Transcription
THE COMPLETE GUIDETOVASCULAR ULTRASOUNDPETER H. ARGER, M.D.,F.A.I.U.M., F.A.C.R.SUZANNE DEBARI IYOOB,B.S., R.D.M.S., R.V.T.Professor EmeritusDepartment of RadiologyUniversity of Pennsylvania Medical CenterHospital of the University of PennsylvaniaPhiladelphia, PennsylvaniaTechnical Director-Vascular LaboratoryDepartment of RadiologyUniversity of Pennsylvania Medical CenterHospital of the University of PennsylvaniaPhiladelphia, Pennsylvania
THE COMPLETE GUIDETOVASCULAR ULTRASOUND
To Christopher, my parents Susan and Robert, my brother Chris, my grandmotherEdith, and to all the rest of my family and friends (especially Susan Schultz andBonnie Brake) for their love, guidance, and support.S.D.I.To Afento, Harry, Donald, Anastasia, Eugenia, and Nicholas, to whom I amimmensely grateful, as they have profoundly influenced my whole approach to life.P.H.A.
CONTENTSPreface ix4Grafts 45I. Hemodialysis Grafts 45II. Bypass Grafts 485Peripheral Venous Systems 55I. Lower Extremity Veins 55II. Upper Extremity Veins 696Penile Vessels 757Cerebrovascular System 848Test Validation and Statistics 1089A Word About Doppler Controls 109Acknowledgments xi1Blood Vessels: Anatomy and Physiology 12Abdominal Vasculature 6I. Abdominal Aorta 6II. Inferior Vena Cava 10III. Hepatic Veins, Portal Veins, and HepaticArteries 11IV. Superior Mesenteric Artery 17V. Renal Arteries and Renal Veins 193Peripheral Arterial Systems 26I. Lower Extremity Arteries 26II. Upper Extremity Arteries 41Appendix 121I. Review Questions 121II. Answer Key 129Subject Index 131
PREFACEVascular ultrasound has expanded to become an integral component of nearly every aspect of diagnostic ultrasound. The complexity of vascular ultrasound has increasedas the technology has increased, along with the ability ofultrasound equipment to visualize more and more vessels aswell as a wider range of flow variables. The increased capability and utilization of color, power, and duplex Dopplerare examples of this.Understanding both the technical and diagnosticaspects of vascular ultrasound is essential to obtaining themaximum information that can be acquired and to makingthe most cogent and informative diagnosis of a given problem.The Complete Guide to Vascular Ultrasound has a different approach to vascular ultrasound, that combines the“technique know-how” and “diagnostic analysis”. Thisapproach results in a better diagnosis of pathology at multiple levels. To promote a comprehensive approach to indepth knowledge of any given vascular problem, most chapters are divided into a six-part approach:1. Anatomy. Graphically demonstrates the general anatomyof the vascular area to be examined as well as the anatomyof individual vessels.2. Pathology. Briefly discusses the pathologic processes,which can affect the vessels being examined. Outlinesimportant associated pathophysiologic information necessary for good analysis.3. History/Questions to Ask the Patient. Details symptoms associated with potential vascular disease of thevessels being evaluated.4. Diagnostic Examinations. Details necessary technicalaspects of the examination tailored to the specific vesselbeing evaluated. This may include commonly performed but non-ultrasound tests.5. Diagnostic Analysis. Includes Doppler waveform imagesand illustrations. Discusses in a detailed outline form ofthe relevance of various clinical findings.6. Other Diagnostic Tests related to the clinical problemincluding nonultrasound diagnostic tests.We believe the information in this book speaks to awide audience including physicians, i.e., radiologists, vascular surgeons, and cardiologists, as well as sonographers,whose work is vital to the field of ultrasound.Peter H. ArgerSuzanne DeBari Iyoob
ACKNOWLEDGMENTSWe would like to extend our sincere thanks to Patricia Hartman whose invaluablehelp was a key factor in the production of this book. Her computer skills and typing ofthe many modifications and re-modifications were a constant source of strength.We also extend our gratitude to Philips Ultrasound, Scott Leonard, and all of thesonographers and physicians in the Ultrasound section at the Hospital of the Universityof Pennsylvania. We appreciate their help in acquiring the ultrasound images included inthis book. We would also like to thank Steven Horii for sharing his technical expertise.
1BLOOD VESSELS:ANATOMY AND PHYSIOLOGYI. ANATOMY OF BLOOD VESSELSA. Three Layers (Tunicae) of Blood Vessels (Fig. 1.1)1. Tunica interna or intima. This is the innermostlayer and is composed of endothelial cells.2. Tunica media. This is the middle layer and is composed of smooth muscle and elastic fibers. It is thickerin arteries, can change the size and shape of arteries,gives arteries their rigidity and round shape, and isinfluenced by hormones and other chemicals.3. Tunica externa or adventitia. This is the outer layerand is composed of collagenous and elastic fibers. Itprotects and anchors the vessel to surrounding tissues.B. Circulatory System (Fig. 1.2)1. Systemic circulation refers to the flow of bloodfrom the left ventricle of the heart through the body(except for the lungs) and back to the right atrium ofthe heart. The blood carries oxygen and nutrients tothe tissues of the body. It also removes wastes, carbondioxide, and heat from the tissues of the body. Theblood leaves the left ventricle of the heart, and goesthrough the aorta, arteries, arterioles, venules, veins,and vena cava to enter the right atrium of the heart:Heart Aorta Arteries Arterioles Capillaries Venules Veins Vena cava Heart2. Pulmonary circulation refers to the flow of bloodfrom the right ventricle of the heart, through the rightand left pulmonary arteries, to the alveoli (air sacs) inthe lungs, then from the alveoli of the lungs, throughthe right and left pulmonary veins, and back to the leftatrium. The blood is deoxygenated when it enters thealveoli from the right ventricle (as it has already gonethrough the rest of the body through the systemic circulation) and is oxygenated when it leaves the alveoliof the lungs to go into the left atrium.Heart Pulmonary arteries Alveoli Pulmonary veins HeartC. Types of Blood Vessels1. Arteries are blood vessels that transport bloodfrom the heart to the tissues of the body. They containall three layers of tunicae. The tunica interna andmedia is thicker than in veins. The tunica externa isthinner than in veins. These divide into smaller andsmaller branches, eventually dividing into arterioles.2. Arterioles. These small vessels are regulators ofblood flow from the arteries into the capillaries. Asthey get closer to the capillaries, the layers of arterioledecrease to consist only of an endothelial layer surrounded by a few smooth muscle fibers. Vasoconstriction (when the smooth muscle constricts) decreasesblood flow into the capillaries. Vasodilation (when thesmooth muscle relaxes) increases blood flow into thecapillaries. Arterioles have the highest resistance in thecirculatory system. They account for one half of thetotal resistance to blood flow.3. Capillaries. These microscopic vessels only have asingle layer of endothelium and a basement membrane. They allow exchange of nutrients and wasteproducts between the blood and the cells of tissue.Capillaries (sometimes extensive networks of capillaries) usually connect arterioles and venules.4. Venules. These vessels drain blood from the capillaries into the veins. Close to the capillaries, venulesmay only consist of an endothelial layer surrounded bythe tunica externa. Closer to the veins, venules consistof all three layers.5. Veins. Veins are blood vessels that transport bloodfrom the tissues of the body back to the heart. Theyare composed of all three layers of tunicae, althoughthe tunica intima and tunica media are thinner than inarteries. The tunica externa is thicker than in arteries.Veins contain valves to prevent backflow of the blood,which has lower pressure at this point.6. Vasa vasorum. This is a network of minute bloodvessels that perfuse the tissues of blood vessels themselves.
2The Complete Guide to Vascular UltrasoundFIGURE 1.1. Three layers of a vessel wall.II. PHYSIOLOGY AND CHARACTERISTICS OFBLOOD FLOWA. Blood flow is the amount of blood that passesthrough a vessel during an episode of time. Blood flowsin a laminar flow pattern in most vessels (Fig. 1.3). Alaminar flow pattern is a stable pattern consisting ofmany laminae (layers) that are concentric. Each layer isthought to flow at a different velocity. The velocity ofeach layer increases as they approach the center of thelumen. The center is where the highest velocity of bloodflow is thought to exist. The two primary factors thatdetermine blood flow are blood pressure and resistance.B. Blood pressure. The pressure that the blood exertson the vessel walls is considered the blood pressure.1. Blood pressure is directly proportional to bloodflow. When one increases, so does the other.2. Blood always flows from areas with higher pressureto areas with lower pressure.3. Blood pressure starts off high as the blood leavesthe left ventricle to go into the systemic circulation(mean pressure of 100 mm Hg) as it progresses downto 0 mm Hg when the blood returns to the heart inthe right atrium.4. Principal factors that affect arterial blood pressure:a. Cardiac output. Cardiac output is determinedby multiplying the stroke volume (which is theamount of blood ejected from either ventricle inone systole, typically 70 mL) by the heart rate. Thisis 5.25 L/min in a normal, resting adult. Cardiacoutput is directly proportional to blood pressure.When one increases, so does the other. When onedecreases, so does the other.b. Blood volume. The volume of the blood is alsodirectly proportional to the blood pressure. Whenone increases, so does the other. When onedecreases, so does the other. Normally, the volumeof blood in an adult is about 5 L. Hemorrhagedecreases blood volume and thus the blood pressurealso decreases. High salt intake (water retention)increases blood volume, and thus the blood pressurealso increases.c. Peripheral resistance is defined as all the factorsthat oppose blood flow in the circulatory system.Arterioles change their diameters to affect the resistance, which affects blood flow and blood pressure.As peripheral resistance increases, so does the arterial blood pressure. This is a directly proportionalrelationship as well.5. Resistance. Opposition to blood flow. This occursas a result of friction between the blood vessel wallsand the blood. It also occurs due to the viscosity thatis created by the plasma proteins and the red bloodcells. It is directly proportional to blood pressure andas a result blood flow. An increase in resistance wouldresult in an increase in both blood flow and bloodpressure.FIGURE 1.2. Simplified circulatory system.
1/Blood Vessels: Anatomy and Physiology3FIGURE 1.3. Laminar flow.6. Principal factors that affect resistance to bloodflow:a. Blood viscosity. The viscosity of the blood ishow “thick” the blood is. It takes more energy tomove blood that is more viscous. The viscosity isdirectly proportional to resistance and thus bloodpressure. Dehydration, severe burns, and polycythemia (an increase in the number of red bloodcells) all cause an increase in the viscosity of theblood, which increases resistance and increasesblood pressure. A condition such as anemia or hemorrhage can cause a decrease in the viscosity of theblood, which decreases the resistance and the bloodpressure.b. Blood vessel radius. The fourth power of theradius of a blood vessel is inversely proportional tothe resistance. When the radius decreases, the resistance and blood pressure increase. Smaller vesselsobviously have higher resistances.c. Blood vessel length. The longer the blood vessel, the higher the resistance. There is a direct proportional relationship.C. Poiseuille’s Law helps to determine how much fluidis moving through a vessel. It is an equation thatdescribes the relationship between resistance, pressure,and volume flow. It demonstrates that the change in thediameter of a blood vessel affects resistance the most. Asthe radius decreases, the resistance increases. The velocityof the blood flow then must increase to keep the sameamount of blood moving through the vessel. Therefore,there is an inversely proportional relationship betweenthe velocity of a blood vessel and the site of the bloodvessel.(P 1 P2) π r4Poiseuille’s Law Q ᎏᎏ8ηLQ volume flowP1 pressure at the proximal end of the vesselP2 pressure at the distal end of the vesselr radius of the vesselL length of the vesselπ 3.1416η viscosity of the fluidAn abbreviated pressure/volume flow relationship canalso be used:Q P/RQ volume flowP pressureR resistanceD. Reynolds Number. As pressure increases, volume flowincreases as well. This occurs only to a point. When the stable laminar flow becomes disturbed, the smooth streamlines break up and form small circular currents called eddycurrents and vortices. Osborne Reynolds discovered thatwhen the flow pattern changes from smooth to disturbed,flow volume was no longer increased by increased pressure.Instead, the flow disturbance increased. Reynolds numberis a “dimensionless” number that reveals at what point flowbecomes turbulent. When the number exceeds 2,000, theflow becomes turbulent. Other factors such as irregularitiesof the vessel wall and plaque, pulsatility of blood flow, andbody movement can cause blood flow to become turbulentat lower values of the Reynolds number.Vq2rReynolds Number (Re) Re ᎏηRe Reynolds numberV velocityq density of the fluid (since density and viscosityare usually constant, turbulent flow)r radius of the tube (develops mainly as a result ofchanges in velocity or radius)η viscosity of the fluidE. The Bernoulli Equation. This demonstrates thatthere is an inversely proportional relationship pressureand velocity. When there is high velocity, there is lowpressure and vice versa. Flow separations are pressure gradients (the difference in pressure from one area of thevessel to another). These can be caused by a change indirection of the vessel (curve or bend) or a change in thegeometry of the vessel (due to widening such as in thecarotid bulb or narrowing due to stenosis or plaque) (Fig.1.4). Velocity decreases in an area of a flow separation,and the pressure increases. Because blood flows fromhigh pressure to low pressure, the direction of the bloodflow changes in this area.
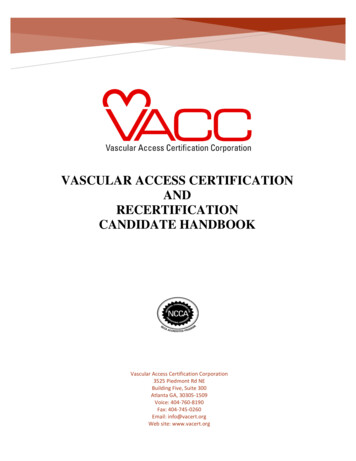
4The Complete Guide to Vascular UltrasoundFIGURE 1.4. Effects of stenotic plaque on flow pattern, velocity, and pressure.F. Other Characteristics of Blood Flow1. Flow that is low-resistance is continuous andsteady throughout systole and diastole. It is usuallyfound feeding a dilated vascular bed, such as in theinternal carotid, renal, vertebral, hepatic, splenic, andceliac arteries.2. Flow that is high resistance is pulsatile (tri- orbiphasic) (Fig. 1.5). It can usually be found in arteries that supply high-resistance peripheral vascularbeds such as the external carotid, aorta, iliac, subclavian, fasting superior mesenteric, and extremityarteries.3. Diastolic flow reversal is normally found in arteriessupplying high-resistance peripheral vascular beds.This flow reversal increases with vasoconstriction anddecreases with vasodilation (which can be produced byexercise, body heating, and stenosis). For example, anormally high-resistance arterial Doppler signalbecomes low resistance after exercise. The diastolicflow reversal portion of the waveform is now seen as aforward reflection.4. Diastolic flow reversal disappears distal to astenosis.5. Diastolic flow reversal can also disappear proximalto a significant stenosis.6. Vasoconstriction causes an increase in pulsatility insmall and medium-size arteries and a decrease in pulsatility in minute arteries, arterioles, and capillaries.FIGURE 1.5. Doppler tracing of the midaorta, demonstrating high-resistance, pulsatile flow.
1/Blood Vessels: Anatomy and Physiology7. Vasodilation causes a decrease in pulsatility in smalland medium-size arteries and an increase in pulsatilityin minute arteries, arterioles, and capillaries.8. Total blood flow may be normal in an extremity atrest even when there is a significant stenosis or occlusion of a vessel. This is due to development of a collateral network.5BIBLIOGRAPHYRumwell C, McPharlin M. Arterial evaluation in vascular technology—an illustrated review Pt. 1, 2nd ed. Pasadena, CA: DaviesPublishing, 2000:1–33.Tortora GJ, Anagnostakos NP. The cardiovascular system: vessels androutes. In: Principles of anatomy and physiology, 6th ed. New York:Harper & Row, 1990: 606–612.
2ABDOMINAL VASCULATUREI. ABDOMINAL AORTAA. Anatomy (Fig. 2.1)1. Abdominal aorta extends from the twelfth thoracicvertebra to the fourth lumbar vertebra.2. Portions of the Abdominal Aorta (Fig. 2.2):a. Proximal—superior to or at the level of the celiacaxis, measures 2 to 3 cmb. Middle—below the celiac axis, above the renalarteries, measures 1.6 to 2.5 cmc. Distal—just above the bifurcation, measures 1.1to 2.0 cmd. Iliac arteries—measure 0.6 to 1.4 cm3. Main branches off the aorta:a. Celiac axis or celiac artery: first branch off theabdominal aorta, divides into the left gastricartery, splenic artery, and common hepaticartery. These feed the stomach, spleen, liver, pancreas, and duodenum.b. The superior mesenteric artery is approximately 1 cm distal to the celiac axis. This arteryfeeds the small intestine, ascending colon, cecum,and part of the transverse colon.c. The renal arteries are the next branches. They supply the kidneys, ureters, and adrenal glands (Fig. 2.3).d. The inferior mesenteric artery is approximately3 to 4 cm above the aortic bifurcation. It supplies thedescending, iliac, and sigmoid colon, as well as the lefthalf of the transverse colon and part of the rectum.e. The common iliac arteries are the terminalbranches of the abdominal aorta. They divide into theinternal iliac arteries and the external iliac arteries.4. Other branches off the abdominal aorta but notcommonly seen on ultrasound are:a. The paired inferior diaphragmatic or inferiorphrenic arteries.b. The paired middle suprarenal arteries.c. The paired gonadal arteries.d. The paired first to fourth lumbar arteries.e. The middle sacral artery.5. Above the umbilicus, all paired arteries course posterior to their related vein. Below the umbilicus, allpaired arteries course anterior to their related vein.B. Pathology1. Ectasia—when the abdominal aorta does not taperas it normally does, but is not dilated to the point ofaneurysm.2. Atherosclerosis or arteriosclerosis—thickening,hardening, and deposition of plaque in the intimalwall of arteries, which can cause stenosis.a. This is associated with smoking, hypertension,sedentary lifestyle, diabetes mellitus, and increasedlevels of low-density lipoprotein (LDL) levels ofcholesterol.b. Because of its large size and high flow rate, theabdominal aorta is sensitive to plaque. Two common sites of plaque formation are the origin of therenal arteries and the bifurcation into the commoniliac arteries. The most common site is theinfrarenal portion of the aorta.c. More men than women are affected with atherosclerosis, and the incidence increases with age.d. Atherosclerosis may be associated withaneurysm and wall weakening.3. Coarctation is the narrowing of the aorta. Thereare two clinical findings associated with this:a. Hypertension resulting from decreased kidneyperfusion.b. Manifestation of lower extremity ischemiadecreased lower extremity pulses.4. Aneurysm—increase in arterial diameter (Fig. 2.4).a. Types of aneurysms (Fig. 2.5):(1) Fusiform—symmetric swelling, most common, usually found below the level of the renalarteries (90% of all aneurysms) and may extendinto the common iliac arteries. These also maycontain thrombus.(2) Saccular—focal outpouching, least common, usually affects the left lateral portion ofthe distal abdominal aorta (where the least support is), causes marked alteration in the patternof blood flow. These also may have thrombus orplaque.(3) Dissecting—tear in intimal lining of the wallof the vessel. A false lumen is created between the
2/Abdominal Vasculature7FIGURE 2.1. Abdominal vasculature.intima and the media. These may extend fromthe aortic valve to the abdominal aorta. They canbe very dangerous. Blood flow may push the flapacross the lumen and completely (or almost completely) obstruct flow. Two flow lumens withmarkedly different flow characteristics would beseen. These are most common in the thoracicaorta (Fig. 2.6).FIGURE 2.2. Sagittal view of the middle and distal aorta.(4) Pseudoaneurysms or false aneurysms. Smallpocket of moving blood connected to an arterythrough a small opening or neck and may bepartly surrounded by thrombus. These form dueto interventional radiology procedures (e.g., cardiac catheterization using the common femoralartery), trauma, surgery, or infection. They canbe felt as a pulsatile mass. A turbulent flow pat-FIGURE 2.3. Transverse view of the renal arteries coming off theaorta.
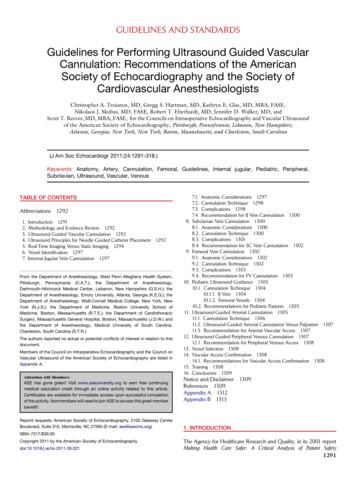
8The Complete Guide to Vascular UltrasoundFIGURE 2.4. Abdominal aortic aneurysm. Note the irregulardilatation of the distal aorta.tern would be visualized. Compression with atransducer may clot them off. An alternativetherapy would be thrombin injection.b. Abdominal aortic aneurysm is considered if thediameter is greater than 3 cm or greater than 50%than the original diameter.c. A true aneurysm contains all the layers of theartery (fusiform and saccular.) A false aneurysm orpseudoaneurysm leaks through a hole in the intimabut is contained by the external layer or by the body.d. There is an increased risk for abdominal aorticaneurysm in close relatives.e. The incidence of the disease is highest amongmen, particularly those over 65 years of age.f. The identification of an abdominal aorticaneurysm increases the risk for aneurysms in thecommon iliac arteries, common femoral arteries,and popliteal arteries.g. Only 4% of abdominal aortic aneurysms actually affect flow into the renal arteries. Stenosis of therenal arteries and hydronephrosis are potential complications of abdominal aortic aneurysms.FIGURE 2.6. Dissection of the abdominal aorta. There appear tobe parallel hypoechoic lumens within the aorta. The posteriorportion is the false lumen, separated from the true lumen by theflap (arrow). (Image courtesy of Philips Medical Systems.)h. Aneurysms over 6 cm in diameter are consideredsurgical emergencies, and 60% of all aneurysmsover 7 cm will rupture within 1 year. Abdominalaortic aneurysms can have small tears and leak intothe body cavity.i. The main complication of abdominal aorticaneurysm is rupture; the main complication ofperipheral aneurysm is distal embolization.j. Atherosclerotic abdominal aortic aneurysms maybecome inflammatory, and the wall will becomethickened and surrounded by fibrosis.k. Marfan syndrome is associated with weakness ofthe arterial wall and may result in aneurysm of thefirst portion of the aorta leading up to the aorticvalve. This may lead to dissection of this portion ofthe aorta.FIGURE 2.5. Types of aneurysms.
2/Abdominal Vasculaturel. To repair an aneurysm, the surgeon may put agraft in. The native aorta is usually wrapped aroundthe graft. Fluid can accumulate between the graft andthe vessel wall. Types of aortic grafts are as follows:(1) Aortic end-to-end graft (wrapped in nativeaorta)(2) Aortoiliac graft(3) Aorto-bifemoral graftC. History: Questions to Ask the Patient1. Do you have abdominal pain? (May be deep andpenetrating, mainly in the back). Aortic rupture causessevere pain.2. Do you have a pulsing sensation in your abdomen?(Most of the time a thoracic aneurysm will not be considered. However, if this is a consideration or if on earlyviews of the aorta one sees a suggestion of extensionfrom the thoracic area, then ask the next question).3. Do you have high back pain, a cough, wheezing,hoarseness, or difficulty swallowing?D. Diagnostic Examination1. Begin with the patient in the supine position,although a decubitus position can be helpful to evaluate the bifurcation.2. Using a 3.5- or 5-MHz curved-array transducer,place the transducer in a sagittal plane at the midlineof the body, just inferior to the xiphoid process of thesternum. Slightly move or angle the transducer to theleft and locate the proximal aorta. Slowly move inferiorly, using a rock-and-slide motion.3. Repeat in the transverse plane.4. Measure anteroposterior and transverse dimensionsof the aorta, outside wall to outside wall.FIGURE 2.7. Sagittal view of a bifurcated endograft (closedarrows) within dilated aortic lumen (open arrows). (Image courtesy of Philips Medical Systems.)95. Take sagittal and transverse images of the followingstructures with and without calipers:a. Proximal aorta (inferior to the diaphragm andsuperior to the celiac trunk).b. Mid aorta (inferior to the celiac trunk and alongthe length of the superior mesenteric artery).c. Distal aorta (inferior to the superior mesentericartery and superior to the bifurcation).d. Right and left common iliac arteries.e. Color images and Doppler waveforms may betaken if necessary.f. If evaluating an endovascular stent graft, takegray-scale images in both planes, and color imagesand Doppler waveforms through the native aorta,entire graft, and outflow iliac vessels. Assess theentire residual aneurysm sac as well. Evaluate potential sites for endoleaks, such as the attachment sitesof the graft or branches related to the lumbar arteryand inferior mesenteric artery (Fig. 2.7).6. Distinguishing the aorta from the inferior venacava (IVC) on ultrasound:a. The aorta never touches the liver; the IVC does.b. The aorta has thicker walls (thicker tunica media).c. The aorta has cardiac pulsatility; the IVCchanges with respiration.d. The aorta tapers from superior to inferior; theIVC has a “hammock” shape.e. The aorta and IVC have different Doppler signals.f. The aorta has multiple anterior branches, whilethe only branches from the IVC are the hepaticveins.g. The right renal artery is seen posterior to theIVC; no vessels course posterior to the aorta.E. Diagnostic AnalysisAnalysis of the abdominal aorta would include the following:1. The maximum true anteroposterior, length, andtransverse dimensions.2. Documentation of the location of an aneurysm,and of whether the renal arteries or iliac arteries areinvolved.3. Notation of wall thickening in terms of what typeand how extensive it is.4. Evaluation for dissection. This appears as a thinmembrane “fluttering” in the lumen. Doppler showsdifferent signals in each of the channels.5. Examination of both kidneys for signs of hydronephrosis or renal artery stenosis.6. Verification that normal triphasic or biphasicwaveforms that are high resistance are seen withDoppler.7. An endoleak associated with an endovascular stentgraft has a distinctly different Doppler signal thanfrom that of the endograft. There should be no flowleaking out around the graft, inside or outside of theresidual aneurysm sac.
10The Complete Guide to Vascular UltrasoundF. Other Diagnostic Tests1. Aortic angiography2. Magnetic resonance angiography (MRA)3. Computed tomographic angiography (CTA).II. INFERIOR VENA CAVAA. Anatomy (Fig. 2.8)1. Originates from the paired common iliac veins atfifth lumbar vertebra.2. Lies to the right of the aorta.3. The size is generally less than 3.5 cm during fullinspiration.4. The main branches include the hepatic veins,renal veins, and the common iliac veins.5. The right and left renal veins enter the IVC laterally, coursing anterior to the renal arteries. The leftrenal vein is longer, and courses anterior to the aortaand posterior to the superior mesenteric artery (SMA).6. The right gonadal and fourth lumbar vein also entersthe IVC. (The left gonadal vein enters the left renal vein.)7. The tunica media of the IVC is very thin and elastic.8. There are no valves in the IVC. There are also novalves in the external and common iliac veins, hepatic,renal, lumbar, gonadal, and soleal sinuses.9. During inspiration, the intrathoracic pressuredecreases and the intraabdominal pressure increases.Blood moves from the abdomen into the chest withdecreased outflow from the peripheral veins, and flowin the legs should decrease or stop. Inflow is allowedfrom upper extremities. During expiration, vice versa.Outflow increases from the lower extremity veins.10. Hydrostatic pressure is pressure due to gravity—when the patient is supine, hydrostatic pressure is negligible (0–15 mm Hg). When the patient is erect,hydrostatic pressure may be 102 mm Hg dependingon his or her height.B. Pathology1. Enlargement of the IVC. A faulty tricuspid valvethat allows blood to reflux through the right atriumFIGURE 2.8. Sagittal view of the inferior vena cava.into the IVC causes the size of the IVC to be large( 3.5 cm). Color flow shows reversal—blue then redthen blue again pattern.2. Thrombus in the IVC may lead to localizedswelling and noncollapse of the IVC during exhalation.3. Tumors may invade the IVC, especially from theright kidney through the right renal vein. These metastasize from lymphoma, hepatocellular carcinoma, renalcell carcinoma, and breast carcinoma. Primary tumorsare rare. Leiomyosarcoma of the IVC wall is the mostcommon type of mural tumor in the venous system.4. Budd-Chiari syndrome—thrombus in hepaticveins prevents blood from draining from the liver tothe IVC.5. Congenital abnormalities may include thehepatic veins draining directly into the right atrium.6. IVC rupture usually occurs after trauma or surgery.7. Greenfield filter (or other filter) — placed in theIVC near the confluence of the renal veins or iliacveins. This keeps the thrombus from coursing throughthe IVC, heart, and pulmonary vessels. A surgical clipcan also be placed in the IVC to decrease the risk forpulmonary embolism.C. History: Questio
Vascular ultrasound has expanded to become an inte-gral component of nearly every aspect of diagnostic ultra-sound. The complexity of vascular ultrasound has increased as the technology has increased, along with the ability of ultrasound equipment to visualize more and more vessels as wel