Transcription
Benha Journal of Applied Sciences (BJAS)Vol. (7) Issue (5) (2022), (15-20)print: ISSN 2356–9751online: ISSN 2356–976xhttp://bjas.journals.ekb.egRole of chest ultrasound to differentiate between acute cardiogenic pulmonary edemaand non-cardiogenic pulmonary edema (acute respiratory distress syndrome)M.M.Refaat1, M.A.Elassal2, T.S.Essawy3 and A.B.Hasaneen4Radiology Dept., Faculty of Medicine, Benha Univ., Benha, Egypt2Internal Medicine, Dept., Faculty of Medicine, Benha Univ., Benha, Egypt3Chest Diseases Dept., Faculty of Medicine, Benha Univ., Benha, Egypt4Critical care medicine Dept., Faculty of Medicine, Benha Univ., Benha, EgyptE-mail: Asmaa.bahy8819@gmail.com1AbstractIntroduction Chest Ultrasound can help in rapid treatment of acute respiratory failure in intensive care units whenrapid decisions are needed and especially when patients’ transport is a big difficult. Therefore, CUS can be consideredan attractive complementary diagnostic tool and one of the most promising techniques for differentiation andmanagement of critically ill patient with either acute cardiogenic pulmonary edema (APE) or acute respiratory distresssyndrome (ARDS). Aim :This study was aim to clarify the role of chest ultrasonography to differentiate betweenARDS(Acute respiratory distress syndrome) and Acute cardiogenic pulmonary edema in patients admitted to ICU withacute dyspnea. Patients and methods Lung US was applied to respiratory distressed patients In Benha UniversityHospital ICUs on 60 patients who divided into APE group (23 cases) or ARDS group (37 cases). LUS examinationfocused on detecting the following pleuropulmonary signs in both groups: alveolar–interstitial syndrome(AIS), absentor reduced lung sliding,spared areas ,subpleural consolidation pleural line abnormalities, and pleural effusion. ResultAlveolointerstitial syndrome (AIS )was observed in 100% of APE patients and in100% ofARDS patients . Absent orreduced lung sliding was observed in 0% of APE patients and in 97.3% of ARDS patients(P 0.001). spared areaswere found in 0% of APE patients and100% in ARDS patients( 0.001),lungConsolidations were present in 4.3% ofAPE patients in 94.6% of ARDS patients with (P 0.001). Pleural line abnormalities were observed in 13% of APEpatients and in 100% of ARDS patients(P 0.001),and Pleural effusion was present in 100% Of APE patients and in40.5% of ARDS patients with APE (P 0.001). All these signs, except the AIS sign,presented a statistically significantdifference in differentiation between ARDS and APE, resulting in specific ultrasonographic pleuropulmonary signs ofARDS and APE. Conclusion Results of the current study demonastrated that LUS play asignificant role in managementof respiratory failure patients especially cases of ARDS and APE in ICU by helping in rapid diagnosis anddifferentiation between both types in accompanying with EChocardiodraohy and IVC diameter measurement. Absenceof reduced lung sliding,spared areas,suppleural consolidation, pleural line abnormalities, on a background of AISconsidered specific features for differentiation between ARDS and APE.Keywords: acute cardiogenic pulmonary edema, acute respiratory distress syndrome, lung ultrasonography, chestultrasound.1. IntroductionAcute respiratory failure is one of the mostdistressing situations for the patient. Emergency casesdo not always present in conditions that are ideal forimmediate diagnosis, which sometimes compromisesoutcome [1].ARDS may be differentiated from cardiogenicpulmonary oedema using lung ultrasound( LUS)on thebasis of inhomogeneous interstitial pattern, pleural linechanges and presence of lung consolidation [2], withUS interstitial syndrome diagnostic accuracy of 95%when compared to CT-defined ARDS [3].ARDS can be diagnosed once cardiogenicpulmonary oedema and alternative causes of acutehypoxemic respiratory failure and bilateral infiltrateshave been excluded. ARDS diagnosis based on TheBerlin Definition (4, 5, and 6): Respiratory symptoms must have begun withinone week of a known clinical insult, or the patientmust have new or worsening symptoms during thepast week. Bilateral opacities consistent with pulmonaryoedema must be present on chest radiograph orcomputed tomography (CT) scan.The patient’s respiratory failure must not be fullyexplained by cardiac failure or fluid overload. Anobjective assessment (e.g, echocardiography) toexclude hydrostatic pulmonary edema is required .A moderate to severe impairment of oxygenationmust be present, as defined by the ratio of arterialoxygen tension to fraction of inspired oxygen(PaO2/FiO2).Acute respiratory distress syndrome (ARDS) hastraditionally been caused by a variety of insults assepsis, which considered the most common cause ofARDS[7].On the other hand cardiogenic pulmonary oedemais defined as pulmonary edema due to increasedcapillary hydrostatic pressure as a result of cardiacdysfunction, The differentiation between ALI/ARDSand CPE is important in order to avoid delayingtreatment of fluid retentionThis study was aim to clarify the role of chestultrasonography to differentiate between ARDS(Acuterespiratory distress syndrome) and Acute cardiogenicpulmonary edema in patients admitted to ICU withacute dyspnea.
16Role of chest ultrasound to differentiate between acute cardiogenic pulmonary edema and non-cardiogenic2. Patients and methodsThis cross sectional prospective study wascarried out in the Intensive care units at BenhaUniversity Hospital to clarify the role of chestultrasonography to differentiate between ARDS andacute pulmonary edema to allow proper management inboth cardiac and non cardiac one.In the period betweenDecember 2019 till November 2021 Patients wereeligible for participation in this study if they hadreceived a new diagnosis of acute respiratory faliure.ABG testing was ordered within ICU admission,showed aPao 2 /Fio 2 ratio less than 300. patientsdividing into two groups,ARDS group who admittedand fulfilling criteria of Berlin ARDS definition .In addition, APE group who diagnosed on thebasis of clinical signs and symptoms, ECG, chestradiography, and echocardiography.As LUS is nowpart of routine diagnostic procedures inour unit, noinformed consent or approval of ethics committee wererequested.All patients underwent LUS on admissionand after being diagnosed based on clinical andradiological data.Regarding the probes used we have two probesAlinear array operates between 6 to 12MHzCurvilinear array operates between 4 to 5 MHztransducer ultrasound machine:[Sonoline GE Logiq F8ultrasound machineoptional features (staticelastrography, LOGIQ View,made in India) at thegeneral ICU of Benha University Hospital was used forlung examination.The examination was performed at patient bedside.Lateral or seated positions were used to scan theposterior thorax. In patients in whom the seatedposition was not possible, a lateral decubitus positionwas used to examine posterior lung regions .Probes were placed vertically along eachintercostal space (the parasternal line, anterior axillaryline, and posterior axillary line) on both sides. Datawere displayed on a screen. Each hemithorax should bedivided into five zones: two anterior zones separatedby the third intercostal space, two lateral zones, andone posterior zone .The following ultrasonographic signs wereinvestigated in this study to differentiate betweenARDS and APE: Alveolointerstitial syndrome (AIS) defined as thePresence of more than3 Ultrasound lung cometsmeans (B lines) or "white lung" appearance foreach examined area. pleural line sliding was defined as evidence ofpleural movement; indicates a pulmonary region incontact with the thoracic wall and excludes pneumothorax,which may beabsent or reduced in acute lung injury ,lobarconsolidation and atelectasis Pleural lines abnormalities defined as thickeninggreater than 2mm, evidence of small sub pleuralconsolidations or coarse appearance of the pleuralline its presence means a process eitherconsolidations or inflammatory process as in casesof ARDS,ALI and its absence means acute processas in (APE). Pleural effusion which appeared as anechoic areaslimited by diaphragm. Spared areas which are normal areas of the lungsurrounded by areas of AIS. Subpleural consolidation,Air bronchogram whichare appear mainly in cases of ARDS appear ascomet tail appearance.B profile is the main diagnostic profile of ourstudy which means presence of more than 3 Blines inthe scanned field in two zones bilaterally by applyingBLUE Protocol as all of our patients were critically illdyspenic patients.In this study Patients divided into NonCardiogenic group37 patients and cardiogenic group,23patientsNon cardiogenic group were selected by precededhistory of infective causes and other causes asmalignancy of ARDS.Most common affected cases of infective causeswere COVID swab ve represent 56,8%of all ARDScases.Cardiogenic-pulmonary oedema group: who werepreliminary diagnosed by Echocardiography, historyand examination.Statistical MethodsData were collected, revised, then extracted andcoded in excel file. The coded data were analyzedusing Statistical package for Social Science (SPSS)version 26.The analyzed data was presented in suitable tablesand graphs using mean Standard deviation (SD) forcontinuous variables, and frequency and percentage forcategorical variables.Independent 2 samples t-test was used to analyzecontinuous variables differences across independenttwo groups, and Chi-Square test was used to examinethe relationship between two qualitative variables.Fisher’s exact test was used to examine the relationshipbetween two qualitative variables when the Chi-squaretest assumptions were violated (the expected count isless than 5 in more than 20% of cells)To estimate the prediction ability of USparameters to pulmonary edema natural and comparebetween them, the following indicators werecalculated: Sensitivity, specificity, positive predictivevalue (PPV), negative predictive value (NPV) , andaccuracy.Additionally, the receiver operating characteristic(ROC) curve was drawn for each parameter, the areaunder the ROC curves were calculated, and thestatistical differences between the area under the ROCcurves and 0.5 were calculated and tested forsignificance.All tests of significance were conducted at 0.05level of significance.Benha Journal Of Applied Sciences, Vol. (7) Issue (5) (2022(
M.M.Refaat, M.A.Elassal, T.S.Essawy and A.B.Hasaneen173. ResultsThe study included 60 patients. 37 met the criteria of ARDS and 23 had APE. There were 36 male and 24 femalepatients. The demographic characteristics of studied patients are shown in Table 1,2Demographic analysis in both groupTable (1) comparison between the two groups as regard personal data.Sex, no., %MaleFemaleAge, mean SDNoncardiogenic (n 37)Cardiogenic (n 23)p-value211638.8615863.260.5256.843.2 16.4165.234.8 11.38 0.001*Table (2) Demographic characteristics of study population as regard clinical onYesNoPneumoniaYesNoMalignancyYesNoNoncardiogenic (n 37)No.%Cardiogenic (n 13 0.001*43310.889.219482.617.4 .01000.037 *211656.843.20230.0100 0.001*53213.586.50230.01000.15 p-valueIn the demographic and comorbid data comparison between the study groups, It was found that the diabetes,hypertension and IHD were significantly higher among cardiogenic pulmonary edema patients compared tononcardiogenic patients.On the other hand, sepsis, pneumonia, and aspiration rates were significantly higher among noncardiogenicpulmonary edema patients compared to cardiogenic patients.Table (3) Comparison between ARDS group and cardiogenic group as regard laboratory findings.P/F ratioWBCNoncardiogenic (n 37)MeanSD158.8964.60414.2437.3273Cardiogenic (n Additionally , WBC count was higher in noncardiogenic group than cardiogenic,while P/F ratio was higher incardiogenic group than cardiogenic one.Benha Journal Of Applied Sciences, Vol. (7) Issue (5) (2022(
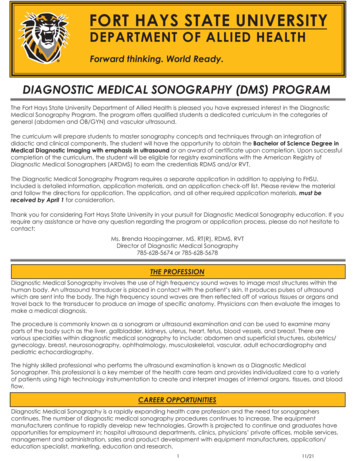
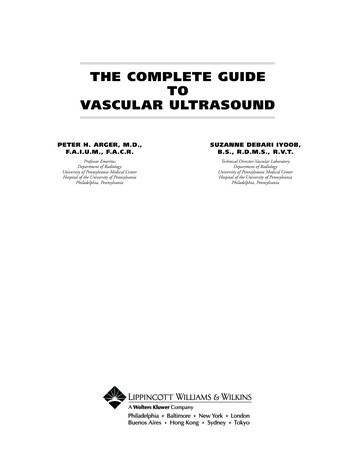
18Role of chest ultrasound to differentiate between acute cardiogenic pulmonary edema and non-cardiogenicTable (3) Comparison between acute respiratory distress syndrome and acute cardiogenic pulmonary edema cases asregards lung ultrasonographic findings.Noncardiogenic (n 37)AIS, no., %37100YesNoReduced Pleural sliding, no., %3697.3Yes12.7NoPleural line abnormalities, no., %37100Yes00.0NoSub pleural consolidation, no., %3594.6Yes25.4NoPleural effusion, no., %1540.5Yes2259.5NoSpared areas, no., %37100Yes00.0No1.430.2933IVC mean SDCardiogenic (n 23)p-value23100NA0230.0100 0.001*3201387 0.001*1224.395.7 0.001*2301000.0 0.001*0232.3700.0100.4247 0.001* 0.001*The sensitivity and specificity of each ultrasonographic sign in ARDS and APE, are illustrated in Table( 4)Table (4) Ultrasound-based predictors for noncardiogenic pulmonary edema.Reduced Pleural slidingPleural line abnormalitiesSub pleural consolidationNo pleural effusionSpared areasIVC diameter d parameters including 5 indices were significantly different between the study groups and each one ofcould be used as an independent parameter given its sensitivity and selectivityThe comparison above showed that the spared areas had the highest accuracy followed by the reduction in pleuralsliding.IVC with a cutoff point of 1.95 was a significant predictor for cardiogenic pulmonary edema. Values 1.95 wereindicative for noncardiogenic pulmonary edema with a sensitivity and specificity of 97.3 and 95.7% respectively.Fig. (1) AIs in both groups,but homogeneous in APEBenha Journal Of Applied Sciences, Vol. (7) Issue (5) (2022(
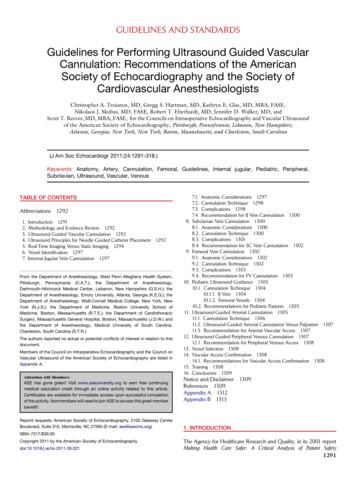
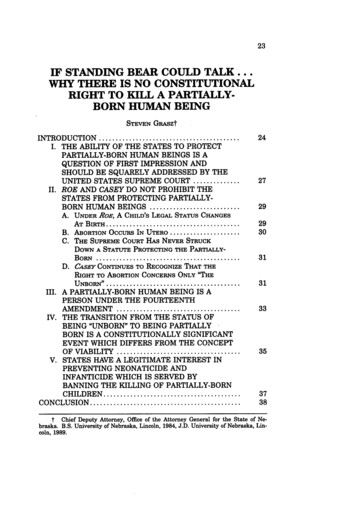
M.M.Refaat, M.A.Elassal, T.S.Essawy and A.B.Hasaneen19Fig. (2) show pleural effusion and air bronchogram, in ARDSFig. (3) spared areas in between AIS characteristic for ARDS4. DiscussionLung ultrasound is a relatively novel application ofpoint- of-care diagnostic ultrasound in acute care. It isnon- invasive, rapid and relatively easy to perform and,as such,it bridges the gap between clinicalexamination and other time consuming investigations,helping to guide patient management in a number ofclinical scenarios. It has the potential to significantlyreduce time to correct diagnosis, harmful radiation,risk of transport and cost.In the current study both groups cardiogenic andnon cardiogenic were charachterized by AIS (alveolarinterstitial syndrome)which is characterized bymultiple diffuse vertical artifacts (B-lines), andcorrelates with extravascular lung water by 100% .This was agree with the study of Taher Elnagarret al[8].on 2016 which done on28 patient .Agreementalso with Daabis et al.[9] on2014 ,study on 100 pateint10% of them was diagnosed as ARDS also show thatAIS was found in all of them.In the current study absence of pleural sliding wasfound in94.6%in non cadiogenic group,and 4.3%incardiogenic group.Agreement with the study of TaherElnagarr et al.on 2016 that found reduction or absenceof pleural sliding in all ARDS patients in his study,thisalso agree with copetti et a[10].on 2008 on 58 patients,Absence or reduction of the 'gliding sign' wasobserved in 100% of patients with ALI/ARDS and in0% of patients with APE.In the current study pleural line abnormalities weredetected in 100%of non cardiogenic group and0%ofcardiogenic group.The result was matching withELnagarr et al. study on 2016which detect pleural lineabnormalities in 100% of patients with ALI/ARDS andin 0% of patients with APE.Also copetti et al.on.[10]2008 on 58 patients Pleural line abnormalities wereobserved in 100% of patients with ALI/ARDS and in25% of patients with APE (p 0.0001). In the currentstudy Subpleural consolidation in 94.6% of noncardiogenic group&4.3% 0.001which was nearly comparable to that reported byZanobetti et al. [11], InAgreement with A.Sanjanet al.[12] on 2019 on 73 respiratory distressed patientsfound that consolidation were present in moderate(100%)and sever(92.3)% ARDS.In the current study spared areas(areas of normallung in betweenB lines found in100%of nonBenha Journal Of Applied Sciences, Vol. (7) Issue (5) (2022(
20Role of chest ultrasound to differentiate between acute cardiogenic pulmonary edema and non-cardiogeniccardiogenic group and 0%of cardiogenic group thissign had the highest accuracy followed by thereduction in pleural sliding and subpleuralconsolidation.In agreement with Copetii et al.on 2008 on 58patients 'Spared areas' were observed in 100% ofpatients with ALI/ARDS and in 0% of patients withAPE (p 0.0001).In the current study the spared areas had thehighest accuracy followed by the reduction in pleuralsliding as its sensitivity and specificity 100%Pleural effusion in the current study represents40.5%of non cardiogenic group&100%of cardiogenicgroup ,pleural effusions were more frequently seen inAPE than in ARDS .Absence of Pleural effusion hasSensitivity of59.5%& Specificity 100%Similar resultswere reported by Copettiet al.on 2008. and Kataoka etal. [13]5. ConclusionResults of the current study show that using lungUS in Differentiation between ARDS and APEthrough the Characterestic pleuropulmonary signs asspared areas of AIS, reduced lung sliding , subpleuralconsolidation and pleural effusion add ahigh value inthe clinical field regarding early diagnosis andmanagement of respiratory failure patients, especiallyin ICU,also using lung ultrasound saves time anddecreases the need for CT,whose drawbacks includedelayed Care implementation ,irradiation and highFeasibility.[3]Reference[1] P. Ray, S. Birolleau, Y. Lefort, Acute respiratoryfailure in the elderly: etiology, ,2006.[2] R. Copetti, G. Soldati, P. Copetti, Chestsonography: a useful tool to differentiate acutecardiogenic pulmonary edema from acuterespiratory distress syndrome.[3] D. Lichtenstein, N.lascols, Meziere cultation, chest radiography, and lungultrasonography in acute respiratory distresssyndrome, Anesthesiology.vol.100 (1),pp. 9–15,2004.[4] C.Guerin, F.Bayle, V.Leray. Open lung biopsy innon resolving ARDS frequently identifies diffusealveolar damage regardless of the severity stageand may have implications for 015.[5] ND.Ferguson, E.L.Fan. The Berlin definition ofARDS: an expanded rationale, justification, andsupplementary material. Intensive Care Med .vol.“38,pp.1573. 2012.[6] G.Soldati, R.Inchingolo, A.Smargiassi, S.Sher.Ex vivo lung sonography: morphologicultrasound relationship. Ultrasound Med dbio,03.001,2012.[7] R.Iscimen, R.Cartin-Ceba, M.Yilmaz. Riskfactors for the development of acute lung injuryin patients with septic shock: an observationalcohort study. Crit Care Med" 2008.[8] Taher El-Naggara , Samar H. Sharkawya ,Hossam Mohamed Abdel-Hamida , Haitham S.El-Din Mohamada , Rasha Mustafa A.Mohamedb Egypt J Bronchol 2016 10:319–323 2016 Egyptian Journal of BronchologyEgyptian Journal of Br[9] R.Daabis , L.Banawan, A.Rabea, El.Abdelaziz ,S.Ayman, review articleRelevance of chestsonography in the diagnosis of acute respiratoryfailure: Comparison with current diagnostic toolsin intensive care units, Egyptian J of Chest Disand Tubercu.vol.63,pp.979-85,2014[10] R.Copetti,G.Soldati,P.Copetti:Chestsonography: a useful tool to differentiate acutecardiogenic pulmonary edema from acuterespiratory distress syndrome. CardiovascUltrasound.vol. 6,pp. 16. 10.1186/1476-7120-616,2008.[11] Zanobetti, Maurizia . Can chest ultrasonographyreplace standard chest radiography for evaluationof acute dyspnea in the ED?” Chest.vol. 139,pp.1140-1147,2011.[12] A.Sanjan ,S.Vimal Krishnan ,Siju V.Abraham, etal utility of point of care ultrasound for initialassessment of ARDS Patients in emergencydepartment J EMERG Trauma shock . Oct-Dec.vol.12(4),pp.248-253. Article pubReader cite,2019.[13] H.Kataoka, S.Takada. The role of thoracicultrasonography for evaluation of patients withdecompensated chronic heart failure. J Am CollCardiol.vol. 35(6),pp.1638–1646,2000.Benha Journal Of Applied Sciences, Vol. (7) Issue (5) (2022(
16 Role of chest ultrasound to differentiate between acute cardiogenic pulmonary edema and non-cardiogenic