Transcription
Value Plan Saver Plan Choice PlanS5660 & S59832021 SUMMARY OF BENEFITSJanuary 1, 2021 – December 31, 2021PRESCRIPTION SAVINGS WITH PLANSTHAT PUT YOUR NEEDS FIRST.This booklet gives you a summary of what Express Scripts Medicare (PDP) Value, Saver andChoice plans cover and what you pay. It doesn’t list every service that we cover or every limitationor exclusion.To get a complete list of services we cover, you can view our Evidence of Coverage online atexpress-scriptsmedicare.com/2021documents, or call Customer Service for more informationor to request an Evidence of Coverage.This document is available in braille, large print and other formats for people with disabilities.Please contact Customer Service if you need plan information in another format.Express Scripts Medicare (PDP) is a prescription drug plan with a Medicare contract.Enrollment in Express Scripts Medicare depends on contract renewal.Y0046 B00SNS1A MCRP2101 004368.1B00SNS1A
CONTACT INFORMATIONHow can I contact Express Scripts Medicare?If you are not a member of this plan:Call toll-free 1.866.477.5704; TTY: 1.800.716.3231,24 hours a day, 7 days a week, except Thanksgiving and Christmas.Website: express-scriptsmedicare.comIf you are a member of this plan:Call toll-free 1.800.758.4574 (New York State residents: 1.800.758.4570);TTY: 1.800.716.3231, 24 hours a day, 7 days a week.Website: express-scripts.comABOUT EXPRESS SCRIPTS MEDICARE (PDP)Who can join our plan?To join Express Scripts Medicare (PDP), you must be entitled to Medicare Part A and/orbe enrolled in Medicare Part B and live in our service area. Our service area includes: Value plan: All 50 states, the District of Columbia and Puerto Rico.Saver plan: All 50 states, the District of Columbia and Puerto Rico.Choice plan: All 50 states and the District of Columbia.Which drugs are covered?We will generally cover the drugs in our formulary (list of covered Part D prescription drugs)as long as the drug is medically necessary, the prescription is filled at an Express Scripts Medicarenetwork pharmacy, and other plan rules are followed.You can see the complete 2021 formulary online for each of our plans, as well as any restrictions,at express-scriptsmedicare.com/2021formulary.Which pharmacies can I use?We have a network of pharmacies (both standard and preferred), and you must generally use thesepharmacies to fill your prescriptions for covered Part D drugs. If you use an out-of-network pharmacy,the plan may not pay for these drugs, and you may pay more than you pay at an in-network pharmacy.Some of our network pharmacies have preferred cost-sharing. You may pay less if you usethese pharmacies.You can check online to see if your pharmacy is in our network atexpress-scriptsmedicare.com/2021network.1
HOW ARE DRUG COSTS DETERMINED?Cost may vary, depending on: The drug’s tierOur plans group each medication into one of five or six “tiers.” The type of pharmacy you useOur plans offer standard and preferred retail network pharmacies, standard and preferred homedelivery pharmacies (including Express Scripts Pharmacy ), as well as long-term care, homeinfusion and Indian Health Service / Tribal / Urban Indian Health Program (I/T/U) pharmacies.Cost-sharing amounts at long-term care, home infusion and I/T/U pharmacies are the same as ata standard retail pharmacy. See page 1 for information about costs at out-of-network pharmacies. The number of days the prescription is written forOur plans may offer a 30-day supply, 60-day supply or 90-day supply, depending on the drug tierand pharmacy type. (Supplies at home infusion, I/T/U and out-of-network pharmacies are limitedto 30 days. Long-term care pharmacies may dispense up to a 31-day supply.) Which stage of the benefit you have reachedSee information on benefit stages below.WHAT ARE THE MEDICARE PART D BENEFIT STAGES? Annual Deductible StageIn this stage, you pay a set amount before your plan begins to pay its share of the cost, if applicable. Initial Coverage StageThis stage begins after you pay your yearly deductible, if applicable. You remain in this stage untilyour total yearly drug costs reach 4,130. (Total yearly drug costs include the total drug costs paidby you and any Part D plan since the calendar year began.) Coverage Gap (or Donut Hole) Stage (Most members do not reach the Coverage Gap.)This stage begins after your total yearly drug costs exceed 4,130. Catastrophic Coverage StageThis stage begins after your year-to-date out-of-pocket costs exceed 6,550.PART D SENIOR SAVINGS MODEL – SAVER AND CHOICE PLANSThe Part D Senior Savings Model provides consistent copays for select insulin drugs in all stagesuntil you reach the Catastrophic Coverage Stage. (If you reach that stage, the cost-sharing amountson page 8 will apply.) If you receive “Extra Help,” you do not qualify for this program, and yourLow-Income Subsidy (LIS) benefit will apply. To find out which drugs are select insulins, you canreview the plan’s Formulary, visit our website at express-scriptsmedicare.com/2021formulary,or contact Customer Service at the phone numbers on page 1.Choice plan: The copay for select insulins in Tier 6 is 0 at a preferred pharmacy or 11 at astandard pharmacy for a 30-day supply in all stages up to the Catastrophic Coverage Stage.Saver plan: The copay for select insulins in Tier 3 is 35 for a 30-day supply at all network pharmacytypes, in all stages up to the Catastrophic Coverage Stage. Because there is no deductible for insulinsin Tier 3, the copay will not apply toward the deductible.2
MONTHLY PREMIUM AND DEDUCTIBLE A premium is the amount you pay for your prescription drug coverage each month.An annual deductible is the amount you pay out-of-pocket each year before theInitial Coverage Stage begins. Not all tiers have a deductible, as noted below.If you receive “Extra Help,” this information may not apply to you.Monthly PremiumYou must continueto pay yourMedicare Part Bpremium.Value PlanSaver PlanChoice Plan 16.80 – 61.00per monthSee the Premium Tableon pages 8 – 9 for thepremium in your state. 18.50 – 32.40per monthSee the Premium Tableon pages 8 – 9 for thepremium in your state. 61.00 – 87.60per monthSee the Premium Tableon pages 8 – 9 for thepremium in your state.Annual DeductibleValue PlanSaver PlanChoice PlanTier 1PreferredGeneric Drugs 0 per year 0 per year 0 per yearTier 2Generic Drugs 0 per year 0 per year 0 per year 445 per-yeartotal for all tierswith a deductible 0 per yearfor select insulins*; 285 per-yeartotal for all tierswith a deductiblefor remaining drugs 0 per yearTier 4Non-PreferredDrugs 445 per-yeartotal for all tierswith a deductible 285 per-yeartotal for all tierswith a deductible 100 per-yeartotal for all tierswith a deductibleTier 5SpecialtyTier Drugs 445 per-yeartotal for all tierswith a deductible 285 per-yeartotal for all tierswith a deductible 100 per-yeartotal for all tierswith a deductibleTier 6Select CareTier Drugs 0 per yearNot applicable –Saver plan does nothave a Tier 6 0 per year,including select insulins*Tier 3PreferredBrand Drugs* Part D Senior Savings Model: See page 2 for more information.3
INITIAL COVERAGE STAGE – VALUE PLAN COST-SHARINGThe tables that follow represent an overview of costs for the Value plan. Some costs vary bystate. To find the cost in your state, please see the tables beginning on page 10.If you receive “Extra Help,” this information may not apply to you.Initial CoverageStagePreferred RetailPharmacyStandard RetailPharmacyDrug Tier30-daysupply60-daysupply90-daysupplyTier 1Preferred Generic Drugs 1copay 2copay 3copay30-daysupply60-daysupplyCopay varies by state. Please referto the table on pages 10 – 11.Tier 2Generic DrugsCopay varies by state.Please refer to the table on pages 12 – 13.Tier 3Preferred Brand DrugsCopay varies by state.Please refer to the table on pages 14 – 15.Tier 4Non-Preferred DrugsCoinsurance varies by state.Please refer to the table on pages 16 – 17.Tier 5Specialty Tier Drugs25% of the cost(30-day supply only)Tier 6Select Care Tier DrugsInitial CoverageStage 0copay 0copay 0copay90-daysupplyCopay varies by state. Please referto the table on pages 18 – 19.PreferredMail OrderStandardMail OrderUp to a 90-day supplyUp to a 90-day supplyTier 1Preferred Generic Drugs 0copayCopay varies by state. Please referto the table on pages 10 – 11.Tier 2Generic Drugs 0copayCopay varies by state. Please referto the table on pages 12 – 13.Tier 3Preferred Brand DrugsCopay varies by state.Please refer to the table on pages 14 – 15.Tier 4Non-Preferred DrugsCoinsurance varies by state.Please refer to the table on pages 16 – 17.Tier 5Specialty Tier Drugs25% of the cost(30-day supply only)Drug TierTier 6Select Care Tier Drugs 0copayCopay varies by state. Please referto the table on pages 18 – 19.4
INITIAL COVERAGE STAGE – SAVER PLAN COST-SHARINGThe tables that follow represent an overview of costs for the Saver plan.If you receive “Extra Help,” this information may not apply to you.Initial CoverageStagePreferred RetailPharmacyStandard RetailPharmacyDrug ly60-daysupply90-daysupplyTier 1Preferred Generic Drugs 2copay 4copay 6copay 19copay 38copay 57copayTier 2Generic Drugs 7copay 14copay 21copay 20copay 40copay 60copayTier 3Preferred Brand Drugs 35copay 70copay 105copay 47*copay 94*copay 141*copayTier 4Non-Preferred Drugs50% of the costTier 5Specialty Tier Drugs28% of the cost(30-day supply only)Initial CoverageStagePreferredMail OrderStandardMail OrderUp to a 90-day supplyUp to a 90-day supplyTier 1Preferred Generic Drugs 0copay 57copayTier 2Generic Drugs 0copay 60copayTier 3Preferred Brand Drugs 105copay 141*copayDrug TierTier 4Non-Preferred Drugs50% of the costTier 5Specialty Tier Drugs28% of the cost(30-day supply only)* Part D Senior Savings Model: Select insulins on Tier 3 will have the same copay as at preferrednetwork pharmacies. See page 2 for more information.5
INITIAL COVERAGE STAGE – CHOICE PLAN COST-SHARINGThe tables that follow represent an overview of costs for the Choice plan. Some costs varyby state. To find the cost in your state, please see the tables beginning on page 20.If you receive “Extra Help,” this information may not apply to you.Initial CoverageStagePreferred RetailPharmacyStandard RetailPharmacyDrug ly60-daysupply90-daysupplyTier 1Preferred Generic Drugs 2copay 4copay 6copay 10copay 20copay 30copayTier 2Generic Drugs 7copay 14copay 21copay 20copay 40copay 60copayTier 3Preferred Brand Drugs 42copay 84copay 126copay 47copay 94copay 141copayTier 4Non-Preferred DrugsCoinsurance varies by state.Please refer to the table on page 20.Tier 5Specialty Tier Drugs31% of the cost(30-day supply only)Tier 6 *Select Care Tier DrugsInitial CoverageStage 0copay 0copay 0copay 11copay 22copay 33copayPreferredMail OrderStandardMail OrderUp to a 90-day supplyUp to a 90-day supplyTier 1Preferred Generic Drugs 0copay 30copayTier 2Generic Drugs 4copay 60copayTier 3Preferred Brand Drugs 126copay 141copayDrug TierTier 4Non-Preferred DrugsCoinsurance varies by state.Please refer to the table on page 20.Tier 5Specialty Tier Drugs31% of the cost(30-day supply only)Tier 6 *Select Care Tier Drugs 0copay 33copay* Part D Senior Savings Model: Tier 6 includes select insulins. See page 2 for more information.6
COST-SHARING IN THE COVERAGE GAP (OR DONUT HOLE) STAGE*This stage begins after your total yearly drug costs exceed 4,130.If you receive “Extra Help,” this information does not apply to you.ValueTier 1Preferred Generic DrugsTier 2Generic DrugsTier 3Preferred Brand DrugsTier 4Non-Preferred DrugsTier 5Specialty Tier Drugs(30-day supply only)Tiers 1 - 6 25% of the cost forgeneric drugs 25% of the cost forbrand drugs (plusa portion of thedispensing fee)SaverTiers 1 - 5 25% of the cost forgeneric drugs 25% of the cost forbrand drugs (plusa portion of thedispensing fee)Select insulinsin Tier 3*The lesser of: 25% of the costof the drug, or 35 for a30-day supplyTier 6Select Care Tier Drugs(Value and Choiceplans only)ChoiceTier 1 2 for a 30-day supplyat a preferred retailpharmacy 10 for a 30-day supplyat a standard retailpharmacyTier 2 7 for a 30-day supplyat a preferred retailpharmacy 20 for a 30-day supplyat a standard retailpharmacyTiers 3, 4, 5 and 6 25% of the cost forgeneric drugs 25% of the cost forbrand drugs (plusa portion of thedispensing fee)Select insulinsin Tier 6* 0 for a 30-day supplyat a preferred retailpharmacy 11 for a 30-day supplyat a standard retailpharmacy* Part D Senior Savings Model: See page 2 for more information.7
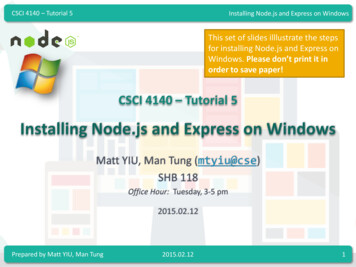
COST-SHARING IN THE CATASTROPHIC COVERAGE STAGEThis stage begins after your year-to-date out-of-pocket costs exceed 6,550.If you receive “Extra Help,” this information may not apply to you.ValueTiers 1 - 6Tier 1Preferred Generic DrugsSaverTiers 1 - 5ChoiceTiers 1 - 6You pay the greater of 3.70 or 5% of the cost for generic drugs, and thegreater of 9.20 or 5% of the cost for all other drugs.Tier 2Generic DrugsTier 3Preferred Brand DrugsTier 4Non-Preferred DrugsTier 5Specialty Tier Drugs(30-day supply only)Tier 6Select Care Tier Drugs(Value and Choiceplans only)PREMIUM loradoConnecticutDelawareDistrict of waKansasYou must continue to pay your Medicare Part B premium.Value Plan 25.70 28.10 33.60 40.20 61.00 30.30 32.80 30.50 30.50 26.80 49.90 46.40 34.70 22.80 26.40 49.70 28.90Saver Plan 25.30 32.40 22.50 26.40 26.50 31.50 27.40 28.50 28.50 27.20 20.20 21.10 24.30 30.60 22.60 25.20 25.008Choice Plan 68.80 70.40 77.00 76.20 84.90 84.50 76.40 65.70 65.70 84.30 61.00 62.30 76.70 86.70 78.90 81.00 72.30
PREMIUM TABLE, raskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaPuerto RicoRhode IslandSouth CarolinaSouth est VirginiaWisconsinWyomingYou must continue to pay your Medicare Part B premium.Value Plan 26.40 33.60 25.30 30.50 32.80 30.90 49.70 49.90 26.30 49.70 49.70 22.20 25.30 32.30 50.60 33.20 45.40 49.70 53.00 26.20 30.30 36.70 30.40 32.80 54.70 49.70 25.70 16.80 34.70 32.80 53.00 30.30 36.70 31.60 49.70Saver Plan 22.60 28.60 25.80 28.50 27.40 18.50 25.20 27.80 21.70 25.20 25.20 24.70 25.80 27.70 30.40 23.60 26.50 25.20 22.70 26.80 29.50 25.90 23.20 27.40 28.90 25.20 25.30 27.50 24.30 27.40 27.10 29.50 25.90 27.50 25.209Choice Plan 78.90 63.40 65.40 65.70 76.40 71.20 81.00 67.70 73.30 81.00 81.00 72.00 65.40 76.80 65.30 87.60 70.70 81.00 65.90 75.60 71.60 82.40N/A 76.40 69.80 81.00 68.80 82.10 76.70 76.40 62.30 71.60 82.40 80.80 81.00
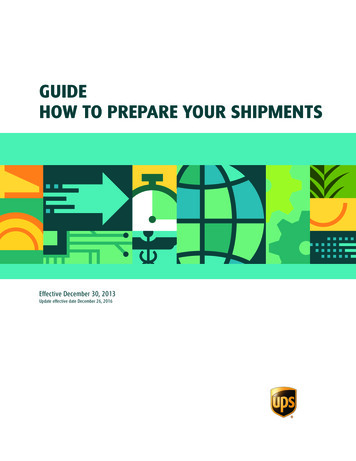
Value Plan ‒ Tier 1 Initial Coverage Cost-Sharing by loradoConnecticutDelawareDistrict of sMichiganMinnesotaMississippiMissouriPreferred RetailPharmacy30-daysupply 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 160-daysupply 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 290-daysupply 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3Standard RetailPharmacy30-daysupply 19 19 19 19 10 19 19 10 10 19 19 19 19 19 10 19 19 10 19 10 10 19 10 19 19 191060-daysupply 38 38 38 38 20 38 38 20 20 38 38 38 38 38 20 38 38 20 38 20 20 38 20 38 38 3890-daysupply 57 57 57 57 30 57 57 30 30 57 57 57 57 57 30 57 57 30 57 30 30 57 30 57 57 57PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 57 57 57 57 30 57 57 30 30 57 57 57 57 57 30 57 57 30 57 30 30 57 30 57 57 57
Value Plan ‒ Tier 1 Initial Coverage Cost-Sharing by State, contd.StateMontanaNebraskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaPuerto RicoRhode IslandSouth CarolinaSouth est VirginiaWisconsinWyomingPreferred RetailPharmacy30-daysupply 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 160-daysupply 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 290-daysupply 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3Standard RetailPharmacy30-daysupply 19 19 19 10 10 19 10 19 19 19 10 19 10 10 19 19 19 19 19 19 19 19 19 10 10 191160-daysupply 38 38 38 20 20 38 20 38 38 38 20 38 20 20 38 38 38 38 38 38 38 38 38 20 20 3890-daysupply 57 57 57 30 30 57 30 57 57 57 30 57 30 30 57 57 57 57 57 57 57 57 57 30 30 57PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 57 57 57 30 30 57 30 57 57 57 30 57 30 30 57 57 57 57 57 57 57 57 57 30 30 57
Value Plan ‒ Tier 2 Initial Coverage Cost-Sharing by loradoConnecticutDelawareDistrict of sMichiganMinnesotaMississippiMissouriPreferred RetailPharmacy30-daysupply 4 3 9 3 3 6 3 3 3 3 3 3 8 3 3 3 3 3 3 3 3 3 4 3 3 360-daysupply 8 6 18 6 6 12 6 6 6 6 6 6 16 6 6 6 6 6 6 6 6 6 8 6 6 690-daysupply 12 9 27 9 9 18 9 9 9 9 9 9 24 9 9 9 9 9 9 9 9 9 12 9 9 9Standard RetailPharmacy30-daysupply 20 20 20 20 15 20 20 14 14 20 20 20 20 20 17 20 20 17 20 12 14 20 12 20 20 201260-daysupply 40 40 40 40 30 40 40 28 28 40 40 40 40 40 34 40 40 34 40 24 28 40 24 40 40 4090-daysupply 60 60 60 60 45 60 60 42 42 60 60 60 60 60 51 60 60 51 60 36 42 60 36 60 60 60PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 60 60 60 60 45 60 60 42 42 60 60 60 60 60 51 60 60 51 60 36 42 60 36 60 60 60
Value Plan ‒ Tier 2 Initial Coverage Cost-Sharing by State, contd.StateMontanaNebraskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaPuerto RicoRhode IslandSouth CarolinaSouth est VirginiaWisconsinWyomingPreferred RetailPharmacy30-daysupply 3 3 4 3 3 8 3 3 3 4 3 5 3 3 3 5 3 4 3 8 3 4 5 3 3 360-daysupply 6 6 8 6 6 16 6 6 6 8 6 10 6 6 6 10 6 8 6 16 6 8 10 6 6 690-daysupply 9 9 12 9 9 24 9 9 9 12 9 15 9 9 9 15 9 12 9 24 9 12 15 9 9 9Standard RetailPharmacy30-daysupply 20 20 20 12 12 20 12 20 20 20 15 20 12 12 20 20 20 20 20 20 20 20 20 12 15 201360-daysupply 40 40 40 24 24 40 24 40 40 40 30 40 24 24 40 40 40 40 40 40 40 40 40 24 30 4090-daysupply 60 60 60 36 36 60 36 60 60 60 45 60 36 36 60 60 60 60 60 60 60 60 60 36 45 60PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 60 60 60 36 36 60 36 60 60 60 45 60 36 36 60 60 60 60 60 60 60 60 60 36 45 60
Value Plan ‒ Tier 3 Initial Coverage Cost-Sharing by loradoConnecticutDelawareDistrict of sMichiganMinnesotaMississippiMissouriPreferred RetailPharmacy30-daysupply 34 35 46 42 30 43 30 35 35 30 29 40 34 39 31 41 42 31 23 24 35 30 25 41 41 3260-daysupply 68 70 92 84 60 86 60 70 70 60 58 80 68 78 62 82 84 62 46 48 70 60 50 82 82 6490-daysupply 102 105 138 126 90 129 90 105 105 90 87 120 102 117 93 123 126 93 69 72 105 90 75 123 123 96Standard RetailPharmacy30-daysupply 47 47 47 47 47 47 47 43 43 37 35 47 45 47 40 47 47 40 28 30 43 47 32 47 47 471460-daysupply 94 94 94 94 94 94 94 86 86 74 70 94 90 94 80 94 94 80 56 60 86 94 64 94 94 9490-daysupply 141 141 141 141 141 141 141 129 129 111 105 141 135 141 120 141 141 120 84 90 129 141 96 141 141 141PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 102 105 138 126 90 129 90 105 105 90 87 120 102 117 93 123 126 93 69 72 105 90 75 123 123 96 141 141 141 141 141 141 141 129 129 111 105 141 135 141 120 141 141 120 84 90 129 141 96 141 141 141
Value Plan ‒ Tier 3 Initial Coverage Cost-Sharing by State, contd.StateMontanaNebraskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaPuerto RicoRhode IslandSouth CarolinaSouth est VirginiaWisconsinWyomingPreferred RetailPharmacy30-daysupply 41 41 39 24 24 47 20 30 41 47 30 35 21 30 30 41 41 34 42 34 30 35 35 21 30 4160-daysupply 82 82 78 48 48 94 40 60 82 94 60 70 42 60 60 82 82 68 84 68 60 70 70 42 60 8290-daysupply 123 123 117 72 72 141 60 90 123 141 90 105 63 90 90 123 123 102 126 102 90 105 105 63 90 123Standard RetailPharmacy30-daysupply 47 47 47 30 29 47 26 47 47 47 46 40 27 47 47 47 47 47 47 45 47 47 40 27 45 471560-daysupply 94 94 94 60 58 94 52 94 94 94 92 80 54 94 94 94 94 94 94 90 94 94 80 54 90 9490-daysupply 141 141 141 90 87 141 78 141 141 141 138 120 81 141 141 141 141 141 141 135 141 141 120 81 135 141PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 123 123 117 72 72 141 60 90 123 141 90 105 63 90 90 123 123 102 126 102 90 105 105 63 90 123 141 141 141 90 87 141 78 141 141 141 138 120 81 141 141 141 141 141 141 135 141 141 120 81 135 141
Value Plan ‒ Tier 4 Initial Coverage Cost-Sharing by loradoConnecticutDelawareDistrict of sMichiganMinnesotaMississippiMissouriPreferred %50%50%50%46%50%47%50%47%50%50%50%Standard rderStandardMailOrderUp to 90day supplyUp to 90day 48%50%50%50%
Value Plan ‒ Tier 4 Initial Coverage Cost-Sharing by State, contd.StateMontanaNebraskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaPuerto RicoRhode IslandSouth CarolinaSouth est VirginiaWisconsinWyomingPreferred %50%50%50%50%46%50%50%47%50%50%50%Standard rderStandardMailOrderUp to 90day supplyUp to 90day 48%50%50%50%
Value Plan ‒ Tier 6 Initial Coverage Cost-Sharing by loradoConnecticutDelawareDistrict of sMichiganMinnesotaMississippiMissouriPreferred RetailPharmacy30-daysupply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 060-daysupply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 090-daysupply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Standard RetailPharmacy30-daysupply 5 5 9 5 5 9 5 5 5 5 5 5 7 5 5 5 5 5 7 5 5 5 5 5 5 51860-daysupply 10 10 18 10 10 18 10 10 10 10 10 10 14 10 10 10 10 10 14 10 10 10 10 10 10 1090-daysupply 15 15 27 15 15 27 15 15 15 15 15 15 21 15 15 15 15 15 21 15 15 15 15 15 15 15PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 15 15 27 15 15 27 15 15 15 15 15 15 21 15 15 15 15 15 21 15 15 15 15 15 15 15
Value Plan ‒ Tier 6 Initial Coverage Cost-Sharing by State, contd.StateMontanaNebraskaNevadaNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaPuerto RicoRhode IslandSouth CarolinaSouth est VirginiaWisconsinWyomingPreferred RetailPharmacy30-daysupply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 060-daysupply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 090-daysupply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0Standard RetailPharmacy30-daysupply 5 5 9 5 5 9 6 5 5 8 5 7 5 5 5 5 5 5 5 7 5 5 7 5 5 51960-daysupply 10 10 18 10 10 18 12 10 10 16 10 14 10 10 10 10 10 10 10 14 10 10 14 10 10 1090-daysupply 15 15 27 15 15 27 18 15 15 24 15 21 15 15 15 15 15 15 15 21 15 15 21 15 15 15PreferredMailOrderStandardMailOrderUp to 90day supplyUp to 90day supply 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 15 15 27 15 15 27 18 15 15 24 15 21 15 15 15 15 15 15 15 21 15 15 21 15 15 15
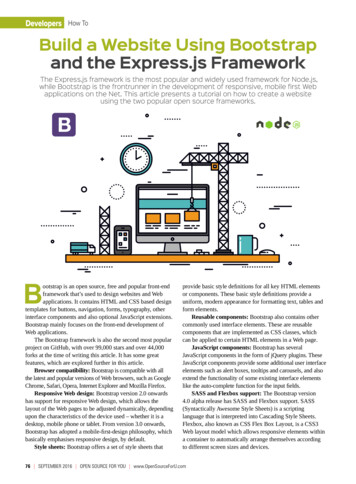
Choice Plan ‒ Tier 4 Initial Coverage Cost-Sharing by State30-day, 60-day and 90-day SuppliesPreferred Retail Pharmacy, Standard Retail Pharmacy,Preferred Mail Order, Standard Mail loradoConnecticutDelawareDistrict of daNew HampshireNew JerseyNew MexicoNew YorkNorth CarolinaNorth DakotaOhioOklahomaOregonPennsylvaniaRhode IslandSouth CarolinaSouth est 50%50%50%50%
NOTES
PRE-ENROLLMENT CHECKLISTBefore making an enrollment decision, it is important that you fully understand ourbenefits and rules. If you have any questions, you can call and speak to a CustomerService representative at 1.866.477.5704; TTY: 1.800.716.3231.UNDERSTANDING THE BENEFITSReview the pharmacy directory to make sure the pharmacy you use forany prescription medicine is in the network. If the pharmacy is not listed,you will likely have to select a new pharmacy for your prescriptions.TANDING THE BENEFITSUNDERSTANDING IMPORTANT RULESIn addition to your monthly plan premium, you must continue to pay yourMedicare Part B premium. This premium is normally taken out of yourSocial Security check each month.Benefits, premiums and/or copayments/coinsurance may change onJanuary 1, 2022.Y0046 B00SNL1A CCRP2101 004368.1
If you want to know more about the coverage and costs of Original Medicare, look in your currentMedicare & You handbook. View it online at medicare.gov or get a copy by calling 1.800.MEDICARE(1.800.633.4227), 24 hours a day, 7 days a week. TTY users should call 1.877.486.2048.Opioids (regardless of tier) and all drugs in Tier 5 are limited to a 30-day supply at all pharmacy types.All mail-order medications are priced at a 90-day cost-share, even if the prescription is writtenfor fewer days.Express Scripts Medicare’s pharmacy network includes limited lower-cost, preferred pharmacies in ruralareas in Alaska; the Saver plan also includes limited lower-cost, preferred pharmacies in suburbanareas in Puerto Rico, and the Choice plan also includes limited lower-cost, preferred pharmacies in ruralareas in Oklahoma. The lower costs advertised in our plan materials for these pharmacies may not beavailable at the pharmacy you use. For up-to-date information about our network pharmacies, includingwhether there are any lower-cost preferred pharmacies in your area, please call Customer Service at1.800.758.4574 (New York State residents: 1.800.758.4570); TTY: 1.800.716.3231, or consult theonline pharmacy directory at express-scriptsmedicare.com/2021network.ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística.Llame al 1.800.758.4574; para residentes del estado de New York: 1.800.758.4570 (TTY: 1.800.716.3231).Images are for representative purposes only and do not depict actual patients. 2020 Express Scripts. All Rights Reserved.
2021 SUMMARY OF BENEFITS January 1, 2021 - December 31, 2021 PRESCRIPTION SAVINGS WITH PLANS THAT PUT YOUR NEEDS FIRST. This booklet gives you a summary of what Express Scripts Medicare (PDP) Value, Saver and Choice plans cover and what you pay. It doesn't list every service that we cover or every limitation or exclusion.