Transcription
The Workshop will begin promptly at 12:00pmDue to the number of participants, you will be automatically placed on mute as you join to ensuregood quality sound. If you would like to comment or ask a question,please use the “chat feature”Send your questions to the host via the chat window in the Zoom meeting.Q A will open at the end of the presentation.Follow-up questions?ContactElaine Henryehenry@healthmanagement.com
FACILITATED BY:Jean Glossa, MD, MBA, FACPTELEHEALTH IN APOST-PANDEMICERA: SUSTAINABLEAPPROACHES TOSUPPORTINTEGRATED CARECopyright 2021 Health Management Associates, Inc. All rights reserved. The content of this presentation is PROPRIETARY and CONFIDENTIAL to Health Management Associates, Inc.and only for the information of the intended recipient. Do not use, publish or redistribute without written permission from Health Management Associates, Inc.Wednesday,August 10, 202112:00 – 1:30pm ESTThe Integrated Care Technical Assistance Program(ICTA) is managed by the DC Department of HealthCare Finance (DHCF) in partnership with the DCDepartment of Behavioral Health (DBH). Thisproject is supported by the Centers for Medicareand Medicaid Services (CMS) of theU.S. Department of Health and Human Services(HHS) as part of a financial assistance awardtotaling 4,616,075.00 with 100 percent fundedby CMS/HHS. The contents are those of theauthor(s) and do not necessarily represent theofficial views of, or an endorsement by, CMS/HHS,or the U.S. Government.
WHAT IS THE ICTA PROGRAM? The Integrated Care TechnicalAssistance Program (ICTA) is a five-yearprogram aimed to enhance Medicaidproviders’ capacity and corecompetencies to deliver whole personcare for physical, behavioral health, SUDand social needs of beneficiaries.The goal is to improve care andMedicaid beneficiary outcomes withinthree practice transformation corecompetencies: The ICTA Program is managed by theDC Department of Health Care Finance(DHCF) in partnership with the DCDepartment of Behavioral Health(DBH). Health Management Associateswill provide the training and technicalassistance.Copyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL3
ICTA TECHNICAL ASSISTANCE The program offers severalcomponents of coaching and training.Material is presented in variousformats. The content is created anddelivered by HMA subject matterexperts with provider idualizedcoachingOffice hoursTA Curriculum All material is available on the projectwebsite: Integratedcaredc.com Educational credit is offered at no costto attendees for select elements.Copyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and health TA4
SPEAKERSJean Glossa, MD, MBA, FACPICTA Project Director, TA Coach, SMEHealth Management AssociatesErin Holve, PhD, MPH, MPPDirector, Health Care Reform and Innovation AdministrationDepartment of Health Care FinanceEduarda KochHealth IT Project ManagerDepartment of Health Care FinanceGerald “Jerry” WilsonDirector, Division of Program IntegrityDepartment of Health Care FinanceCarrie OjoDirector of Population HealthSo Others Might Eat (SOME)Neal Sikka, MDProfessor, GWU Emergency MedicineDirector, Innovative Practice and Telehealth SectionChief, Innovative Practice & Telemedicine Section, Department of Emergency MedicineMelissa Long, MDPediatrician, Children’s Health Center at Children’s National HospitalAssistant professor, GWU School of Medicine & Health SciencesDirector, DC Mental Health Access in Pediatrics (DC MAP)Zarfishan Zahid, MDDirector of Clinical OperationsMedical Home Development GroupCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL5
DISCLOSURESFacultyNature of Commercial InterestJean Glossa, MD, MBA, FACPDr. Glossa discloses she is an employee of Health Management Associates, a national research andconsulting firm providing technical assistance to a diverse group of healthcare clientsErin Holve, PhD, MPH, MPPDr. Holve discloses that she has a financial relationship or commercial interest with RegenstriefInstitute and is an employee of Department of Health Care Finance.Eduarda KochMs. Koch discloses she is an employee of Department of Healthcare Finance.Gerald “Jerry” WilsonMr. Wilson discloses that he is an employee of Fox Rehabilitation and the Department of Health CareFinance.Carrie OjoMs. Ojo discloses she is an employee of So Others Might Eat (SOME).Zarfishan Zahid, MDDr. Zahid discloses she is an employee of Medical Home Development GroupNeal Sikka, MDDr. Sikka discloses that he has a financial relationship or commercial interest with MTEC, SonoStik,EMI, and Qualcomm Wireless Reach and is an employee of George Washington University.Melissa Long, MDDr. Long discloses that she has a family member who previously was on the board for Masimo and isan employee of Children’s National Hospital.Elizabeth Wolff, MD, MPACME ReviewerDr. Wolff discloses that she is an employee of Health Management Associates, a national researchand consulting firm providing technical assistance to a diverse group of healthcare clients.Copyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL6
AGENDATelehealth inA PostPandemicEra:SustainableApproaches toSupportIntegratedCare Welcome and Program Announcements DC Landscape to Support Telehealth Telehealth Models Used Right Now Opportunities for Telehealth expansions andbarriers/suggestions for expansion Improving access to integrated care throughtechnology Introducing eConsult/peer-to-peer consultation Q&A and Next StepsCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL7
OBJECTIVES1.2.3.4.Describe Medicaid coverageupdates, expectations fordocumentation post-public healthemergency, and potentialopportunities to expand support fordigital health among Medicaidproviders.Describe 4 different telehealthmodels currently in place acrossDistrict Medicaid providers, anddiscuss workflow and sustainabilityconsiderations for each.Identify current uses oftelehealth/eConsult and anybarriers for expansion.Review the Telehealth Assessmenttool and discuss goals for Part II ofthe workshop.Image permitted by DC Department of Health Care FinanceCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL8
DC LANDSCAPE TO SUPPORTTELEHEALTH9
Ongoing Support for Telehealth in theDistrict’s Medicaid ProgramAugust 10, 2021Department of Health Care Finance8/10/202110
Medicaid Telehealth Policy Firmly Supports Telehealth as aModality of Care Services may be rendered via telemedicine if Already included in the Department ofHealthcare Finance (DHCF) fee schedulewithin broad categories specified in theDHCF telemedicine rule Can be delivered as the standard of care Home as an originating site is allowable Providers have flexibility to work remotely Authorized during the public healthemergency – with intent to continue postPHE: Audio-only services Consent may be documented in clinicalnotes Flexibilities on using services non-HIPAAcompliant technology (per HHS)https://dhcf.dc.gov/page/telemedicine
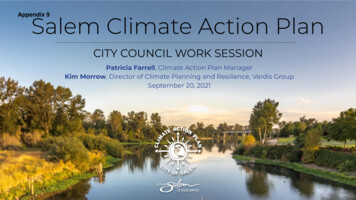
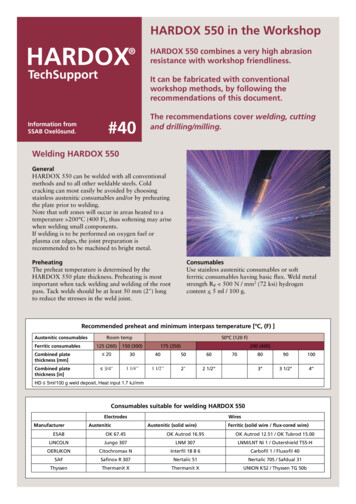
Telehealth Utilization Has Leveled Off Yet Continues To Be aWidely-used Modality of CareMonthly Telehealth Claim & Beneficiary Count (January 2020 – February 2021) In January and February 2020, telehealth accounted for just 0.3% of outpatient claims and only0.8% of beneficiaries had a telehealth service Between October 1, 2020 and February 28, 2021, approximately 21% of all outpatient claims werefor telehealth services, and 22% of Medicaid beneficiaries used at least one telehealth service.
Health IT Telehealth Digital Health13
Telehealth Documentation Must IncludeInformation on Service Modality and Contacts Effective January 1, 2021, for the purposes of servicesdelivered via telemedicine, for providers to “maintaincomplete and accurate beneficiary records of servicesprovided, ” providers must document for each clinicalencounter: The modality of service used to deliver the service (e.g.audio/visual, audio-only, etc.); The patient’s telephone number, cellphone number, orother information on how communications wereestablished with the patient based on the mode ofcommunication used to deliver the service viatelemedicine; Any other requirements applicable to the specific healthservice, per District law orregulation.*Providers can record this documentation in the providers’ clinicalnotes or other fields in the electronic health record (EHR).
ARPA Provides a One Time Opportunity to Enhance Home &Community Based Services (HCBS) The American Rescue Plan (ARPA) of 2021 was signed into law on March 11, 2021 ARPA Section 9817 Enhances Medicaid Funding for Medicaid Home and Community BasedServices 10% Federal Medical Assistance Percentages (FMAP) bump for services provided betweenApril 1, 2021, and March 31, 2022; New funds must supplement not supplant level of state funds for programs in effect as ofApril 1, 2021 Eligibility for enhanced match requires states to enhance, expand, and strengthen homeand community-based services under the state’s Medicaid program Funds are not administered like traditional grant funds; states must maintaincurrent service / benefit levels and new initiatives must be sustainable District submitted an initial and ongoing spending plan detailing proposedenhancement activities. The plan is now pending review and approval by CMS.Refer to pages 13-14 for proposed EHR incentive program and telehealth support 15 https://dhcf.dc.gov/page/arpa-hcbs-planning
Extension of the EHR Incentive Program (ARPA HCBS):Proposed Program Tracks/Milestones per practiceProgram StageTrack 1: Implement a new EHRMilestone 1.1: Participation AgreementMilestone 1.2: Complete TA Training and EducationMilestone 1.3: EHR Go-LiveMilestone 1.4: Connect to the DC HIE to view clinical informationMilestone 1.5: Send patient encounter information to the DC HIEMilestone 1.6: Send clinical notes to the DC HIETrack 2: Upgrade existing EHR to a CEHRTMilestone 2.1: Participation AgreementMilestone 2.2: Complete TA Training and EducationMilestone 2.3: EHR upgradeMilestone 2.4: Connect to the DC HIE to view clinical informationMilestone 2.5: Send patient encounter information to the DC HIEMilestone 2.6: Send clinical notes to the DC HIETrack 3: Optimize Existing EHR or Case Management SystemMilestone 3.1: Participation AgreementMilestone 3.2: Complete TA Training and EducationMilestone 3.3: Purchase gap tools or direct integration tools to connect to DC HIEMilestone 3.4: Connect to the DC HIE to view clinical informationMilestone 3.5: Send patient encounter information to the DC HIEMilestone 3.6: Send clinical notes to the DC HIEThree Tracks Based onProvider Need: Track 1: Purchase new ONCCertified EHR that meets DC’sinteroperability requirements Track 2: Upgrade to ONCCertified EHR that meets DC’sinteroperability requirements E.g. Credible - 2015 CertifiedCredible Track 3: Optimize electronicreporting and DC HIE connectivity16
ONC Certified Electronic Health Record Technology (CEHRT) EnsuresDistrict Providers are “Interoperability-Ready”Office of the National Coordinator for Health Information Technology (ONC) Certified HER SoftwareMulti-specialty EHRsFunctionalitiesHIPAA CompliantBasic Clinical InformationDemographicsFamily Health HistorySocial, Psychological, and BehavioralDeterminants DataE-PrescribingTransitions of CareDC HIE Connectivity EnabledComputerized Provider Order Entry (CPOE)MedicationsLaboratoryDiagnostic ImagingDrug-Drug CheckDrug-FormularyDrug-Drug, Drug-Allergy InteractionClinical Decision SupportTransmission to Public Health AgenciesImmunization RegistriesSyndromic SurveillanceCancer Registries (2015 CEHRT)Electronic Case Reporting (2015 CEHRT)Provider to Patient InteractionsPatient-Specific EducationAccess to Patient PortalSecure Messaging (2015 CEHRT)Provider to Provider InteractionDirect Messaging (2015 CEHRT)Athena sentPresentPresentPresentPresentPresentBehavioral Health EHRsBehavioral Health and Human Services EHR Care Management SystemPresentMyEvolv igentCarelogic own
TELEHEALTH MODELS USED RIGHTNOW18
PROVIDER SHOWCASE AND PANEL DISCUSSION:SPECIFIC MODELS SHOWCASED Improving access to care with the implementation of patient kiosks CarrieOjo, So Others Might Eat (SOME) Helping patients use technology to access their health care Dr. Neal Sikka,Department of Emergency Medicine, George Washington University Supporting primary care providers through peer-to-peer tele-mental healthconsultations Dr. Melissa Long, DC MAP (Mental Health Access in Pediatrics) Using technology to address the treatment of complex conditions includingSubstance Use Disorder Dr. Zarfishan Zahid, Medical Home DevelopmentGroupCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL19
IMPROVING ACCESS TO CARE WITHTHE IMPLEMENTATION OF PATIENT KIOSKSCarrie OjoDirector of Population HealthSo Others Might Eat (SOME)Copyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL20
SO OTHERS MIGHT EATTELEHEALTHKIOSKSLet's get you seen!Hours:Issues: thealth@some.org
TELEHEALTHMale65 years oldAfrican AmericanUnhousedLimited Income6th Grade EducationLow Digital Literacy LevelM ultiple ComorbiditiesW H O WESERVE"Mr. Some"
1TELEHEALTH GUIDEChose W ho You W ant To See2STARTASESSIONType Your Name3Turn On Camera & M icrophoneYou'reIn!3 Simple StepsIssues: thealth@some.orgYour Name
TELEHEALTHPROVIDERSMEDICAL TEAMHours:Issues: thealth@some.org
TELEHEALTHPROVIDERSMENTAL HEALTH TEAM
HELPING PATIENTS USE TECHNOLOGY TOACCESS THEIR HEALTH CARENeal Sikka, MDProfessor, GWU Emergency MedicineDirector, Innovative Practice and Telehealth SectionChief, Innovative Practice & Telemedicine Section, Department of Emergency MedicineCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL26
Neal Sikka, MDProfessorDepartment of Emergency MedicineGeorge Washington University
What is HealthDesk? A mobile desk with a mission to maximize the benefits ofdigital health technologies and platforms to improveindividual health and well-being in Wards 5,7 and 8 ofWashington, D.C What does HealthDesk do? Provides curated health information and resources Utilizes volunteer digital health coaches (DHCs) tointroduce residents to digital health applications &phone optimization settings based on their needs Helps make device/technological navigation easierand straightforward for residents with low digitalhealth literacy
Outputs Trained 8 community members Nearly 300 residentswho trained 22 more Median Age 61 Developed a Community basedPhoneAppsPop-up modelMost InterestedInDiabetesHTNHealthy LifestyleStressStroke11%36%34%11%6%In Case of EmergencyPatient nt AppsFont SizeMedication DiscountsColor Blind FeaturesStroke
Builds cultural competency and humility by working with and servingWashington, D.C. residentsImpact Increases understanding of barriers to health, especially in the digitalhealth space Helps identify ways in which digital health applications can be utilizedin their future practice
Digital HealthCoachHealthDesk helps coaches supportresidents to improve digital healthliteracy (DHL) Downloading patient portal Optimizing phone- Alarms orMedical ID Providing curated Apps (i.e HeadSpace, BabyScripts )
Digital Health Applications Patient PortalsDigitalHealthApplications& Topics Medical ID (In Case of Emergency) Phone Apps: (Headspace, BabyScripts etc)Phone Optimization Settings Font Size Color blind settings Medication alarms Voice-enabled
HealthDesk & COVID19 Provide content that will make residents morecomfortable with video telehealth appointments Work to enhance remote patient monitoring forCOVID-19 patients Utilize DHCs to assist residents with digitalhealth technology set-up/ use Set up monthly Q&A webinars with communitypartners Create videos on specific digital healthtools/technologies
Interviews with Doctors-COVID-19 Mythbusters-COVID-19 Telehealth-COVID-19 Emergency Care
Identifying Challenges to Adoption New to Smartphone How people utilized device (what are theirmain activities?) What are their concern about utilizingtheir device to help manage their health?
Developing Strategies for Engagement Awareness Access to devices/service (FCCLifeline, Medicaid, other) Promotion
Tiered ApproachInnate FeaturesSet up PhoneAdvanced FeaturesMaking Calls, Email, SMS Adding contactsUsing the cameraSettingAlarms/RemindersConnecting to WIFIBrowser SearchChange the font sizeLock ScreenIn Case of EmergencyEnable Hot SpotApps and DevicesVideo ChatInstalling AppsPatient PortalSelf TrackingConnecting Devices (BT)
Implementation Healthcare Team member education Prioritize digital health literacy At the bedside and in the community
Questions? Neal Sikka nsikka@mfa.gwu.edu HealthDesk https://smhs.gwu.edu/healthdesk/
USING TECHNOLOGY TO ADDRESS THE TREATMENTOF COMPLEX CONDITIONS INCLUDING SUBSTANCEUSE DISORDERZarfishan Zahid, MDDirector of Clinical OperationsMedical Home Development GroupCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL40
Using Technology to Address the Treatment ofComplex Conditions Including Substance Use DisorderZarfishan Zahid, M D
N C Q A recognized P C M Hthat provides primary careservices with a specialty inaddiction medicine
SERVIC ESExtendedOffice HoursPrimary CareMon - Fri: 7:00AM to 9:00PMSat-Sun: 8:00AM-6:00PMPeer Recovery SupportIntegrated CareMAT Services
I M P A C T of COVID19
TH A N K YO UZarfishan Zahid, MDzzahid@mhdgroups.net
SUPPORTING PRIMARY CARE PROVIDERSTHROUGH PEER-TO-PEER TELE-MENTAL HEALTHCONSULTATIONSMelissa Long, MDPediatrician, Children’s Health Center at Children’s National HospitalAssistant Professor, GWU School of Medicine & Health SciencesDirector, DC Mental Health Access in Pediatrics (DC MAP)Copyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL48
DC Mental Health Access inPediatricsMelissa Long, MDPediatrician, Children’s Health Center, Children’s National HospitalDirector, DC MAPAssistant Professor, GW School of Medicine & Health SciencesAugust 10, 2021
MentalHealthAccessProgramsMental Health Access Programs (MAPs orMHAPs -HRSA grantees)AKA Child Psychiatry Access Programs(CPAPs)Goal: to enhance the ability of primarycare providers to promote and managethe behavioral health needs of theirpatientsStarted in Massachusetts in 2004– Massachusetts Child PsychiatryAccess Program (MCPAP)Spread to 40 states and counting
Mental Health Access Programs:The Rationale Child mental health problems are common Most families present in the pediatricprimary care provider’s office 65% of pediatricians endorse inadequatetraining in treatment of child mental healthproblems Child psychiatrists (and other mental healthprofessionals) are in short supply
District of Columbia Mental HealthAccess in Pediatrics (DC MAP)
DC MAP: Core Services Telephone consultations– Child psychiatrist, psychologist, social worker Care Coordination Face-to-face consultation (when indicated) Training and education for pediatric primarycare providers DC Child & Adolescent Mental HealthResource Guide
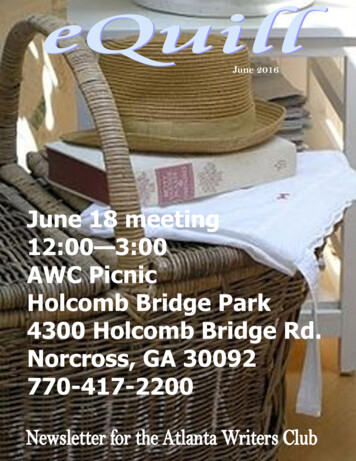
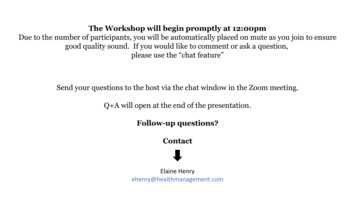
DC MAP Consults by Fiscal Year (2015 - 2021)1200Total consultsCare coordinationPsychiatryPsychology/social work1000Number of consults80060040020002015201620172018Government Fiscal Year (Oct-Sept)201920202021(Q1, Q2, Q3)
DC MAP Outcomes Provider satisfaction– 95% would recommend DC MAP to colleague Increased access to MH care– 75% endorsed increased comfort with MHtreatment– 88% say DC MAP improves patient access to MHcare Decreased utilization of emergency services– In consultations with psychiatrists where safetywas a concern, 42% of patients were able to bemanaged in primary care
Challenges/Discussion How can we help tomove pediatric PCPsfrom screening/referringfor MH concerns toscreening/diagnosing/managing MH concerns? Sustainable fundingQuestions? Melissa Long mflong@cnmc.org dcmap.org
PARTICIPANT TELEHEALTHASSESSMENT RESULTS57
TELEHEALTH ASSESSMENT AT A GLANCE 46 respondents Predominantly BH/SUD, FHQCs and non-FQHC community health centers.Practice TypeBehavioral health/SUD practiceFQHCCommunity health center (other than FQHC, RHC)Primary careGovernment/BH AuthoritySchool based health centerResidential treatmentMulti-specialty practice including primary careSpecialty practicePublic health clinicMental Health ClubhousePrivate practiceHome HealthHospital AssociationCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and 4%4%4%2%2%2%58
EXPERIENCE PROVIDING/RECEIVING TELEHEALTH Majority have experience with virtual visits and texting/direct messaging to patients Patient portal and eConsult referrals are also common, but not used by the majorityNVirtual video visits (live, interactive)Texting or direct messaging to patientsPatient PortaleConsult referral platform for specialty consultationsProject ECHO or other specialty telehealthconsultation serviceRemote patient monitoring such as scales, continuousglucose monitoring or BP monitoringStore and forward to specialists such asteledermatologyCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and 3%74%11%7%83%0%9%91%NNo%24%30%61%76%59
BENEFITS/SUCCESSES OF TELEHEALTH PROGRAM Single biggest benefit: improved BH access All other options were viewed as benefits of their telehealth program by at least two-thirds ofassessment participants, except for improved access to primary careImproved access to behavioral healthReduced no show rate for appointmentsImproved patient follow upImproved appointment scheduling processImproved provider satisfactionImproved patient satisfactionImproved access to primary careImproved access to different providers across sitesBiggest it(but not Not a benefitN%49%11101399181324%22%28%20%20%39%28%46 respondentsCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL60
BARRIERS TO TELEHEALTHIMPLEMENTATION/EXPANSION Single biggest barrier: patient access to needed capabilities Digital literacy/comfort level of patients was a reported barrier of their telehealth program by atleast two-thirds of assessment participants Less than half of assessment participants thought that lack of payment/coverage policies orscheduling were barriersBiggest barrierN%Patient access to needed capabilities (smartphone,internet access, etc)Digital literacy/telehealth comfort level of patientsDocumentation barriersDigital literacy/telehealth comfort level of providersLack of payment or coverage policiesConcerns about privacyCost of equipment and softwareScheduling barriersCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and r(but not Not a barrierN%382121262120277%17%46%46%57%46%43%59%61
EVALUATION POLLING QUESTIONAs a result ofthisworkshop, Iunderstand(check all thatapply):a. Medicaid coverage updates in theDistrict b. Expectations for documentationpost – PHE and opportunities toexpand support for digital healthamong Medicaid providersc. The 4 different telehealth modelscurrently in place across DistrictMedicaid providersd. Current uses of telehealth/eConsultand any barriers for expansionCopyright 2021 Health Management Associates, Inc. All rights reserved. PROPRIETARY and CONFIDENTIAL62
WRAP UP AND NEXT STEPS Please complete the online evaluation! If you would like to receive CMEcredit, the evaluation will need to be completed. You will receive a link tothe evaluation shortly after this workshop. The workshop recording will be available within a few days at:https://www.integratedcaredc.com/learning/ Upcoming Webinar/TA Office Hour: Stay tuned for Part II of this workshop in September! For more information about the DC Integrated Care Technical AssistanceProgram, please visit: https://www.integratedcaredc.com/63
Certified EHR that meets DC's interoperability requirements E.g. Credible - 2015 Certified Credible Track 3: Optimize electronic reporting and DC HIE connectivity 16 Program Stage Track 1: Implement a new EHR Milestone 1.1: Participation Agreement Milestone 1.2: Complete TA Training and Education Milestone 1.3: EHR Go-Live