Transcription
Alcoholism and the Brain:An OverviewMarlene Oscar-Berman, Ph.D., and Ksenija Marinkovic, Ph.D.Alcoholism can affect the brain and behavior in a variety of ways, and multiple factors caninfluence these effects. A person’s susceptibility to alcoholism-related brain damage may beassociated with his or her age, gender, drinking history, and nutrition, as well as with thevulnerability of specific brain regions. Investigators use a variety of methods to study alcoholismrelated brain damage, including examining brains of deceased patients as well as neuroimaging, atechnique that enables researchers to test and observe the living brain and to evaluate structuraldamage in the brain. KEY WORDS: neurobehavioral theory of AODU (alcohol and other drug use);alcoholic brain syndrome; brain atrophy; neuropsychological assessment; neurotransmission; riskfactors; comorbidity; disease susceptibility; neuroimaging; treatment factors; survey of researchThe brain, like most body organs,is vulnerable to injury fromalcohol consumption. The riskof brain damage and related neurobehavioral deficits varies from personto person. This article reviews themany factors that influence this risk,the techniques used to study the effectsof alcoholism1 on the brain andbehavior, and the implications of thisresearch for treatment.About half of the nearly 20 millionalcoholics in the United States seem tobe free of cognitive impairments. In theremaining half, however, neuropsychological difficulties can range from mildto severe. For example, up to 2 millionalcoholics develop permanent and debilitating conditions that require lifetimecustodial care (Rourke and Löberg 1996).Examples of such conditions includealcohol-induced persisting amnesic disorder (also called Wernicke-Korsakoffsyndrome) and dementia, which seri-1Alcohol dependence, also known as alcoholism, is characterized by a craving for alcohol, possible physical dependence on alcohol, an inability to control one’s drinking onany given occasion, and an increasing tolerance to alcohol’s effects (American Psychiatric Association [APA] 1994).Vol. 27, No. 2, 2003ously affects many mental functionsin addition to memory (e.g., language,reasoning, and problem-solving abilities) (Rourke and Löberg 1996). Mostalcoholics with neuropsychologicalimpairments show at least some improvement in brain structure and functioningwithin a year of abstinence, but somepeople take much longer (Bates et al.2002; Gansler et al. 2000; Sullivan etal. 2000). Unfortunately, little is knownabout the rate and extent to which peoplerecover specific structural and functionalprocesses after they stop drinking. However, research has helped define the variousfactors that influence a person’s risk forexperiencing alcoholism-related braindeficits, as the following sections describe.Risk Factors and ComorbidConditions That InfluenceAlcohol-Related BrainDamageAlcoholism’s effects on the brain are diverseand are influenced by a wide range ofvariables (Parsons 1996). These includethe amount of alcohol consumed, the ageat which the person began drinking, andthe duration of drinking; the patient’s age,level of education, gender, genetic background, and family history of alcoholism;MARLENE OSCAR-BERMAN, PH.D., is aprofessor in the Departments of Anatomyand Neurobiology, Psychiatry, andNeurology, Boston University School ofMedicine, and a research career scientistat the U.S. Department of VeteransAffairs Healthcare System, JamaicaPlain Division, Boston, Massachusetts.KSENIJA MARINKOVIC, PH.D., is aresearch scientist at the Athinoula A.Martinos Center for Biomedical Imaging,instructor in the Radiology Departmentat Harvard Medical School, and assistantin Neuroscience at the MassachusettsGeneral Hospital, Boston, Massachusetts.This work was supported by NationalInstitute on Alcohol Abuse and Alcoholismgrants R37–AA–07112, K05–AA–00219, K01–AA–13402, and by theMedical Research Service of the U.S.Department of Veterans Affairs.125
and neuropsychiatric risk factors such asalcohol exposure before birth and gen eral health status. Overall physical andmental health is an important factorbecause comorbid medical, neurologi cal, and psychiatric conditions caninteract to aggravate alcoholism’s effectson the brain and behavior. Examples ofcommon comorbid conditions include: Medical conditions such as malnu trition and diseases of the liver andthe cardiovascular system Neurological conditions such as headinjury, inflammation of the brain(i.e., encephalopathy), and fetal alcoholsyndrome (or fetal alcohol effects) Psychiatric conditions such as depres sion, anxiety, post-traumatic stressdisorder, schizophrenia, and the useof other drugs (Petrakis et al. 2002).Models for ExplainingAlcohol-Related BrainDamageaccompanying table lists the prevailingmodels (Oscar-Berman 2000). It shouldbe noted that the models that focus onindividual characteristics cannot be totallyseparated from models that emphasizeaffected brain systems because all ofthese factors are interrelated. Several ofthe models have been evaluated usingspecialized tests that enable researchersto make inferences about the type andextent of brain abnormalities.Some of the previously mentioned factorsthat are thought to influence how alco holism affects the brain and behaviorhave been developed into specific modelsor hypotheses to explain the variabilityin alcoholism-related brain deficits. TheModels Based on Characteristicsof Individual AlcoholicsPremature Aging Hypothesis.According to this hypothesis, alcoholismaccelerates natural chronological aging,These conditions also can contribute tofurther drinking.Hypotheses Proposed to Explain the Consequences of Alcoholism for the BrainHypotheses Emphasizing the Personal Characteristics Associated With e aging hypothesis: Alcoholism accelerates aging. Brains of alcoholicsresemble brains of chronologically old nonalcoholics. This may occur at the onsetof problem drinking (“accelerated aging”) or later in life when brains are morevulnerable (“increased vulnerability” or “cumulative effects”).GenderAlcoholism affects women more than men. Although women and men metabolizealcohol differently, it is not yet clear if women’s brains are more vulnerable thanmen’s brains to the effects of alcoholism.Family historyAlcoholism runs in families; thus, children of alcoholics face increased risk ofalcoholism and associated brain changes.Vitamin deficiencyThiamine deficiency can contribute to damage deep within the brain, leading tosevere cognitive deficits.Hypotheses Emphasizing the Vulnerability of Brain Regions or SystemsRegion/SystemHypothesisEntire brainVulnerable to cerebral atrophy.Limbic system, thalamus,and hypothalamusVulnerable to alcohol-induced persisting amnesic disorder (also known asWernicke-Korsakoff syndrome).Frontal lobe systemsMore vulnerable to the effects of alcoholism than other brain regions/systems.Right hemisphereMore vulnerable to the effects of alcoholism than the left hemisphere.*Neurotransmitter systems(e.g., gamma-aminobutyric acid (GABA),glutamate, dopamine, acetylcholine,and serotonin systems)Several neurotransmitter systems are vulnerable to effects of alcoholism.*The right hemisphere is also believed to be more vulnerable to the effects of normal aging than the left hemisphere, which is taken as support for the premature aginghypothesis listed above.NOTE: These hypotheses are not mutually exclusive; some are interrelated. Supporting data for these models come from neurobehavioral and electrophysiological studies,brain scans, and post mortem neuropathology.126Alcohol Research & Health
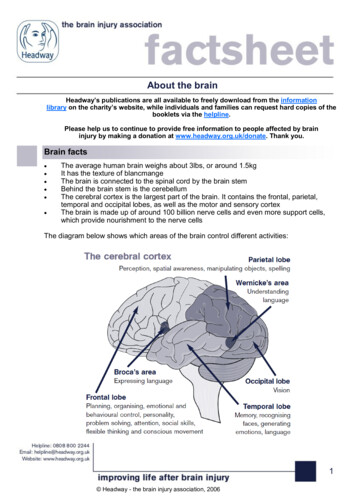
Alcoholism and the Brain: An Overviewbeginning with the onset of problemdrinking.An alternate version suggests that olderpatients (age 50 and older) are especiallysusceptible to the cumulative effects ofalcoholism, and aging is accelerated onlylater in life. The preponderance of scientificevidence suggests that although alcoholismrelated brain changes may mimic someof the changes seen in older people,alcoholism does not cause prematureaging. Rather, the effects of alcoholismare disproportionately expressed inolder alcoholics (Oscar-Berman 2000).Gender. Although it has been hypothe sized that women’s brain functioningis more vulnerable to alcoholism thanmen’s, studies of gender differenceshave not consistently found this to betrue (see Wuethrich 2001 for a review),even though women and men metabo lize alcohol differently (i.e., womenachieve higher blood alcohol contents[BACs] than men after consuming thesame amount of alcohol). However, itis not known whether this comparisonbetween men and women holds amongolder populations (Oscar-Berman 2000).Family History. Family history of alco holism has been found to be importantbecause it can influence such things astolerance for alcohol and the amount ofconsumption needed to feel alcohol’seffects. Also, studies examining brainfunctioning in people with and withouta positive family history of alcoholismhave shown that there are clear differ ences between the groups on measuresof brain electrical activity (Porjesz andBegleiter 1998).Vitamin Deficiency. Research on mal nutrition, a common consequence ofpoor dietary habits in some alcoholics,indicates that thiamine deficiency (vita min B1) can contribute to damage deepwithin the brain, leading to severe cog nitive deficits (Oscar-Berman 2000).The exact location of the affected partsof the brain and underlying neuro pathological mechanisms are still beingresearched (see the next section).Models Based on VulnerableBrain SystemsThe outer, convoluted layer of braintissue, called the cerebral cortex or thegray matter, controls most complex men tal activities (see figure 1). Just beneathit are the nerve fibers, called the whitematter, that connect different corticalCerebral cortex{Parietal lobeCorpus usCerebellumHippocampal TemporalregionslobeFigure 1 Schematic drawing of the human brain, showing regions vulnerable toalcoholism-related abnormalities.Vol. 27, No. 2, 2003regions and link cortical cells with otherstructures deep inside the brain (sub cortical regions).Areas of the brain that are especiallyvulnerable to alcoholism-related damageare the cerebral cortex and subcorticalareas such as the limbic system (impor tant for feeling and expressing emotions),the thalamus (important for communi cation within the brain), the hypothalamus(which releases hormones in response tostress and other stimuli and is involvedin basic behavioral and physiologicalfunctions), and the basal forebrain (thelower area of the front part of the brain,involved in learning and memory)(Oscar-Berman 2000). Another brainstructure that has recently been impli cated is the cerebellum (Sullivan 2000),situated at the base of the brain, whichplays a role in posture and motor coor dination and in learning simple tasks.Alcohol-Related Brain Atrophy.According to one hypothesis, shrinkage(i.e., atrophy) of the cerebral cortex andwhite matter, as well as possible atrophyof basal forebrain regions, may resultfrom the neurotoxic effects of alcohol(Lishman 1990). Furthermore, thiaminedeficiency may result in damage to portionsof the hypothalamus (perhaps becauseblood vessels break in that region).According to this hypothesis, alcoholicswho are susceptible to alcohol toxicity2may develop permanent or transientcognitive deficits associated with brainshrinkage. Those who are susceptibleto thiamine deficiency will develop amild or transient amnesic disorder, withshort-term memory loss as the salientfeature. Patients with dual vulnerability,those with a combination of alcoholneurotoxicity and thiamine deficiency,will have widespread damage to largeregions of the brain, including structuresdeep within the brain such as the lim bic system. These people will exhibitsevere short-term memory loss and col lateral cognitive impairments (OscarBerman 2000).Frontal Lobe Vulnerability. Althoughalcoholics have diffuse damage in the2Some people may have better immunity than others toalcohol’s toxic effects.127
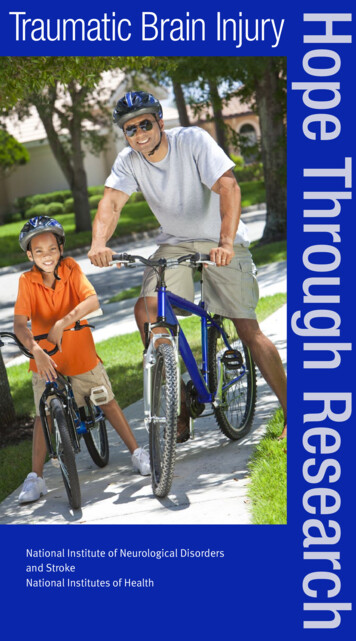
cerebral cortex of both hemispheresof the brain, neuropathological studiesperformed on the brains of deceasedpatients as well as findings derived fromneuroimaging studies of living brainspoint to increased susceptibility of frontalbrain systems to alcoholism-related dam age (Moselhy et al. 2001; Oscar-Berman2000; Sullivan 2000). The frontal lobesare connected with all other lobes ofthe brain (i.e., the parietal, temporal,and occipital lobes on both halves ofthe brain; see figure 1), and they receiveand send fibers to numerous subcorticalstructures. Behavioral neuroscientistshave determined that the anterior regionof the frontal lobes (i.e., the prefrontalcortex) is important for engaging inordinary cognitive, emotional, andinterpersonal activities. The prefrontalcortex is considered the brain’s executive—that is, it is necessary for planning andregulating behavior, inhibiting theoccurrence of unnecessary or unwantedbehaviors, and supporting adaptive“executive control” skills such as goaldirected behaviors, good judgment,and problem-solving abilities. Disruptionsof the normal inhibitory functions ofprefrontal networks often have theinteresting effect of releasing previouslyinhibited behaviors. As a result, a personmay behave impulsively and inappro priately, which may contribute toexcessive drinking.There is evidence that the frontallobes are particularly vulnerable toalcoholism-related damage, and thebrain changes in these areas are mostprominent as alcoholics age (OscarBerman 2000; Pfefferbaum et al. 1997;Sullivan 2000) (see figure 2). Otherstudies of frontal lobe function in olderalcoholics have confirmed reports ofa correlation between impaired neuro psychological performance (e.g., execu tive control skills, as noted above)and decreased blood flow or metabolism(energy use) in the frontal lobes, as seenusing neuroimaging techniques (Adamset al. 1998).Vulnerability of the Right Hemisphere.Some investigators have hypothesizedthat functions controlled by the brain’sright hemisphere are more vulnerableto alcoholism-related damage than thosecarried out by the left hemisphere (seeOscar-Berman and Schendan 2000 forreview). Each hemisphere of the humanbrain is important for mediating differ ent functions. The left hemisphere hasa dominant role in communication andin understanding the spoken and writtenword. The right hemisphere is mainlyinvolved in coordinating interactionswith the three-dimensional world (e.g.,spatial cognition).Differences between the two cerebralhemispheres can easily be seen in patientswith damage to one hemisphere but notthe other (from stroke, trauma, or tumor).Patients with left hemispheric damageoften have problems with language;patients with right hemispheric damageoften have difficulty with maps, designs,music, and other nonlinguistic materials,and they may show emotional apathy.Alcoholics may seem emotionally“flat” (i.e., they are less reactive to emo tionally charged situations), and mayCortical Gray Matter Volumes157-year-old menAlcoholicControl SubjectYounger Alcoholics (N 33)Older Alcoholics (N 29)Control SubjectsZ-score0-1Lifetime consumption of alcohol was1866 kgor 625 gallons60 kgor 20 rietal OccipitalFigure 2 Brain MRI scans of age-equivalent men with different histories of alcohol use. The image shows clear evidence ofbrain shrinkage in the alcoholic compared with the control subject. The graph on the right shows that older alco holics have less cortical tissue than younger alcoholics, and that the prefrontal cortex is especially vulnerable toalcohol’s effects. The location of the temporal, parietal, and occipital regions of the brain can be seen in figure 1.*Z-score is a mathematical measure that is useful for showing the difference between the recorded value and a “normal” value.SOURCE: Pfefferbaum et al. 1997.128Alcohol Research & Health
Alcoholism and the Brain: An Overviewhave difficulty with the same kinds oftasks that patients with damage to theright hemisphere have difficulty with.New research has shown that alcoholicsare impaired in emotional processing,such as interpreting nonverbal emotionalcues and recognizing facial expressionsof emotion (Kornreich et al. 2002;Monnot et al. 2002; Oscar-Berman 2000).Yet, despite the fact that emotionalfunctioning can be similar in some alco holics and people with right hemi sphere damage, research provides onlyequivocal support for the hypothesis thatalcoholism affects the functioning of theright hemisphere more than the left(Oscar-Berman and Schendan 2000).Impairments in emotional functioningthat affect alcoholics may reflect abnor malities in other brain regions which alsoinfluence emotional processing, such asthe limbic system and the frontal lobes.Disruption of NeurotransmitterSystems. Brain cells (i.e., neurons)communicate using specific chemicalscalled neurotransmitters. Neuronalcommunication takes place at thesynapse, where cells make contact.Specialized synaptic receptors on thesurface of neurons are sensitive to spe cific neurotransmitters. Alcohol canchange the activity of neurotransmittersand cause neurons to respond (excitation)or to interfere with responding (inhibi tion) (Weiss and Porrino 2002), anddifferent amounts of alcohol can affectthe functioning of different neuro transmitters. Over periods of days andweeks, receptors adjust to chemical andenvironmental circumstances, such as thechanges that occur with chronic alcoholconsumption, and imbalances in theaction of neurotransmitters can result inseizures, sedation, depression, agitation,and other mood and behavior disorders.The major excitatory neurotransmitterin the human brain is the amino acidglutamate. Small amounts of alcoholhave been shown to interfere with glu tamate action. This interference couldaffect several brain functions, includingmemory, and it may account for theshort-lived condition referred to as“alcoholic blackout.” Chronic alcoholconsumption increases glutamatereceptor sites in the hippocampus, anVol. 27, No. 2, 2003area in the limbic system that is crucialto memory and often involved in epilep tic seizures. During alcohol withdrawal,glutamate receptors that have adaptedto the long-term presence of alcoholmay become overactive, and this over activity has been repeatedly linked toneuronal death, which is manifested byconditions such as stroke and seizures.Deficiencies of thiamine caused bymalnutrition may contribute to thispotentially destructive overactivity(Crews 2000).Gamma-aminobutyric acid (GABA)is the major inhibitory neurotransmitter.Available evidence suggests that alcohol3initially potentiates GABA’s effects (i.e.,it increases inhibition, and often thebrain becomes mildly sedated). However,over time, prolonged, excessive alcoholconsumption reduces the number ofGABA receptors. When the person stopsdrinking, decreased inhibition combinedwith a deficiency of GABA receptorsmay contribute to overexcitation through out the brain. This in turn can con tribute to withdrawal seizures within aday or two. It should be noted that thebalance between the inhibitory actionof GABA and the excitatory action ofglutamate is a major determinant of thelevel of activity in certain regions of thebrain; the effects of GABA and gluta mate on withdrawal and brain functionare probably interactive (see Valenzuela1997 for review).Alcohol directly stimulates release ofthe neurotransmitter serotonin, whichis important in emotional expression,and of the endorphins, natural substancesrelated to opioids, which may contributeto the “high” of intoxication and thecraving to drink. Alcohol also leads toincreases in the release of dopamine (DA),a neurotransmitter that plays a role inmotivation and in the rewarding effectsof alcohol (Weiss and Porrino 2002).Changes in other neurotransmitters suchas acetylcholine have been less consis tently defined. Future research shouldhelp to clarify the importance of manyneurochemical effects of alcohol con sumption. Furthermore, areas amenableto pharmacological treatment could be3The amount of alcohol needed to cause this effectdepends on the person.identified by studying regionally specificbrain neurochemistry in vivo usingneuroimaging methods such as positronemission tomography (PET) and singlephoton emission computerized tomog raphy (SPECT) (described below).New information from neuroimag ing studies could link cellular changesdirectly to brain consequences observedclinically. In the absence of a cure foralcoholism, a detailed understanding ofthe actions of alcohol on nerve cells mayhelp in designing effective therapies.Techniques for StudyingAlcohol-Related BrainDamageResearchers use multiple methods tounderstand the etiologies and mecha nisms of brain damage across subgroupsof alcoholics. Behavioral neuroscienceoffers excellent techniques for sensi tively assessing distinct cognitive andemotional functions—for example, themeasures of brain laterality (e.g., spatialcognition) and frontal system integrity(e.g., executive control skills) mentionedearlier. Followup post mortem examina tions of brains of well-studied alcoholicpatients offer clues about the locus andextent of pathology and about neuro transmitter abnormalities. Neuroimagingtechniques provide a window on theactive brain and a glimpse at regions withstructural damage.Behavioral NeuroscienceBehavioral neuroscience studies therelationship between the brain and itsfunctions—for example, how the braincontrols executive functions and spatialcognition in healthy people, and howdiseases like alcoholism can alter thenormal course of events. This is accom plished by using specialized tests designedexpressly to measure the functions ofinterest. Among the tests used by scientiststo determine the effects of alcoholismon executive functions controlled bythe frontal lobes are those that measureproblem-solving abilities, reasoning,and the ability to inhibit responses thatare irrelevant or inappropriate (Moselhyet al. 2001; Oscar-Berman 2000). Tests129
to measure spatial cognition controlledby the right hemisphere include thosethat measure skills important for recog nizing faces, as well as those that rely onskills required for reading maps andnegotiating two- and three-dimensionalspace (visuospatial tasks) (Oscar-Bermanand Schendan 2000). With the adventof sophisticated neuroimaging techniques(described below), scientists can evenobserve the brain while people performmany tasks sensitive to the workings ofcertain areas of the brain.NeuropathologyResearchers have gained importantinsights into the anatomical effectsof long-term alcohol use from studyingthe brains of deceased alcoholic patients.These studies have documentedalcoholism-related atrophy throughoutthe brain and particularly in the frontallobes (Harper 1998). Post mortemstudies will continue to help researchersunderstand the basic mechanisms ofalcohol-induced brain damage andregionally specific effects of alcoholat the cellular level.NeuroimagingRemarkable developments in neuroimag ing techniques have made it possible tostudy anatomical, functional, and bio chemical changes in the brain that arecaused by chronic alcohol use. Becauseof their precision and versatility, thesetechniques are invaluable for studyingthe extent and the dynamics of braindamage induced by heavy drinking.Because a patient’s brain can be scannedon repeated occasions, clinicians andresearchers are able to track a person’simprovement with abstinence anddeterioration with continued abuse.Furthermore, brain changes can becorrelated with neuropsychologicaland behavioral measures taken at thesame time. Brain imaging can aid inidentifying factors unique to theindividual which affect that person’ssusceptibility to the effects of heavydrinking and risk for developing depen dence, as well as factors that contributeto treatment efficacy.130Imaging of Brain Structure. Withneuroimaging techniques such as com puterized tomography (CT) and mag netic resonance imaging (MRI), whichallow brain structures to be viewedinside the skull, researchers can studybrain anatomy in living patients. CTscans rely on x-ray beams passingthrough different types of tissue in thebody at different angles. Pictures of the“inner structure” of the brain are basedon computerized reconstruction of thepaths and relative strength of the x-raybeams. CT scans of alcoholics haverevealed diffuse atrophy of brain tissue,with the frontal lobes showing the ear liest and most extensive shrinkage(Cala and Mastaglia 1981).MRI techniques have greatly influ enced the field of brain imaging becausethey allow noninvasive measurementof both the anatomy (using structuralMRI) and the functioning (using func tional magnetic resonance imaging[fMRI], described below) of the brainwith great precision. Structural MRIscans are based on the observation thatthe protons derived from hydrogenatoms, which are richly represented inthe body because of its high water con tent, can be aligned by a magnetic fieldlike small compass needles. When pulsesare emitted at a particular frequency,the protons briefly switch their alignmentand “relax” back into their original stateat slightly different times in differenttypes of tissue. The signals they emit aredetected by the scanner and convertedinto highly precise images of the tissue.MRI methods have confirmed andextended findings from post mortemand CT scan studies—namely, thatchronic use of alcohol results in brainshrinkage. This shrinkage is most markedin the frontal regions and especially inolder alcoholics (Oscar-Berman 2000;Pfefferbaum et al. 1997; Sullivan 2000).Other brain regions, including portionsof the limbic system and the cerebel lum, also are vulnerable to shrinkage.Imaging of Brain Function: Hemodynamic Methods. Hemodynamicmethods create images by trackingchanges in blood flow, blood volume,blood oxygenation, and energy metab olism that occur in the brain in responseto neural activity. PET and SPECT areused to map increased energy consump tion by the specific brain regions that areengaged as a patient performs a task.One example of this mapping involvesglucose, the main energy source for thebrain. When a dose of a radioactivelylabeled glucose (a form of glucose thatis absorbed normally but cannot befully metabolized, thus remaining“trapped” in a cell) is injected into thebloodstream of a patient performing amemory task, those brain areas thataccumulate more glucose will be impli cated in memory functions. Indeed,PET and SPECT studies have confirmedand extended earlier findings that theprefrontal regions are particularly sus ceptible to decreased metabolism in alco holic patients (Berglund 1981; Gilmanet al. 1990). It is important to keep inmind, however, that frontal brain sys tems are connected to other regions ofthe brain, and frontal abnormalities maytherefore reflect pathology elsewhere(Moselhy et al. 2001).Even though using low doses ofradioactive substances that decay quicklyminimizes the risks of radiation expo sure, newer and safer methods haveemerged, such as MRI methods. MRIis noninvasive, involves no radioactiverisks, and provides both anatomicaland functional information with highprecision. The fMRI method is sensi tive to metabolic changes in the partsof the brain that are activated duringa particular task. A local increase inmetabolic rate results in an increaseddelivery of blood and increased oxy genation of the region participating ina task. The blood oxygenation level–dependent (BOLD) effect is the basisof the fMRI signal. Like PET andSPECT, fMRI permits observing thebrain “in action,” as a person performscognitive tasks or experiences emotions.In addition to obtaining structuraland functional information about thebrain, MRI methodology has beenused for other specialized investigationsof the effects of alcohol on the brain.For example, structural MRI can clearlydelineate gray matter from white matterbut cannot detect damage to individualnerve fibers forming the white matter.By tracking the diffusion of water molAlcohol Research & Health
Alcoholism and the Brain: An Overviewecules along neuronal fibers, an MRItechnique known as diffusion tensorimaging (DTI) can provide informationabout orientations and integrity of nervepathways, confirming earlier findings frompost mortem studies which suggested thatheavy drinking disrupts the microstruc ture of nerve fibers. Moreover, the find ings correlate with behavioral tests ofattention and memory (Pfefferbaumet al. 2000). These nerve pathways arecritically important because thoughts andgoal-oriented behavior depend on theconcerted activity of many brain areas.Another type of MRI application,magnetic resonance spectroscopy imag ing (MRSI), provides informationabout the neurochemistry of the livingbrain. MRSI can evaluate neuronalhealth and degeneration and can detectthe presence and distribution of alcohol,certain metabolites, and neurotransmitters.Imaging of Brain Function: Electromagnetic Methods. In spite of theirexcellent spatial resolution—that is,the ability to show precisely where theactivation changes are occurring in thebrain—hemodynamic methods such asPET, SPECT, and fMRI have limita tions in showing the time sequence ofthese changes. Activation maps can revealbrain areas involved in a particular task,but they cannot show exactly when theseareas made their respective contributions.This is because they measure hemodynamicchanges (blood flow and oxygenation),indicating the neuronal activation onlyindirectly and with a lag of more than asecond. Yet, it is important to under stand the order and timing of thoughts,feelings, and behaviors, as well as thecontributions of different brain areas.The only methods capable of onlinedetection of the electrical currents inneuronal activity are electromagneticmethods such electroencephalography(EEG), event-related brain potent
eral health status. Overall physical and mental health is an important factor because comorbid medical, neurologi cal, and psychiatric conditions can interact to aggravate alcoholism's effects on the brain and behavior. Examples of common comorbid conditions include: Medical conditions such as malnu trition and diseases of the liver and