follow-up period.MethodsThis study was performed using data of subjects participating in the PREVEND study. Details of the study protocol have been published elsewhere(www.prevend.org).8 In brief, from 1997 to 1998, all inhabitants of the city ofGroningen, The Netherlands, aged 28-75 years, were sent a questionnaire ondemographics, disease history, smoking habits, use of medication, and a vialto collect an early morning urinary sample (n 85,421). Of these subjects,40,856 responded (47.8%). After exclusion of subjects with type 1 diabetes102
Iron markers and new onset heart failure in the communitymellitus (defined as the use of insulin), and pregnant women, subjects withan urinary albumin excretion (UAE) 10 mg/L (n 6000) and a randomlyselected control group with an UAE 10 mg/L (n 2592) completed the protocol and formed the baseline PREVEND cohort (n 8592). For the currentanalyses we used data from the second survey, which took place between2001 and 2003 (n 6894), as hepcidin and iron measurements were onlyavailable from this time period. We excluded 508 subjects due to missingferritin or hepcidin values, and missing follow-up data, leaving 6386 subjects for the current analysis. The PREVEND study was approved by theinstitutional medical ethics committee and conducted in accordance withthe Declaration of Helsinki. All subjects provided written informed consent.Definitions & calculations5Blood pressure was calculated as the mean of the measurements of thetwo study visits of the second survey. Hypertension was defined as systolicblood pressure 140 mmHg, diastolic blood pressure 90 mmHg, or selfreported use of antihypertensive medication. Body mass index (BMI) wascalculated as the ratio of weight and height squared (kg/m2), and obesitywas defined as a BMI 30 kg/m2. Hypercholesterolemia was defined astotal serum cholesterol 6.5 mmol/L (251 mg/dL), a serum cholesterol 5.0 mmol/L (193mg/dL) when a history of myocardial infarction (MI) waspresent or when lipid-lowering medication was used. Type 2 diabetesmellitus was defined as a fasting glucose level of 7.0 mmol/L (126 mg/dL), a non-fasting glucose level of 11.1mmol/L (200 mg/dL), or the use ofanti-diabetic drugs. Smoking was defined as current smoking or smokingcessation within the previous year. Urinary albumin excretion was calculated as the average UAE in the two consecutive 24-h urine collections. Anestimate of the glomerular filtration rate was calculated using the ChronicKidney Disease Epidemiology Collaboration (CKD-EPI) equation.9 Historyof myocardial infarction or stroke was defined as a self-reported conditionrequiring hospitalization for at least 3 days. Anemia was defined accordingto the World Health Organization (WHO) criteria (hemoglobin 13 g/dL formen and 12 g/dL for women).10 Standard 12-lead electrocardiograms wererecorded using the computer Modular ECG Analysis System.11 The presenceof a left bundle branch block (LBBB) was defined as a QRS duration on ECG 120msec. Left ventricular hypertrophy (LVH) was defined using the Cornellcriteria: RaVL SV3 (with 6mm added in women) multiplied by the QRSduration. A threshold of 2440 mm*ms was used to identify LVH.12103
Analytical methodsFasting blood samples were obtained in the morning from all participantsfrom 2001-2003. Aliquots of these samples were stored immediatelyat -80 C until further analysis. Hemoglobin (g/dL) was measured usinga Coulter Counter STKS sum (Coulter Corporation, Miami, Florida, USA).Serum iron (umol/L), ferritin (ug/L) and transferrin (g/L) were measuredusing a colorimetric assay, immunoassay and immunoturbidimetric assay,respectively (Roche Diagnostics, Mannheim, Germany). The total iron binding capacity was calculated by multiplying transferrin x 25.2. Subsequently,transferrin saturation (TSAT [%]) was computed by dividing serum iron byTIBC and multiplied by 100. Serum hepcidin concentrations were measuredwith a competitive enzyme-linked immunosorbent assay, as described elsewhere.13 The between-plates and inter-assay coefficient of variation (CV)were 8.6% and 16.2%, respectively. Hepcidin concentrations are expressedin nanomoles per liter (nmol/L). Concentrations of total cholesterol, plasmaglucose and serum creatinine were measured using standard methods.Urinary albumin concentration was determined by nephelometry, with athreshold of 2.3 mg/L and intra- and interassay CV of 2.2 and 2.6%, respectively (BN II, Dade Behring Diagnostica, Marburg, Germany). High-sensitiveC-reactive protein (hs-CRP) was also determined using nephrelometry witha threshold of 0.175 mg/L and intra- and interassay coefficients of less than4.4 and 5.7% respectively.Definition of cardiovascular events and new onset heart failureFollow-up for the present study was defined as the time between the firstfollow-up visit to the outpatient department and the date of a CV event, newonset HF, death, or January 1st 2011. Subjects were censored on the date theymoved to an unknown destination or at the last date of follow-up (January 1st2011), whichever date came first. Information on dates and causes of deathfor every participant was obtained from Statistics Netherlands and codedaccording to the 10th revision of the International Classification of Diseases.14The combined incidence of CV morbidity and mortality after the secondsurvey was used. Information on hospitalization for CV morbidity was obtained from PRISMANT, the Dutch national registry of hospital dischargediagnoses, which has proven validity with 84% of the primary diagnosis and87% of the secondary diagnosis matching those recorded in the patients’charts.15 In the present study, CV events were defined as the following:acute MI (ICD-code 410), acute and subacute ischaemic heart disease (411),subarachnoid haemorrhage (430), intra-cerebral haemorrhage (431), otherintra-cranial haemorrhage (432), occlusion or stenosis of the pre-cerebral104
Iron markers and new onset heart failure in the community(433) or cerebral arteries (434), coronary artery bypass grafting or percutaneous transluminal coronary angioplasty, and other vascular interventionsas percutaneous transluminal angioplasty or bypass grafting of aorta andperipheral vessels.Participants with a new diagnosis of HF were identified using criteriadescribed in the Heart Failure Guidelines of the European Society of Cardiology and an endpoint adjudication committee ascertained the diagnosisof HF, as described elsewhere.16 Additionally, HF was classified as HF witha reduced (HFrEF) or preserved ejection fraction (HFpEF) based on theleft ventricular ejection fraction at the time of diagnosis. To acknowledgethe most recent trends in cut-off for HFrEF and HFpEF in accordance withthe most recent HF guidelines, we set the cut-off for HFpEF at 50%.17 Inall subjects developing new onset heart failure in the present study data onLVEF was available.Baseline continuous variables are expressed as means with standard deviation (SD) when normally distributed, as medians with interquartile range(IQR) when distribution is skewed, or as numbers and percentages whencategorical. Inter-group differences were tested using trend-analyses. Forfurther analyses, skewed variables were transformed to a 2-log scale toachieve a normal distribution.By design, the PREVEND study over-selected subjects with an elevatedUAE ( 10mg/L). To overcome this over-selection of subjects with UAE, astatistical weighted method was applied in our regression analyses, allowing our conclusions to be generalized to the general population.18,19 The association of ferritin with baseline variables was examined by bootstrappingthe linear regression model 1000 times. Variables selected 700 times wereassumed to be accurate and included in the multivariate model.Overall and sex-stratified adjusted annual incidence rates of new onsetHF, CV events, and all-cause mortality were assessed assuming a Poissondistribution. The test for trend was calculated using the Mantel-Haenszelmethod. To preserve ferritin (and hepcidin) as continuous variables, multivariable fractional polynomials were employed to determine the best fittingfunctional form of both markers for all outcome parameters. To account fordeath as a competing risk for new onset HF, a subject’s follow-up time wascensored at the time of death whenever death occurred before the onset ofHF. Hazard ratios are then interpreted as the covariate effects on the causespecific (sub)hazard function of the transition from heart failure-free tonew onset HF in a competing risks model with new onset HF and all-cause5Statistical analyses105
mortality as the two absorbing states.20 Crude analyses were consecutivelyadjusted for 1) age and sex; 2) a multivariate model consisting of the following established HF and CV risk factors: age, sex, BMI, current smoking,diabetes, hypertension, hypercholesterolemia, history of MI or stroke, LVH,renal function, and levels of hemoglobin, erythropoietin, UAE, and presenceof inflammation (hs-CRP 5 mg/L); and 3) time-varying development of CVevents. Similar analyses were done for incident CV events and all-causemortality. All reported probability values are two-tailed and a value of P 0.05 was used as the nominal level of statistical significance. Models andanalyses were performed using STATA software version 13.0 (StataCorp LP,College station, Texas, USA).ResultsBaseline characteristics of the 6386 subjects, stratified per ferritin quartiles,are displayed in Table 1. Mean age was 53.1 12.0 years and 50.7% of thecohort was female. Median ferritin concentration was 97 (47 - 173) ug/L andwas higher in men (142 ug/L) compared to women (61 ug/L; P 0.001). Irondeficiency, defined by ferritin levels 30ug/L, was present in 928 subjects(14.5%) and more frequently observed in women (24.6% vs. 4.2% in men;P 0.001). Although postmenopausal women had significantly higher ferritin levels in relation to their premenopausal counterparts (94 ug/L vs. 36ug/L; P 0.001), iron deficiency was still more frequently seen when compared to men (8.7% vs. 4.2% in men; P 0.001).Per increasing ferritin quartile, individuals were generally older, moreoften male, and more likely to have cardiovascular risk factors (e.g. diabetes,hypertension). Additionally, higher concentrations of hemoglobin, hs-CRP,TSAT and hepcidin were observed, whereas renal function worsened andEPO concentrations declined. Baseline ferritin quartiles were additionally stratified by sex (Table S1A&1B). Similar results were detected for bothsexes, with the exception of prior MI and the presence of either LBBB orLVH, which were more frequently observed in women.Clinical associates of ferritin levelsIn both sexes, serum ferritin remained positively correlated with hemoglobinand MCV, other markers of iron homeostasis and glucose concentrations.Whereas ferritin was strongly related to cardiovascular risk factors (BMI,cholesterol) in men, inflammation and decreasing erythropoietin levelswere correlated with ferritin levels in women (Table 2). In a bootstrapped106
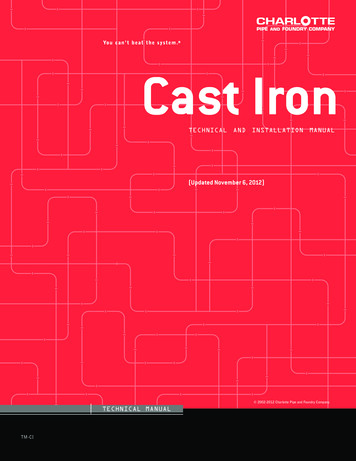
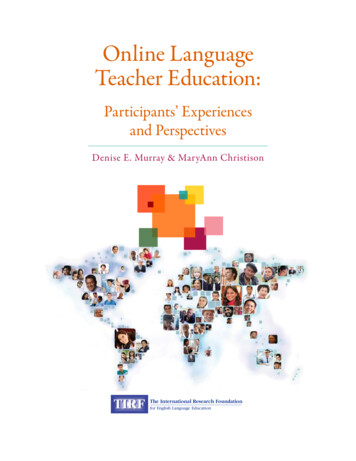
Iron markers and new onset heart failure in the communitymodel for ferritin (per doubling), these variables were highly selected. Thepresence of LVH (a strong HF risk factor) or LBBB was associated with ferritin levels in women (but not in men) in univariable regression only (TableS2). The multivariable model in women had a better model fit compared tomen (Table 2). Similar cardiovascular risk factors related to ferritin levels inmen and women without prior CV disease and adjusted R2 was comparable(Table S3).Markers of iron homeostasis and new onset heart failure.After a median follow-up of 8.3 (7.8-8.9), years, 199 individuals (3.1%) werediagnosed with new onset HF, 456 (7.1%) experienced a CV event and 356(5.6%) died from all-causes. Compared to other markers of iron status, ferritin had the best accuracy in predicting incident HF and other events (FigureS1). The adjusted annual incidence of new onset HF rose per increasing fer-5Figure 1. Total annual incidence of new onset heart failure according to ferritin (1A) and hepcidin(1B) quartiles and stratified by sex.107
percholesterolemia2.9Type 2 diabetes30.4Smoking or quit 1 yearMIMedical history (%)2.25.8LVH according to Cornell (%)68.5 10.0Heart rate (b.p.m.)LBBB (%)126.3 18.818.726.7 4.350.753.1 12.020.919.115.85.00.92.029.73.41.068.9 9.4119.5 17.112.725.5 4.382.048.3 10.927 (1–48)638697 (1–1925)Q1TotalSystolic BP (mmHg) 30 (%)BMI (kg/m2)Female sex (%)Age (years)Clinical signsFerritin (ug/L), min-maxnVariablesTable 1. Baseline characteristics according to ferritin quartiles.7.227.824.16.31.12.532.84.82.368.4 10.3125.0 18.715.526.2 4.356.653.3 12.071 (49–97)1579Q25.034.426.67.80.63.131.07.12.268.4 10.0128.5 18.119.126.9 4.240.554.6 11.7130 3 10.3132 18.627.628.1 4.123.156.4 11.7257 (173–1925)1595Q4 0.001 0.001 0.001 0.0010.68 0.0010.19 0.0010.0010.022 0.001 0.001 0.001 0.001 0.001NANAP - valuefor trend
3.27.8 (5.7–12.4)7.9 (5.8–13.9)5.589.9 17.683.4 16.94.7 (4.4–5.2)5.4 1.01.3 (0.6–2.9)7.7 (5.9–10.1)25.0 8.316.0 5.22.6 (1.8–3.5)90.7 4.113.7 1.1Q258.5 (6.1–16.0)6.788.2 17.486.5 19.05.0 (4.5–5.4)5.5 1.01.4 (0.7–3.2)7.5 (5.7–9.7)25.8 8.416.1 5.13.8 (2.8–5.1)90.8 4.214.0 1.1Q310.0 (6.7–20.3)7.786.2 17.790.4 23.65.1 (4.6–5.6)5.6 1.11.8 (0.8–3.6)7.3 (5.5–9.7)28.2 9.617.2 5.55.6 (4.2–8.0)91.3 4.414.3 1.1Q4 0.001 0.001 0.001 0.001 0.001 0.001 0.001 0.001 0.001 0.001 0.001 0.001 0.001P - valuefor trendContinuous variables are presented as mean standard deviation or as median (inter-quartile range) when non-normally distributed. Binary categorical variables are presented aspercentages. Abbreviations: BMI Body mass index, BP Blood pressure, eGFR Estimated glomerular filtration rate, hs-CRP high-sensitive C-reactive protein, LBBB Left bundlebranch block, LVH Left ventricular hypertrophy, MCV Mean corpuscular volume, MI Myocardial infarction, TSAT Transferrin saturation, UAE Urinary albumin excretion.8.5 (6.0–15.1)5.7UAE (mg/24h) 60 (%)94.1 17.1eGFR (ml/min/1.73m2)78.9 14.184.8 19.189.6 17.7Creatinine (umol/L)4.6 (4.3–5.1)4.8 (4.4–5.3)5.1 1.01.0 (0.4–2.3)8.6 (6.5–12.0)20.6 9.5Glucose (mmol/L)5.4 1.01.4 (0.6–3.0)Cholesterol (mmol/L)7.8 (5.9–10.3)24.8 9.4TSAT (%)Erythropoietin (IU/L)15.9 5.6hs-CRP (mg/L)1.1 (0.6–1.7)3.1 (1.7–4.9)Hepcidin (nmol/L)Serum iron (umol/L)14.1 6.388.9 5.313.7 1.290.4 4.612.9 1.2Q1Hemoglobin (g/dL)TotalMCV (fL)Laboratory measurementsVariablesTable 1. Baseline characteristics according to ferritin quartiles. (continued)Iron markers and new onset heart failure in the community109
Table 2. Multivariable regression beta-coefficients between cardiovasular risk factors and serumferritin in men and women (selected after bootstrapping).Variables (selected afterbootstrapping)Menstruation (yes vs. no)BMI (per kg/m2)Smoking (yes vs. no)Women(n 3241)Men(n 3145)StandardizedßTPvalue---0.0905.4-- 0.001-Standardized ßT 0.129 7.4-- 0.035 2.6Pvalue 0.0010.011Hemoglobin (per g/dL)0.1086.5 0.0010.0714.1 0.001MCV (per fL)0.0996.0 0.0010.1247.6 0.001Log 2 hepcidin (nmol/L)0.68038.6 0.0010.62530.4 0.001TSAT (per 5%)0.0945.1 0.0010.1315.7 0.001--- 0.031 2.0-0.0593.5--0.0524.4Log 2 erythropoietin(IU/L)Log 2 hs-CRP (mg/L))--Cholesterol (mmol/L)0.0442.50.011Log 2 glucose (mmol/L)0.0433.6 0.001R2 total model0.60R2 total model0.042 0.001 0.0010.74For abbreviations, see Table 1.ritin quartile (Figure 1). This trend only appeared to be significant in women(P 0.001). Crude and multivariable fractional polynomials revealed theassociation between ferritin levels and the development of new onset HFto be best described by a linear function. In subsequent Cox regressionanalyses (with all-cause mortality as a competing risk) increasing ferritinconcentrations were strongly associated with the development of newonset HF (P 0.001; Table 3) However, this association was lost in multivariable analyses. Interaction analyses showed a significant interaction betweensex, ferritin levels and new onset HF (Pint 0.032). When stratified by sex, thisassociation persisted only in women (P 0.001) and remained significantin all multivariable models. Adjusting for menstrual status did not alter theresults. No interaction between menstrual status, ferritin levels and development of new onset HF was found in women (P 0.59). Additional subgroupanalyses in women demonstrated increasing ferritin levels to amplify risk forincident HF in almost every subgroup, but were significantly more predictive in women without anemia, without microalbuminuria and with an eGFR 60 ml/min/1.73m2.(Figure S2).Since body iron stores are firmly regulated at the systemic level by hepcidin, we additionally explored the role of hepcidin and risk of new onset HF.Similar observations regarding adjusted annual HF incidence were made forhepcidin, both overall and in women (Figure 1). Likewise, a strong associa-110
Iron markers and new onset heart failure in the communityTable 3. Levels of ferritin and hepcidin and risk for incident heart failure with all-cause mortalityas a competing risk.Ferritin (per doubling)sHR95%CIHarrell’s CP-value1Total population (n 6386)Univariable1.481.30–1.690.64 0.001Model 11.241.05–1.460.830.011Model 21.060.89 – 1.260.880.45Men (n 3145)Univariable1.000.81–1.230.520.98Model 11.060.87–1.290.820.54Model 20.920.75–1.140.870.45 0.001Women (n 3241)Univariable2.071.63–2.610.74Model 11.571.20–2.050.830.001Model 1A1.691.26–2.260.79 0.0011.351.02–1.790.870.038Model 31.391.05–1.860.870.024HR95%CIHarrell’s CP-valueHepcidin (per doubling)5Model 2Total population (n 6386)2Univariable1.451.23–1.720.61 0.001Model 11.200.98–1.450.830.07Model 21.090.92–1.300.880.39Men (n 3145)Univariable0.960.79–1.160.540.76Model 11.000.81–1.250.820.94Model 0.75 0.001Model 11.591.17–2.170.840.003Model 1A1.681.19–2.370.790.003Model 21.441.03–2.050.870.039Model 31.601.09–2.370.880.018Women (n 3241)Abbreviations: CI Confidence interval, sHR Sub-hazard ratio.1P for interaction ferritin, sex and new onset heart failure 0.032.2P for interaction hepcidin, sex and new onset heart failure 0.045.Model 1 is adjusted for age (per 10 years) and sex (in total population).Model 1A is adjusted for menstrual state instead of age.Model 2 is adjusted for model 1 cardiovascular and heart failure risk factors: BMI, current smoking, the presenceof diabetes, hypertension, hypercholesterolemia, history of MI or stroke, LVH, renal function, and levels of hemoglobin, erythropoietin, hs-CRP and UAE.Model 3 is adjusted for model 2 time-varying incident cardiovascular events.111
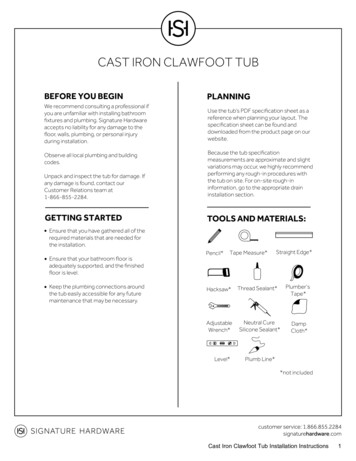
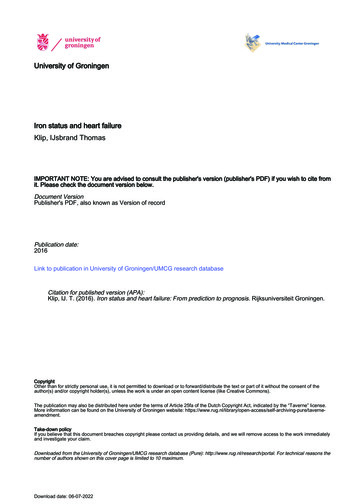
112Figure 2. Sex stratified risk for new onset heart failure according to the joint classification of ferritin levels and tertiles of TSAT (A), hepcidin (B), hs-CRP (C),BMI (D), glucose (E) or systolic blood pressure (F).
Iron markers and new onset heart failure in the community5tion between levels of hepcidin and the development of new onset heartfailure was observed in women only (Pint 0.045). Removing potential outliers (highest and lowest 1%) did not change the results. In subjects withoutprior myocardial infarction and/or stroke, both ferritin and hepcidin levelsremained strongly associated with the development of HF in women (TableS4). Sensitivity analyses in postmenopausal women showed ferritin - andnot hepcidin - to remain predictive for new-onset HF (Table S5).To assess whether the association between body iron stores and risk ofnew onset HF were modified by other markers of iron homeostasis (TSAT,hepcidin), inflammation (hs-CRP) or the metabolic syndrome (BMI, glucose,systolic blood pressure), the joint association of ferritin levels with eitherone of these 6 variables and the development of HF was examined. In thesejoint analyses, ferritin levels remained independently associated with newonset HF in women in almost all stratified analyses.(Figure 2).Finally, 79 of the 199 subjects newly diagnosed with HF were women.Of these women, 37 developed HFrEF and 42 HFpEF. Unadjusted causespecific hazard analyses demonstrated serum ferritin to be associated witheither HFrEF or HFpEF, with no significant interaction between both entities(Table S6). Multivariable analyses showed that levels of ferritin remainedstrongly associated with an increased risk for HFpEF only. However, againno significant interaction was found.Markers of iron homeostasis and risk for cardiovascular diseaseand all-cause mortality.A higher total annual incidence of new CV events and all-cause mortalitywas observed per increasing ferritin and hepcidin quartile (Figure S3). Whenstratified by sex, these observations only persisted in women. Multivariablefractional polynomials again showed the best fitting functional form between levels of ferritin or hepcidin and new CV events to be linear. Cruderegression analyses showed increasing ferritin and hepcidin concentrationsto be both strongly predictive for new CV events and all-cause mortality inthe overall population and in women (both P 0.001). However, age- andmultivariable analyses were non-significant. No interaction between variables was demonstrated.DiscussionIn this contemporary, prospective, population-based cohort, increasingferritin levels amplify the risk for new onset HF in women, but not in men.113
This relationship is independent of established conventional CV and HF riskfactors and the development of CV events over time. These observationsprovide evidence that increased ferritin levels are an independent risk factorfor the development of HF in women and might play a direct or indirect rolein the pathogenic mechanism leading to HF.How do elevated iron stores relate to incident heart failure?Whereas iron deficiency has detrimental effects on outcome in establishedheart failure,17,21,22 the role of iron markers or markers of erythropoiesis in thedevelopment of HF has only been investigated to some extent.23,24 Previousliterature suggested a U-shaped relationship between iron stores and newonset HF.3,4.In the present study, we observed a linear relationship betweenincreasing ferritin levels and the development of HF. Excess body iron isknown to accumulate in organs such as the heart and lead to cardiomyopathy. The generation of reactive oxygen species (ROS) in mitochondriais believed to be the most important pathogenic pathway determiningcardiomyocyte damage. Production of ROS causes lipid peroxidation andDNA damage, leading to cell death, fibrosis, and eventually cardiac dysfunction. However, iron overload is only observed when the binding capacity oftransferrin is fully saturated and non-transferrin bound iron is formed. Interestingly, joint analyses showed an association between serum ferritin andnew onset HF in all TSAT tertiles, suggesting that another pathway linkingincreased ferritin levels with cardiomyocyte damage may also be involved.Iron-mediated cell damage does not only occur under conditions of ironoverload. It has been proposed that iron maldistribution among organs,tissues and cellular compartments can also attenuate cell integrity and celllife. Dysmetabolic hyperferritinemia, meaning elevated ferritin levels withnormal TSAT, is commonly observed in clinical practice and has been associated with insulin resistance, obesity, hypertension, and other manifestationsof the metabolic syndrome.25 During circumstances of subclinical systemicinflammation, iron efflux in organs may be halted due to increased hepcidinproduction and subsequent internalization and degradation of its receptor,iron exporter ferroportin.26 Therefore, elevated ferritin levels (and hepcidin)might be a reflection to a low-grade inflammatory response of anotherpathophysiological process (e.g. metabolic syndrome), causally responsiblefor the development of HF.27 Supporting this hypothesis is the fact that weobserved a posit
Iron is an essential micronutrient for a wide range of metabolic and bio-logical processes. Systemic iron homeostasis is orchestrated by hepcidin, a liver-derived peptide that has emerged as the key circulating regulator of iron absorption and tissue distribution.1 In response to low body iron