Transcription
Revenue Cycle ManagementBKD Tuesdays at Ten Webinar SeriesDecember 8, 2020
Today’s PresentersBrian O’ReillyBrenda ChristmanRyan RozwatDeb KozlowskiPartnerManaging DirectorSeniorManaging ConsultantSeniorManaging Consultant
What toExpect21Current Operating Environment2Revenue Cycle Management 1013Front, Middle, Back4Effectively Managing RCM5Q&A
Current EnvironmentDisruptions Due to Pandemic Increase in Expenses Heroes pay OT PPE & Cleaning supplies Technology Loss of Volume efficiencies Transportation Day Services Clinic SEIT/EI3 Decline in Revenue Residential vacancies Difficulty in filling Day programs under utilized End of RetainerPayments Property funding Low enrollment in Educationprograms 1 to 1 Aide funding changes
CurrentEnvironment NYS Budget Problems Trouble before the Pandemic 2% across the board cuts Currently projected 16B shortfall Governor’s call for 5% cuts for all Departments Trouble after the Pandemic Years to rebuild tax base4
CurrentEnvironmentImpact onFunding –Changes toFunding5 Elimination of Vacancy days & Reduction to Retainer &Therapeutic Leave days Reduction of 5% for residential agenciesReducing expenses doesn’t workDecertifying beds doesn’t workFilling beds with inappropriate placement doesn’t work20% WithholdAdditional cuts could be comingChanges being discussed for Rate RationalizationWaiver modification to make telehealth permanentDelays in payments – Additional Medicaid Lag
Current EnvironmentMove to Managed Care SIPs-PL Starting 2021 Voluntary enrollment initially Mandatory within 1 to 2 years Transition from Fee for service Value Based Payments SIPS-M Possible Geographic areas withinadequate coverage6 Managed Care System Multiple payors Different billing rules &requirements Increased billing compliance Different timelines Initial Billing Re-billings Payment cycles Negative impact Cash Flows
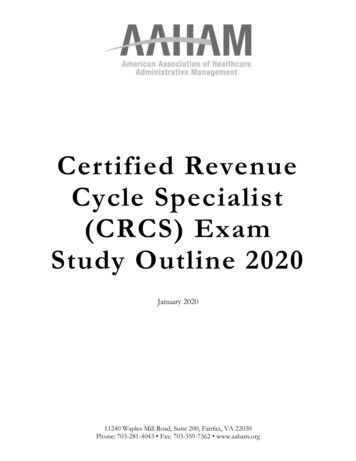
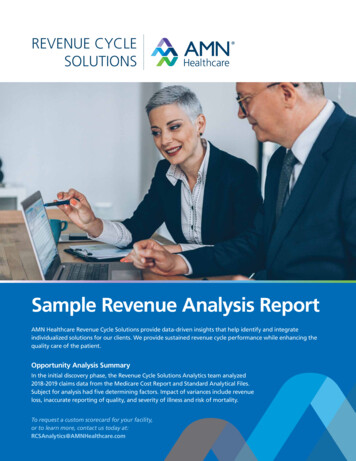
REVENUE CYCLE MANAGEMENTFront- EndAdmissions /Access:Pre-Service Scheduling Pre-Registration FinancialCounseling Medicaid &CharityApplicationAdmissions /Access: ServiceDate Registration InsuranceVerification PreCertification /Authorization FinancialCounseling StaffDeploymentValue:Efficient processes to control financialrisk, improve accuracy of collectiondata. Reduced denials from accessareas.7MiddleBack-EndHIM/CDI: Coding& CDIRevenue Integrity:Charge Capture &PricingBusiness Office:Billing Clinicaldocumentationimprovement(CDI) ICD-10 &HCPCScoding MedicalRecords Cost Reportoptimization Charge capturereconciliation Chargemaster Pricingrationalization CDMStandardization Managed Carepricing /Contracting Claimsubmission Claim Edits &Billing Electronic billing Billing backlogreduction Claim RejectionValue:Improve net revenue from chargecapture, clinical documentationimprovement & managed carecontracting & pricing.Business Office:Follow-Up AccountsReceivablemanagement Denialsmanagement Insurance FollowUp VendorManagement Cash Posting Self PayCollectionsValue:Improved days in A/R, accelerated cashflow. Reduced cost to collect, bad debt &satisfaction scores from business officeprocesses.Revenue CycleManagement(RCM) is processused by health caresystems to trackrevenue forservices providedfrom initialencounter to finalpayment of balance
REVENUECYCLEOVERVIEW8
REVENUE CYCLE TEAMRevenue Cycle success depends on active involvement & contribution from all areas of the organization.Revenue Cycle StaffAdmissions AccessBillingDenialsCoding/HIMCase Management9Clinical StaffSupport staffPhysician ChampionITService Line LeadersManaged CareDepartment managersPharmacyLeadership to drive the changeProcess owners to implement the changeQuality
WHAT ARE THE KEY RESPONSIBILITIES OF THEFRONT END OF THE REVENUE CYCLE?All administrative & clinical functions that contribute to the capture, management & collection ofservice revenue prior to and/or at time of serviceGeneral Elements of “Front End” Revenue Cycle Counseling Service Request &Entry Receiving/Sendingrequests to schedule Entering & resolving individual& order information issues Check-in & admissionprocess Attaching & StoringOrders Entering individualinformation & BookingAppointments Insurance, Auth, MedicalNecessity, individualdemographic verification Entering & resolvingindividual & orderinformation Determiningeligibility &providingenrollment supportfor assistanceprograms Relay Instructions Communicating individualliability estimates & referral toF.C. Communicating &Collecting individualliability Communicateindividual liabilityestimates Medical Necessity Distributing Appointmentor Service Reminders
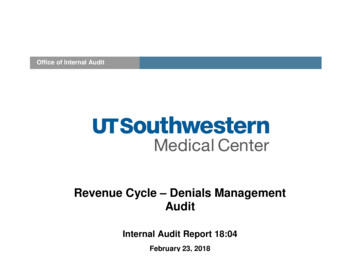
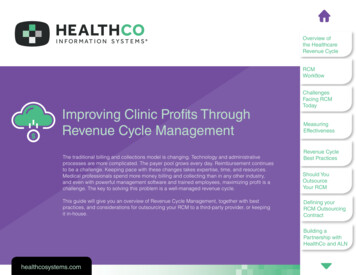
WHY IS THE FRONT END OF THE REVENUE CYCLEIMPORTANT?The snowball represents amount of reworkrequired to create accurate bill if earlier stagesof Revenue Cycle collected inaccurate gistrationCodingDenial ManagementPayment PostingChargeCaptureFinancialClaims ProcessingAccount Resolution& EntryCounseling
BEST PRACTICE CHECKLIST FOR INDIVIDUALSCHEDULING & PRE-REGISTRATION Have clearly defined & written policies & procedures for customer intake & scheduling Have multiple easy to use avenues exist for an individual to request & schedule service aswell as ask questions (online portal, phone & fax) Assist uninsured individuals by scheduling a meeting with financial counselors to completefinancial assistance applications Provider appointment reminder calls to individuals for any day services Validate both insurance & benefit information using electronic insurance portals & callinginsurance plans if results are unclear for clarification Optimize electronic medical & scheduling systems to allow for electronic based task lists tohelp with completing & monitoring completion of financial clearance12
BEST PRACTICE FOR REGISTRATION & CREDENTIALING Re-verify individual demographic information (each service or on a consistentcadence) Re-verify individual insurance & benefit information & ask for copy of insurancecard to scan in Establish friendly customer service scripting Optimize electronical medica records systems for easy information retrieval &ability to see completion of financial clearance activities Perform timely credentialing with payers (Medicaid & HMO’s) & establish13reporting to monitor & track until completion (prior to any services performed)
FRONT END REVENUE CYCLE MEASUREMENT &REPORTING BEST PRACTICES Establish Productivity & Quality Metrics for front end revenue cycle staff Establish performance metrics & trending reports to measure team & department g indicator that individuals are financially cleared &ready prior to serviceCalculationBenchmarkNumber of encounters pre-registered /Number of scheduled encounter 98%Trending indicator that customer access functions are timely,accurate & efficient; verified encounters are total of monthlyscheduled encounters that have been verified prior to or at timeNumber of verified encounters /InsuranceNumber of registered encountersVerification Rate of service & non-scheduled encounters verified within one (1)day of service or date of admission. A successful verification isdefined by individual organization policyTrending indicator of response time for requests to schedule or% of calls answered within 80 seconds or lessCall Wait Timequestions about serviceAuth Rate14Trending indicator of authorization rate# of Outpatient Encounters Authorized / # ofOutpatient Encounters Requiring Authorization 98%85% 98%
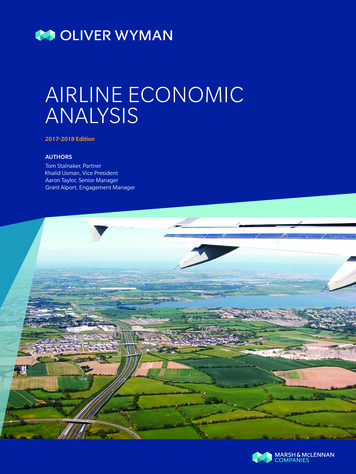
Why Is the Middle Revenue Cycle Important?1. COMPLIANCE2. REIMBURSEMENTCHARGEDESCRIPTIONMASTER (CDM)MAINTENCECHARGECAPTURE AIMSSUBMISSION )
BEST PRACTICES FOR CHARGE CAPTURE, CODING &CLINICAL DOCUMENTATION IMPROVEMENT (CDI) Establish daily charge entry reconciliation process to ensure all charges arecapture for services that are scheduled & performed (review againstdocumentation &/or schedule) Establish daily claims reconciliation process to ensure bills have been submitted& received for all services rendered Optimize system claim scrubber & coding “edits” to identify & flag common errorsfor resolution prior to claim submission Measure charge entry lag days (days from date of service to charge entry) &develop a prevention plan to reduce or resolve delays impacting timely16 reimbursement
BEST PRACTICES FOR CHARGE CAPTURE, CODING & CLINICALDOCUMENTATION IMPROVEMENT (CDI) Use concurrent coding to improve medical necessity documentation Conduct regular chart audits to ensure documentation is compliant &maximizing reimbursement Hold quarterly meetings to review & update charge description masterto eliminate missed charge capture opportunities or billing errors &delays that may be caused by CDM set-up17
MIDDLE REVENUE CYCLE MEASUREMENT &REPORTING BEST PRACTICES Establish Productivity & Quality Metrics for revenue integrity functions Establish performance metrics & trending reports to measure team, staff & department performanceMeasurementDefinitionCharge Lag Trending indicator that charges areDaysbeing entered timelyCalculationBenchmarkAverage # of days it takes fromdate of service for charges tobe posted or entered into thesystem 3*average calculated weekly/monthlyCodingTrending indicator of staff codingProductivity productivity18Number of charts reviewed &coded per hour10-20/hr
WHAT ARE THE KEY RESPONSIBILITIES OF THE BACKEND OF THE REVENUE CYCLE?General Elements of “Back End” Revenue Cycle ProcessBilling Claim Creation &Submission. Claim Edits creation& correction withappropriatedepartments.Follow Up Management &monitoring ofoutstandingreceivables. Claim StatusInquiries. Application of Client Working with payersfor delays to claimStatements Process.payment/responses.DenialsCash Posting Reviewing denial root cause &mitigation needed to address & appeal. Automatic & manualpostings of remittances &reconciliation to bankdeposits. Determination action needed on fataldenials to adjust off appropriately, whenrequired, or adjust to the individualresponsibility. Evaluate underpayments & work withpayers when payment terms are notmet. Application of payments &adjustments forappropriate individualbalances. Month end reconciliation &reporting.Over 80% of your organization’s services should be submitted on a claim to payer without needing any manualintervention. One goal of back end revenue cycle: utilize technology & processes to improve that figure, whiledeveloping processes to address claims that do require intervention.
BEST PRACTICE: BILLING & FOLLOW UPBilling Stratify accounts by amount Separate Medicare from commercial accounts Define & develop policies & procedures forbilling guidelines Educate staff on: Payer Contract Requirements How to verify insurance coverage Payer Specific billing requirements Monitoring timely filing of claims in accordancewith payer requirementsFollow Up / Denials Clearly defined revenue cycle & clinical documentationpolicies & procedures Design a team of individuals to appeal denials forreconsideration of payments Ensure all outstanding claims are reviewed every 30 days Develop, implement & monitor performance of appealsfor denials received & appeal success rates Monitor denials for reporting & resolution by: PayerDenial TypeReasonRoot CauseAppeal Success Rate Monitoring timely filing of claims in accordance withpayer requirements for appealing claims
Denials Improvement Denial results in the provider receivingSamples: Remittance & Denial Categoriesless reimbursement for services thananticipated/contractually agreed upon 3.3% hospital net revenue lost dueto claim denials1 118 average cost to formally appeala denied claim1 Denials Management begins with understanding denials receivedStart by identifying largest denial writeoffs & remittance code associated withdenial(s) receivedIdentify root cause & opportunity toprevent/mitigate fatal denial write offs &improve metric to benchmark1Statisticscited from Change Healthcare Study 2016Denial CategoryDenial Category DescriptionSampleRemittance CodesNot MedicallyNecessaryServices determined as being not medically necessary,does not support level of services provided, additionaldocumentation will be required.Coordination ofBenefits /RegistrationDenials due to individual unidentified as insured, servicesprovided prior to or after coverage terminated, max benefitsfor services have been reached273, 31, 32Timely FilingEither the initial claim submission or the appeal of the claimdenial was not made within payer specific timely filing limitdeadlines29, 164, 16640, 50
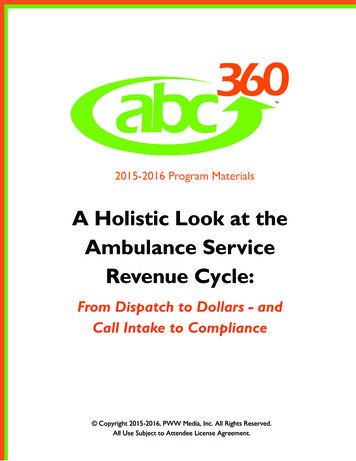
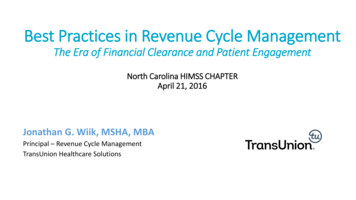
CASH POSTING WORKFLOW MATTERSTrue Cost of Cash PostingProviderResourcesper ClaimElectronicPayment ManualRemitPaperCheck ElectronicRemitElectronicPayment ElectronicRemitPaymentProcessingTime & Cost5 minutes3 minutes5 minutes3 minutes 2.51 1.51 2.51 1.51RemittanceProcessingTime & Cost7 minutes7 minutes2 minutes2 minutes 3.76 3.76 1.21 1.2112 minutes10 minutes7 minutes5 minutes 6.27 5.27 3.72 2.72 47,025 39,525 27,900 20,400Resourcesper ClaimCost per7500 Claims22PaperCheck ManualRemitSource: 2019 CAQH Index Report
EFFECTIVELYMANAGEYOURREVENUECYCLE Assess your Revenue Cycle, End-to-End Know your Key Performance Indicators (KPIs) & definetargets for improvement with a Dashboard Change Management: Adopt Culture of AccountabilityOrganization-wide Develop SMART goals for specific departments Establish Clear Ownership Structure for each componentof the Revenue Cycle23
BACK END REVENUE CYCLEMEASUREMENT & REPORTING BEST Clean Claim RateTrending indicator of claims data, indicates quality ofdata collected & reported, including direct submissions tothird-party payersNumber of claims that pass edits requiring nomanual intervention / Number of claims acceptedinto claims processing tool for billing 85%Days in ARTrending indicator of overall AR performanceInsurance AR over Trending indicator of receivable collectability, indicates revenue90 dayscycle effectiveness at liquidating A/R.Trending indicator of effectiveness of self-pay collection efforts;Bad Debt & Charityfinancial counseling, organization's ability to collect self-payas % of Grossaccounts, identification of payer sources & charity for thoseRevenueindividuals unable to payInitial Denial RateTrending indicator of % claims denied, indicates provider'sability to comply with payer requirements & payer's ability toaccurately pay the claimTrending indicator of lost reimbursement, all appeal effortsDenial Write Offs as exhausted, or provider chooses to write off, indicates provider's% of Net Revenue ability to comply with payer requirement & payer's ability to payaccurately24Gross AR / Average Daily Gross Revenue 90 Days from Discharge Date /Total Billed A/R 40.6 Days(Total Charity Care Total Bad Debt) /Gross Patient Service Revenue 2.5%Total number of claims denied /Total number of claims remitted 4%Net dollars written off monthly as denials /Average Monthly Net Patient Service Revenue 2% 20.6%
25Brian O’Reilly, CPAPartner BKD CPAs & Advisors212.867.4000, ext. 13123boreilly@bkd.comBrenda Christman, RN, MHAManaging Director BKD CPAs & AdvisorsHealth Care Performance Advisory Services513.621.8300 Ext 30457bchristman@BKD.comDeb Kozlowski, CPASenior Managing Consultant BKD CPAs & AdvisorsHealth Care Performance Advisory Services312.270.2521 Directdkozlowski@BKD.comRyan Rozwat, CHFPSenior Managing Consultant BKD CPAs & AdvisorsHealth Care Performance Advisory Services630.282.9674 Ext 23713trozwat@BKD.com
Tuesday, October 27 – COVID CFR Reporting Tuesday, November 10 – IDD & Behavioral Health Care Providers –Wading Through the CARES Act Tuesday, November 24 – Cash Flow Management & Budgeting Tuesday, December 8 – Revenue Cycle Management Tuesday, December 22 – IDD/BH MergersRegister at Tuesdays at Ten Webinar Series
REVENUE CYCLE 23 Assess your Revenue Cycle, End-to-End Know your Key Performance Indicators (KPIs) & define targets for improvement with a Dashboard Change Management: Adopt Culture of Accountability Organization-wide Develop SMART goals for specific departments Establish Clear Ownership Structure for each component of the Revenue Cycle