Transcription
Menu2021OVERVIEWSmall GroupInsurance CoverageWhy HorizonOMNIA Health PlansHealth Plan BenefitsMedical PlansOMNIA Health PlansAdvantage EPO Health PlansAdvantage Direct Access Health PlansHorizon MyWay Horizon EXPANDDental PlansVoluntary DentalVisionHealth Plus PlanLife & DisabilityInternational MedicalPet InsuranceMedicare AdvantageHorizon Blue AppSeptember 30, 2020September30, 2020 2021 OVERVIEW SMALL GROUP INSURANCE COVERAGE
Menu» Why HorizonNow more than ever, you need healthinsurance you can count on.OMNIA Health PlansHealth Plan BenefitsMedical PlansHorizon Blue Cross Blue Shield of New Jersey(Horizon BCBSNJ) has had decades of experiencehelping New Jersey residents get the most out of theirhealth plans. We can help you and your employeestoo, with plans, tools and resources to better manageyour health care.OMNIA Health PlansAdvantage EPO Health PlansAdvantage Direct Access Health PlansHorizon MyWay Horizon EXPAND Access to New Jersey’s leading doctors, hospitals and health centers Online tools and mobile apps to simplify health care Plans with low copays and low deductiblesDental PlansWe have plans that keep yourcosts low.Voluntary DentalVisionHealth Plus Plan Innovative extras like education resources and healthy living discountsLife & Disability A variety of affordable plans for the coverage your employees needInternational MedicalPet InsuranceMedicare AdvantageDid You Know?1 out of 3 Americans* carry a Blue Cross Blue Shield (BCBS) card, which providesthem with access to the largest network of doctors and hospitals across the U.S.and here in New Jersey.Contact your Broker orHorizon Account Representativeor visit HorizonBlue.com.*BCBS Fact Sheet, July 2020September 30, 2020Why Horizon 2021 OVERVIEW SMALL GROUP INSURANCE COVERAGEHorizon Blue App
MenuWhy HorizonOur OMNIASM Health Plans are nowbetter than ever.» OMNIA Health PlansHealth Plan BenefitsMedical PlansOur newly expanded plans provide even morechoices to help employees save with leadingproviders in New Jersey, New York, Pennsylvania andDelaware. Plus, we have some of the most affordablypriced plans in New Jersey.OMNIA Health PlansAdvantage EPO Health PlansAdvantage Direct Access Health PlansHorizon MyWay Horizon EXPANDOMNIA Health Plans with BlueCard nationwide coverage offer: Low copays and deductibles with OMNIA Tier 1 doctorsand hospitals1Get great service fromdedicated associates whoare experts in OMNIA HealthPlans.Dental PlansVoluntary DentalVisionHealth Plus Plan Access to 90% of doctors and hospitals nationwideLife & Disability Coverage for over 90 percent of the nation’s doctors andhospitals in every U.S. Zip code at the Tier 2 level.2International Medical2Pet InsuranceMedicare AdvantageContact your Broker orHorizon Account Representativeor visit HorizonBlue.com.1. No referrals needed2. Blue Cross and Blue Shield (BCBS) Fact Sheet, July 2020September 30, 2020OMNIA Health Plans 2021 OVERVIEW SMALL GROUP INSURANCE COVERAGEHorizon Blue App
MenuWhy HorizonWe’re here to provide care and supportfrom the comfort of home.OMNIA Health Plans» Health Plan BenefitsMedical PlansOMNIA Health PlansNurse ChatAdvantage EPO Health PlansIt should be easy to get the care you need, especiallywhen you’re not feeling well. If you can’t reach yourprimary doctor, our Nurse Chat feature is just a fewclicks away on our secure member website. You canalso use the Horizon Blue app to chat with a nurseabout your health issues, all without leaving home.1Advantage Direct Access Health PlansTelemedicineWe have more ways to connect with U.S. boardcertified, licensed doctors, via the Horizon Blue app,video, chat or phone, 24 hours a day, seven daysa week.2Horizon MyWay More ways to get care virtually.Dental PlansChronic Care ProgramsThese programs can help employees take control oftheir health by providing support to manage theday-to-day challenges of living with chronic conditions,such as asthma or diabetes.Voluntary DentalVisionHealth Plus PlanLife & DisabilityInternational MedicalPillPackPresorted medicines and home delivery make it easierto take care of your health. You can get your medicinesdelivered to your home from PillPack by AmazonPharmacy, a full-service pharmacy, in user-friendlypackaging at no additional cost to you.Virtual Health & Wellness Programs andResourcesThese live webinars and recorded videos on a varietyof wellness topics can help you ease stress and stayactive.1. Some state and plan restrictions may apply.2. Horizon CareOnline telemedicine functionality within the Horizon Blue app will be available in the 4th quarter of 2020.September 30, 2020Horizon EXPANDHealth Plan Benefits 2021 OVERVIEW SMALL GROUP INSURANCE COVERAGEPet InsuranceMedicare AdvantageHorizon Blue App
MenuWe can help your employees achieve their best health.Why HorizonOMNIA Health Plans» Health Plan Benefits WellnessBehavioral Health & Substance Use DisorderServices such as annual physical and gynecologicalexams, well-baby/child medical care and immunizationsare covered when using an in-network doctor.Care for behavioral health conditions or alcohol/substance use disorder is offered through our extensivenetwork of participating health care professionals whoprovide a full range of counseling services.OMNIA Health PlansAdvantage EPO Health PlansAdvantage Direct Access Health PlansHorizon MyWay Wellness Includes: My Health Manager powered by WebMD (Members may be eligible to earn a 50 Visa prepaid gift card) Healthy Living Discounts with Blue365 Online health educationCase ManagementOur Care Managers help manage complex health caresituations by simplifying navigation, coordinating careand providing a better understanding of policies andprocedures.Horizon EXPANDDental PlansVoluntary Dental PRECIOUS ADDITIONS program for parents-to-beVision HorizonbFitSM gym reimbursement*Health Plus Plan*Included with OMNIA Health PlansPrescription Drug CoveragePrescription drug coverage is an integrated part ofour health plans, helping employees recover from anillness, manage a condition and stay in good health.September 30, 2020Medical PlansHealth Plan Benefits Away From Home CareLife & DisabilityThis program is available to members withoutBlueCard coverage in Horizon HMO, Horizon EPO andOMNIA Health Plans. It gives eligible members accessto participating doctors, facilities and other health careprofessionals throughout the country.International MedicalPet InsuranceMedicare AdvantageHorizon Blue App2021 OVERVIEW SMALL GROUP INSURANCE COVERAGE
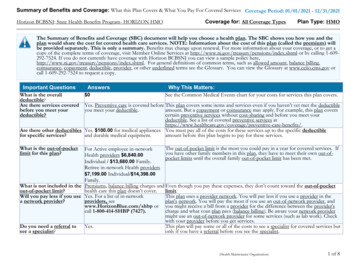
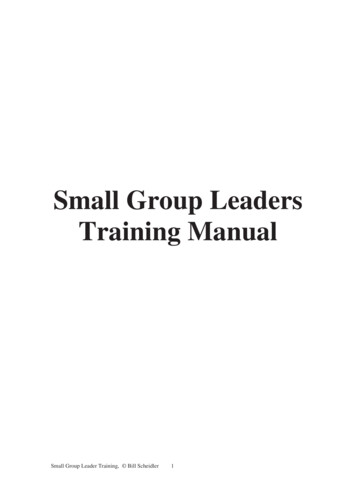
OMNIAHEALTH PLANS2021 Small Group OMNIA Health Plans2021 BENEFITSGENERALPROVISIONSOMNIA PlatinumTier 1Tier 2Tier 1OMNIA Gold with Blue CardTier 2Tier 1MenuOMNIA Gold HSA with BlueCard*Tier 2Why HorizonOut-of-State Coveragen/an/aat Tier 2Yesat Tier 2YesIndividual Deductible 0 1,000 1,000 1,500 1,750 2,000Family Deductible 0 2,000 2,000 3,000 3,500 4,000Individual Drug Deductiblen/an/an/an/an/an/aFamily Drug Deductiblen/an/an/an/an/an/aIndividual Maximum Out-of-Pocket 2,000 3,200 5,800 7,500 4,500 6,600Family Maximum Out-of-Pocket 4,000 6,400 11,600 15,000 9,000 13,200HEALTH CARESERVICESPCP Office Visits & Consultations 10 copay 15 copay 20 copay 30 copayDeductibleDed then 20% coinSpecialist Visits & Consultations 15 copay 35 copay 40 copay 50 copayDeductibleDed then 20% coinDIAGNOSTIC TESTINGAND IMAGINGLab/Radiology FreestandingNo chargeNo chargeNo chargeNo chargeDeductibleDeductibleLab Office VisitNo chargeNo chargeNo chargeNo chargeDeductibleDeductibleRadiology Office Visit 10 PCP copay or 15 specialist copay 15 PCP copay or 35 specialist copay 20 PCP copay or 40 specialist copay 30 PCP copay or 50 specialist copayDeductibleDed then 20% coinLab/Radiology OutpatientNo chargeDed then 30% coinDed then 25% coinDed then 40% coinDeductibleDed then 20% coinGeneric Drugs 5 copay (retail) 10 copay (mail order) 5 copay (retail) 10 copay (mail order) 10 copay (retail) 20 copay (mail order) 10 copay (retail) 20 copay (mail order)Ded then 10 copay (retail)Ded then 20 copay (mail order)Ded then 10 copay (retail)Ded then 20 copay (mail order)Preferred Brand Drugs 15 copay (retail) 30 copay (mail order) 15 copay (retail) 30 copay (mail order) 40 copay (retail) 80 copay (mail order) 40 copay (retail) 80 copay (mail order)Ded then 40 copay (retail)Ded then 80 copay (mail order)Ded then 40 copay (retail)Ded then 80 copay (mail order)Non-Preferred Brand Drugs &Specialty Drugs 30 copay (retail) 60 copay (mail order) 30 copay (retail) 60 copay (mail order) 75 copay (retail) 150 copay (mail order) 75 copay (retail) 150 copay (mail order)Ded then 75 copay (retail)Ded then 150 copay (mail order)Ded then 75 copay (retail)Ded then 150 copay (mail order)Dental PlansER Hospital 100 copay 100 copay 100 copay & ded then 25% coin 100 copay & ded then 25% coinDed then 80% coinDed then 80% coinVoluntary DentalER ProfessionalNo chargeNo chargeDed then 25% coinDed then 25% coinDed then 80% coinDed then 80% coinMedical TransportationNo chargeNo chargeDed then no chargeDed then 40% coinDeductibleDed then 20% coinUrgent Care Center 30 copay 70 copay 75 copay 75 copayDeductibleDed then 20% coinOutpatient Hospital & Physician 15 copayDed then 30% coinDed then 25% coinDed then 40% coinDeductibleDed then 20% coinInpatient Hospital 300 per day copayDed then 30% coinDed then 25% coinDed then 40% coinDeductibleDed then 20% coinPHARMACY SERVICESEMERGENCY/URGENT MEDICALSERVICESHOSPITAL SERVICESPhysician/SurgeonNo chargeDed then 30% coinDed then 25% coinDed then 40% coinDeductibleDed then 20% coinOCCUPATIONAL/PHYSICAL THERAPYOffice 10 copay 15 copay 20 copay 30 copayDeductibleDed then 20% coinOutpatient 15 copayDed then 30% coinDed then 25% coinDed then 40% coinDeductibleDed then 20% coinMATERNITY SERVICESDelivery & All Inpatient Services 300 per day copayDed then 30% coinDed then 25% coinDed then 40% coinDeductibleDed then 20% coinOTHER SERVICESIn-Home Health Care 10 copayn/a 20 copay 30 copayDeductibleDed then 20% coinRehabilitation, Hospice &Skilled Nursing Care** – Inpatient 300 per day copayDed then 30% coinDed then 25% coinDed then 40% coinDeductibleDed then 20% coinDurable Medical Equipment50% coinn/a50% coin50% coinDed then 50% coinDed then 50% coinChiropractic Care – 30 Visits PerYear Maximum 10 copay 15 copay 20 copay 30 copayDeductibleDed then 20% coinAbbreviations: “ded” refers to deductible, “coin” refers to coinsurance, “copay” refers to copayment.*Away From Home Care Program not available for HSA eligible or BlueCard plans. Out of state benefits available through BlueCard.**For 2021 all Hospice & Skilled Nursing providers are Tier 1 except BlueCard providers. All BlueCard providers are Tier 2.September 30, 2020Medical Plans // OMNIA Health PlansThis document is for informational purposes only and does not constitute a binding agreement. Please note that rates are subject to change. Contact Horizon Blue CrossBlue Shield of New Jersey for the most current rates. The information provided by this document is not intended to replace or modify the terms, conditions, limitations andexclusions contained within health, dental or vision benefit plans issued or administered by Horizon BCBSNJ. In the event of a conflict between the information contained inthis document and your plan documents, your plan documents shall control.2021 OVERVIEW SMALL GROUP INSURANCE COVERAGEOMNIA Health PlansHealth Plan BenefitsMedical Plans»OMNIA Health PlansAdvantage EPO Health PlansAdvantage Direct Access Health PlansHorizon MyWay Horizon EXPANDVisionHealth Plus PlanLife & DisabilityInternational MedicalPet InsuranceMedicare AdvantageHorizon Blue App
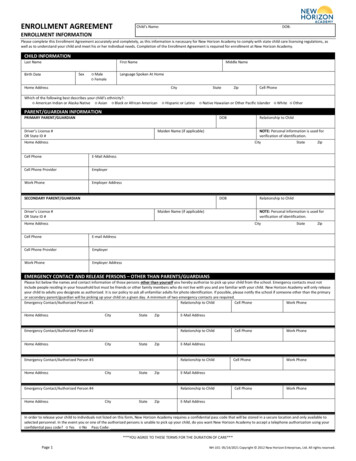
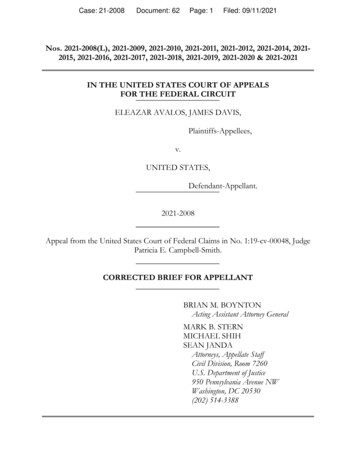
OMNIAHEALTH PLANS2021 Small Group OMNIA Health Plans2021 BENEFITSGENERALPROVISIONSOMNIA GoldTier 1Tier 2Tier 1OMNIA Silver BlueCard*Tier 2Tier 1MenuOMNIA SilverTier 2Why HorizonOut-of-State Coveragen/an/aat Tier 2Yesn/an/aIndividual Deductible 500 2,500 1,750 2,250 1,300 2,500Family Deductible 1,000 5,00 3,500 4,500 2,600 5,000Individual Drug Deductible 250 250 350 350 250 250Family Drug Deductible 500 500 700 700 500 500Individual Maximum Out-of-Pocket 5,400 7,600 8,550 8,550 8,550 8,550Family Maximum Out-of-Pocket 10,800 15,200 17,100 17,100 17,100 17,100HEALTH CARESERVICESPCP Office Visits & Consultations 10 copayDed then 30 copay 30 copay 40 copay 30 copayDed then 50% coinSpecialist Visits & Consultations 25 copayDed then 50 copay 40 copay 60 copay 60 copayDed then 50% coinDIAGNOSTIC TESTINGAND IMAGINGLab/Radiology FreestandingNo chargeNo chargeNo chargeNo chargeNo chargeNo chargeLab Office VisitNo chargeNo chargeNo chargeNo chargeNo chargeNo chargeRadiology Office Visit 10 PCP copay or 25 specialist copayDed then 30 PCP copay orDed then 50 specialist copay 30 PCP copay or 40 specialist copay 40 PCP copay or 60 specialist copay 30 PCP copay or 60 specialist copayDed then 50% coinAdvantage EPO Health PlansLab/Radiology OutpatientDed then 30 copayDed then 30% coinDed then 35% coinDed then 45% coinDed then 100 copayDed then 50% coinAdvantage Direct Access Health PlansGeneric DrugsDed then 10 copay (retail)Ded then 20 copay (mail order)Ded then 10 copay (retail)Ded then 20 copay (mail order)Ded then 25 copay (retail)Ded then 50 copay (mail order)Ded then 25 copay (retail)Ded then 50 copay (mail order) 20 copay (retail) 40 copay (mail order) 20 copay (retail) 40 copay (mail order)Preferred Brand DrugsDed then 40 copay (retail)Ded then 80 copay (mail order)Ded then 40 copay (retail)Ded then 80 copay (mail order)Ded then 50% coinDed then 50% coinDed then 50% coin1Ded then 50% coin1Non-Preferred Brand Drugs &Specialty DrugsDed then 75 copay (retail)Ded then 150 copay (mail order)Ded then 75 copay (retail)Ded then 150 copay (mail order)Ded then 50% coinDed then 50% coinDed then 50% coin1Ded then 50% coin1ER Hospital 100 copay & ded 100 copay & ded 100 copay & ded then 35% coin 100 copay & ded then 35% coin 100 copay & ded 100 copay & dedER ProfessionalDeductibleDeductibleDed then 35% coinDed then 35% coinDeductibleDeductibleMedical TransportationDed then no chargen/aDed then no chargeDed then 45% coinDed then no chargen/aUrgent Care Center 50 copayDed then 75 copay 75 copay 75 copay 75 copayDed then 50% coinOutpatient Hospital & PhysicianDed then 20 copayDed then 30% coinDed then 35% coinDed then 45% coinDed then 50 copayDed then 50% coinInpatient HospitalDed then 500 per day copayDed then 30% coinDed then 35% coinDed then 45% coinDed then 500 per day copayDed then 50% coinPhysician/SurgeonDeductibleDed then 30% coinDed then 35% coinDed then 45% coinDeductibleDed then 50% coinOffice 10 copayDed then 30 copay 30 copay 30 copay 30 copayDed then 50 copayOutpatientDed then 20 copayDed then 30% coinDed then 35% coinDed then 45% coinDed then 50 copayDed then 50% coinInternational MedicalMATERNITY SERVICESDelivery & All Inpatient ServicesDed then 500 per day copayDed then 30% coinDed then 35% coinDed then 45% coinDed then 500 per day copayDed then 50% coinPet InsuranceOTHER SERVICESIn-Home Health Care 10 copayn/a 30 copay 40 copay 30 copayn/aRehabilitation, Hospice &Skilled Nursing Care** – InpatientDed then 500 per day copayDed then 30% coinDed then 35% coinDed then 45% coinDed then 500 per day copayDed then 50% coinDurable Medical EquipmentDed then 50% coinn/aDed then 50% coinDed then 50% coinDed then 50% coinn/aChiropractic Care – 30 Visits PerYear Maximum 10 copayDed then 30% coin 30 copay 30 copay 30 copayDed then 50% coinPHARMACY SERVICESEMERGENCY/URGENT MEDICALSERVICESHOSPITAL SERVICESOCCUPATIONAL/PHYSICAL THERAPYAbbreviations: “ded” refers to deductible, “coin” refers to coinsurance, “copay” refers to copayment.*Away From Home Care Program not available for HSA eligible or BlueCard plans. Out of state benefits available through BlueCard.**For 2021 all Hospice & Skilled Nursing providers are Tier 1 except BlueCard providers. All BlueCard providers are Tier 2.1. 250 max per script for a 1-30 day supplySeptember 30, 2020Medical Plans // OMNIA Health PlansThis document is for informational purposes only and does not constitute a binding agreement. Please note that rates are subject to change. Contact Horizon Blue Cross BlueShield of New Jersey for the most current rates. The information provided by this document is not intended to replace or modify the terms, conditions, limitations and exclusionscontained within health, dental or vision benefit plans issued or administered by Horizon BCBSNJ. In the event of a conflict between the information contained in this documentand your plan documents, your plan documents shall control.2021 OVERVIEW SMALL GROUP INSURANCE COVERAGEOMNIA Health PlansHealth Plan BenefitsMedical Plans»OMNIA Health PlansHorizon MyWay Horizon EXPANDDental PlansVoluntary DentalVisionHealth Plus PlanLife & DisabilityMedicare AdvantageHorizon Blue App
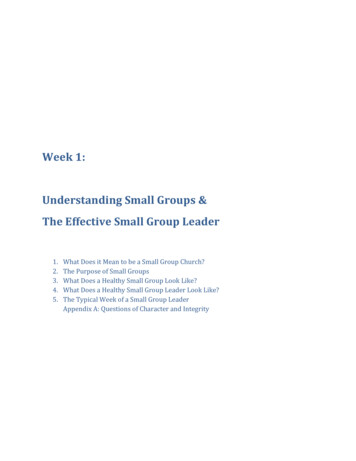
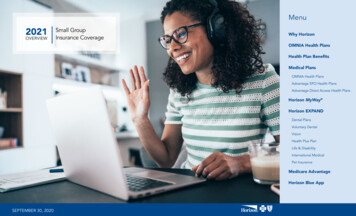
OMNIAHEALTH PLANS2021 Small Group OMNIA Health PlansOMNIA Silver HSA*2021 BENEFITSOMNIA Silver ValueMenuOMNIA BronzeTier 1Tier 2Tier 1Tier 2Tier 1Tier 2Out-of-State Coveragen/an/an/an/an/an/aIndividual Deductible 1,850 2,500 2,000 2,500 3,000 3,000Family Deductible 3,700 5,000 4,000 5,000 6,000 6,000Individual Drug Deductiblen/an/an/an/an/an/aFamily Drug Deductiblen/an/an/an/an/an/aIndividual Maximum Out-of-Pocket 6,900 6,900 7,900 8,150 8,550 8,550Family Maximum Out-of-Pocket 13,800 13,800 15,800 16,300 17,100 17,100HEALTH CARESERVICESPCP Office Visits & ConsultationsDed then 10 copayDed then 25 copay 35 copayDed then 50% coinDed then 50 copayDed then 50% coinSpecialist Visits & ConsultationsDed then 20 copayDed then 50 copayDed then 40% coinDed then 50% coinDed then 75 copayDed then 50% coinDIAGNOSTIC TESTINGAND IMAGINGLab/Radiology FreestandingDeductibleDeductibleNo chargeNo chargeNo chargeNo chargeLab Office VisitDeductibleDeductibleNo chargeNo chargeNo chargeNo chargeRadiology Office VisitDed then 10 PCP copay orDed then 20 specialist copayDed then 25 PCP copay orDed then 50 specialist copay 35 PCP copay or ded then 40%specialist coinDed then 50% coinDed then 50 PCP copay orDed then 75 specialist copayDed then 50% coinAdvantage EPO Health PlansLab/Radiology OutpatientDed then 25 copayDed then 50% coinDed then 40% coinDed then 50% coinDed then 50% coinDed then 50% coinAdvantage Direct Access Health PlansDed then 40% coinDed then 10 copay (retail)Ded then 20 copay (mail order)Ded then 10 copay (retail)Ded then 20 copay (mail order) 25 copay (retail) 50 copay (mail order) 25 copay (retail) 50 copay (mail order)Ded then 40 copay (retail)Ded then 80 copay (mail order)Ded then 50% coinDed then 50% coinGENERALPROVISIONSPHARMACY SERVICESGeneric DrugsDed then 40% coinWhy HorizonOMNIA Health PlansHealth Plan BenefitsMedical Plans»OMNIA Health PlansHorizon MyWay Preferred Brand DrugsDed then 40% coinDed then 40% coinDed then 40 copay (retail)Ded then 80 copay (mail order)Non-Preferred Brand Drugs &Specialty DrugsDed then 40% coinDed then 40% coinDed then 75 copay (retail)Ded then 150 copay (mail order)Ded then 75 copay (retail)Ded then 150 copay (mail order)Ded then 50% coinDed then 50% coinER HospitalDed then 100 copay & 20% coinDed then 100 copay & 20% coin 100 copay & ded then 40% coin 100 copay & ded then 40% coin 100 copay & ded then 50% coin 100 copay & ded then 50% coinER ProfessionalDed then 20% coinDed then 20% coinDed then 40% coinDed then 40% coinDed then 50% coinDed then 50% coinMedical TransportationDed then 20% coinn/aDed then no chargen/aDed then no chargen/aVoluntary DentalUrgent Care CenterDed then 40 copayDed then 75 copayDed then 40% coinDed then 50% coinDed then 75 copayDed then 50% coinVisionOutpatient Hospital & PhysicianDed then 20% coinDed then 50% coinDed then 40% coinDed then 50% coinDed then 50% coinDed then 50% coinHealth Plus PlanInpatient HospitalDed then 20% coinDed then 50% coinDed then 40% coinDed then 50% coinDed then 500 per day copayDed then 50% coinPhysician/SurgeonDed then 20% coinDed then 50% coinDed then 40% coinDed then 50% coinDed then no chargeDed then 50% coinOCCUPATIONAL/PHYSICAL THERAPYOfficeDed then 10 copayDed then 25 copay 35 copayDed then 50% coinDed then 40 copayDed then 50% coinOutpatientDed then 20% coinDed then 50% coinDed then 40% coinDed then 50% coinDed then 50% coinDed then 50% coinMATERNITY SERVICESDelivery & All Inpatient ServicesDed then 20% coinDed then 50% coinDed then 40% coinDed then 50% coinDed then 500 per day copayDed then 50% coinOTHER SERVICESIn-Home Health CareDed then 10 copayn/a 35 copayn/aDed then 50 copayn/aRehabilitation, Hospice &Skilled Nursing Care** – InpatientDed then 20% coinDed then 50% coinDed then 40% coinDed then 50% coinDed then 500 per day copayDed then 50% coinDurable Medical EquipmentDed then 50% coinn/aDed then 50% coinn/aDed then 50% coinn/aChiropractic Care – 30 Visits PerYear MaximumDed then 10 copayDed then 25 copay 30 copayDed then 50% coinDed then 30 copayDed then 50% coinEMERGENCY/URGENT MEDICALSERVICESHOSPITAL SERVICESAbbreviations: “ded” refers to deductible, “coin” refers to coinsurance, “copay” refers to copayment.*Away From Home Care Program not available for HSA eligible or BlueCard plans. Out of state benefits available through BlueCard.**For 2021 all Hospice & Skilled Nursing providers are Tier 1 except BlueCard providers. All BlueCard providers are Tier 2.1. 250 max per script for a 1-30 day supplySeptember 30, 2020Medical Plans // OMNIA Health PlansThis document is for informational purposes only and does not constitute a binding agreement. Please note that rates are subject to change. Contact Horizon Blue Cross BlueShield of New Jersey for the most current rates. The information provided by this document is not intended to replace or modify the terms, conditions, limitations and exclusionscontained within health, dental or vision benefit plans issued or administered by Horizon BCBSNJ. In the event of a conflict between the information contained in this documentand your plan documents, your plan documents shall control.2021 OVERVIEW SMALL GROUP INSURANCE COVERAGEHorizon EXPANDDental PlansLife & DisabilityInternational MedicalPet InsuranceMedicare AdvantageHorizon Blue App
2021 Small Group Advantage EPO Health PlansGold100% C25/452021 BENEFITSGENERALPROVISIONSHEALTH CARESERVICESDIAGNOSTIC TESTINGAND IMAGINGPHARMACY SERVICESMenuGold100% t-of-State al*Optional*Individual Deductible 0 0 1,250 2,450 2,200 3,000Family Deductible 0 0 2,500 4,900 4,400 6,000Individual Drug Deductiblen/an/an/an/an/an/aFamily Drug Deductiblen/an/an/an/an/an/aIndividual Maximum Out-of-Pocket 5,500 5,000 6,650 8,150 8,350 8,550Family Maximum Out-of-Pocket 11,000 10,000 13,300 16,300 16,700 17,100PCP Office Visits & Consultations 25 copay 40 copay 20 copay 45 copay 30 copayDed then 50% coinSpecialist Visits & Consultations 45 copay 60 copay 40 copay 70 copay 60 copayDed then 50% coinLab/Radiology FreestandingNo chargeNo chargeNo chargeNo chargeNo chargeNo chargeLab Office VisitNo chargeNo chargeNo chargeNo chargeNo chargeNo chargeRadiology Office Visit 25 PCP copay or 45 specialist copay 40 PCP copay or 60 specialist copay 20 PCP copay or 40 specialist copay 45 PCP copay or 70 specialist copay 30 PCP copay or 60 specialist copayDed then 50% coinLab/Radiology Outpatient 100 copay 100 copay 50 copayDed then 100 copay 100 copayDed then 100 copayGeneric Drugs 25 copay (retail) 50 copay (mail order) 15 copay (retail) 30 copay (mail order) 10 copay (retail) 20 copay (mail order) 25 copay (retail) 50 copay (mail order) 20 copay (retail) 40 copay (mail order) 25 copay (retail) 50 copay (mail order)Preferred Brand Drugs 50 copay (retail) 100 copay (mail order)40% coin 25 copay (retail) 50 copay (mail order) 50 copay (retail) 100 copay (mail order) 50 copay (retail) 100 copay (mail order)Ded then 50% coin***Non-Preferred Brand Drugs &Specialty Drugs 75 copay (retail) 150 copay (mail order)50% coin 50 copay (retail) 100 copay (mail order) 75 copay (retail) 150 copay (mail order) 75 copay (retail) 150 copay (mail order)Ded then 50% coin*** 100 copay & ded then 30%coin 100 copay & ded then 50%coin 100 copay & ded then 50%coinWhy HorizonOMNIA Health PlansHealth Plan BenefitsMedical PlansOMNIA Health Plans»Advantage EPO Health PlansAdvantage Direct Access Health PlansHorizon MyWay Horizon EXPANDER Hospital 100 copay 100 copay 100 copay & ded then 20%coinER ProfessionalNo chargeNo chargeDed then 20% coinDed then 30% coinDed then 50% coinDed then 50% coinMedical TransportationNo chargeNo chargeDed then 20% coinDed then 30% coinDed then 50% coinDed then no chargeUrgent Care Center 75 copay 75 copay 75 copay 75 copay 75 copayDed then 50% coinOutpatient Hospital & Physician 45 copay 50 copayDed then 20% coinDed then 30% coinDed then 50% coinDed then 50% coinInpatient Hospital 500 per day copay 500 per day copayDed then 20% coinDed then 30% coinDed then 50% coinDed then 100 per day copayHealth Plus PlanPhysician/SurgeonNo chargeNo chargeDed then 20% coinDed then 30% coinDed then 50% coinDed then no chargeLife & DisabilityOffice 25 copay 40 copay 20 copay 40 copay 30 copayDed then 50% coinInternational MedicalOutpatient 45 copay 50 copayDed then 20% coinDed then 30% coinDed then 50% coinDed then 50% coinMATERNITY SERVICESDelivery & All Inpatient Services 500 per day copay 500 per day copayDed then 20% coinDed then 30% coinDed then 50% coinDed then 100 per day copayOTHER SERVICESIn-Home Health Care 25 copay 40 copay 20 copay 40 copay 30 copayDed then 50% coinRehabilitation, Hospice &Skilled Nursing Care** – Inpatient 500 per day copay 500 per day copayDed then 20% coinDed then 30% coinDed then 50% coinDed then 100 per day copayDurable medical Equipment50% coin50% coin50% coin50% coin50% coinDed then 50% coinChiropractic Care – 30 Visits Per YearMaximum 25 copay 30 copay 20 copay 30 copay 30 copayDed then 50% coinEMERGENCY/URGENT MEDICALSERVICESHOSPITAL SERVICESOCCUPATIONAL/PHYSICAL THERAPYAbbreviations: “ded” refers to deductible, “coin” refers to coinsurance, “copay” refers to copayment.*Away From Home Care Program not available for HSA eligible or BlueCard plans. Out of state benefits available through BlueCard.**For 2021 all Hospice & Skilled Nursing providers are Tier 1 except BlueCard providers. All BlueCard providers are Tier 2.***Advantage EPO Bronze Preferred and Non-Preferred Brand drugs subject to a 250 maximum per script.September 30, 2020This document is for informational purposes only and does not constitute a binding agreement. Please note that rates are subject to change. Contact Horizon Blue Cross BlueShield of New Jersey for the most current rates. The information provided by this document is not intended to replace or modify the terms, conditions, limitations and exclusionscontained within health, dental or vision benefit plans issued or administered by Horizon BCBSNJ. In the event of a conflict between the information contained in this documentand your plan documents, your plan documents shall control.Medical Plans // Advantage EPO Health Plans2021 OVERVIEW SMALL GROUP INSURANCE COVERAGEDental PlansVoluntary DentalVisionPet InsuranceMedicare AdvantageHorizon Blue App
2021 Small Group Advantage Direct Access Health PlansPlatinum 100/702021 BENEFITSGENERALPROVISIONSHEALTH CARESERVICESDIAGNOSTIC TESTINGAND IMAGINGPHARMACY SERVICESIn-networkOut-of-networkOut-of-State CoverageMenuGold 100/80/60In-networkYes*Out-of-networkSilver HSA 100/70/60In-networkOut-of-networkYes*Why HorizonYes*Individual Deductible 0 1,500 2,000 4,000 1,675 3,000Family Deductible 0 3,000 4,000 8,000 3,350 6,000Individual Drug Deductiblen/an/an/an/an/an/aFamily Drug Deductiblen/an/an/an/an/an/aIndividual Maximum Out-of-Pocket 3,000 6,000 5,000 8,000 6,850 8,000Family Maximum Out-of-Pocket 6,000 12,000 10,000 16,000 13,700 16,000PCP Office Visits & Consultations 20 copayDed then 30% coin 30 copayDed then 40% coinDed then 30 copayDed then 40% coinSpecialist Visits & Consultations 40 copayDed then 30% coin 50 copayDed then 40% coinDed then 50 copayDed then 40% coinLab/Radiology FreestandingNo chargeDed then 30% coinNo chargeDed then 40% coinNo chargeDed then 40% coinOMNIA Health PlansLab Office VisitNo chargeDed then 30% coinNo chargeDed then 40% coinNo chargeDed then 40% coinAdvantage EPO Health PlansDed then 40% coinDed then 30 PCP copay orDed then 50 specialist copayDed then 40% coinDed then 40% coinDed then 30% coinDed then 40% coinRadiology Office VisitNo chargeDed then 30% coin 30 PCP copay or 50 specialist copayLab/Radiology OutpatientNo chargeDed then 30% coinDed then 20% coinGeneric Drugs 10 copay (retail) 20 copay (mail order) 15 copay (retail) 30 copay (mail order)Ded then 40% coinPreferred Brand Drugs 25 copay (retail) 50 copay (mail order) 40 copay (retail) 80 copay (mail order)Ded then 40% coinNon-Preferred Brand Drugs &Specialty Drugs 50 copay (retail) 100 copay (mail order) 75 copay (retail) 150 copay (mail order)Ded then 40% coinOMNIA Health PlansHealth Plan BenefitsMedical Plans»Advantage Direct Access Health PlansHorizon MyWay Horizon EXPANDER Hospital 100 copay 100 copay 100 copay & dedthen 20% coin 100 copay & dedthen 20% coinDed then 100 copay &30% coinDed then 100 copay &30% coinER ProfessionalNo chargeNo chargeDed then 20% coinDed then 20% coinDed then 30% coinDed then 30% coinMedical TransportationNo chargeDed then 30% coinDed then 20% coinDed then 40% coinDed then 30% coinDed then 40% coinUrgent Care Center 75 copayDed then 30% coin 75 copayDed then 40% coinDed then 75 copayDed then 40% coinVisionOutpatient Hospital & Physician 40 copayDed then 30% coinDed then 20% coinDed then 40% coinDed then 30% coinDed then 40% coinHealth Plus PlanInpatient Hospital 250 per day copayDed then 30% coinDed then 20% coinDed then 40% coinDed then 30% coinDed then 40% coinLife & DisabilityPhysician/SurgeonNo chargeDed then 30% coinDed then 20% coinDed then 40% coinDed then 30% coinDed then 40% coinOffice 20
Advantage EPO Health Plans Advantage Direct Access Health Plans Horizon MyWay Horizon EXPAND Dental Plans Voluntary Dental Vision Health Plus Plan Life & Disability International Medical Pet Insurance Medicare Advantage Horizon Blue App SEPtEMbEr 30, 2020 WHy HOrIzON 2021 OVErVIEW SMALL GrOUP INSUrANCE COVErAGE Now more than ever, you need .