Transcription
Best of AASLD &DDW 2019December 14th, 2019
Best of AASLD and DDW 2019Table of ContentsItemPageAgenda3Acknowledgements4Speaker Biographies5Speaker Disclosures9Presentation Handouts:Liver Transplantation10Non-Viral Liver Disease18Liver Cancer23Pancreas-Biliary Tree28Portal Hypertension38Motility and Functional Bowel Disease49Colon Cancer55Inflammatory Bowel Disease65
Best of AASLD and DDW 2019AgendaStartEndTopic7:30 AM8:00 AMRegistration/Breakfast8:00 AM8:05 AMOpening RemarksDekey Lhewa, MD8:05 AM8:30 AMLiver TransplantationMichael Chang, MD, MS, MBA8:35 AM9:00 AMNon‐Viral Liver DiseaseArnab Mitra, MD9:05 AM9:30 AMLiver CancerJanice Jou, MD MHS9:35 AM10:00 AMPancreas‐Biliary TreeJessica Yu, MD10:00 AM10:30 AM‐Break‐10:30 AM10:55 AMPortal HypertensionScott Naugler, MD11:00 AM11:25 AMMotility and Functional Bowel DiseaseSarah Diamond, MD11:30 AM11:55 AMColon CancerDavid Lieberman, MD11:55 AM12:15 PM‐Lunch Break‐12:15 PM12:40 PMInflammatory Bowel DiseaseAnthony Sofia, MD12:45 PM1:45 PMViral Hepatitis (Keynote Speaker)Norah Terrault, MD, MPH1:45 PM2:00 PMClosing Remarks, SummaryJoseph Ahn, MD, MS,MBA/Anthony Sofia, MD 1 3Speaker
Best of AASLD and DDW 2019ACKNOWLEDGMENTSWe thank the following companies for their support of the Best of AASLD and DDW 2019:Silver Level Supporter: AbbVie HCVBronze Level Supporter: GileadEXHIBITORS AbbVie GI CareAlexionBoston ScientificCapsoCookGilead HepBInterceptJohnson JohnsonMerckPfizerRetrophin Inc.4
Best of AASLD and DDW 2019Speaker BiographiesNorah Terrault, MD, MPH, FAASLD, is the Chiefof Gastroenterology & Hepatology at KeckMedical Center of University of SouthernCalifornia. Dr. Terrault is world renowned for herexpertise on her work related to viral hepatitis,especially in the setting of liver transplantation.After earning her medical degree from theUniversity of Alberta, Dr. Terrault completedmedical training in Internal Medicine andGastroenterology at the University of Toronto,Canada followed by post-doctoral fellowship inhepatology and viral hepatitis at University ofCalifornia, San Francisco along with a concurrentmaster’s degree in public health from Universityof California, Berkeley.Dr. Terrault has authored numerous originalarticles, reviews and book chapters on viralhepatitis, including the most recent AASLDHepatitis B treatment Guidelines. She is aninvestigator on several NIH-funded clinicalstudies in hepatitis B, C and NASH. She has served as deputy editor for LiverTransplantation, associate editor for Hepatology, is current Associate Editor forHepatology Communications and Councilor for the AASLD Governing Board.In addition, Dr. Terrault will serve as the president of the AASLD in 2023 and hasbeen the recipient of many prestigious awards in the field of hepatology.5
Best of AASLD and DDW 2019 Speaker BiographiesJoseph Ahn, MD, MS, MBA is Professor of Medicine, Section Chief and Director ofClinical Hepatology at OHSU. Dr. Ahn received his medical degree fromNorthwestern University and completed his internal medicine residency at theUniversity of Chicago and gastroenterology fellowship at Northwestern. Dr. Ahntreats patients with chronic liver diseases, and liver transplant candidates andrecipients. His research interests are focused on hepatitis B, hepatitis C, and PSC.Michael Chang, MD, MS, MBA completed medical school, internal medicineresidency, gastroenterology fellowship, and a Master of Science at BostonUniversity, followed by training in Transplant Hepatology at Harvard’s Beth IsraelDeaconess Medical Center, and an MBA at Oregon Health and Science University /Portland State University. He is the Section Chief for gastroenterology andhepatology at the VA Portland Health Care System, Associate Professor ofMedicine at OHSU and the Program Director for the Transplant HepatologyFellowship program. Dr. Chang's areas of clinical interest include qualityinitiatives in Advanced Liver Disease, non-invasive assessment of liver fibrosis,and the use of ECHO to improve specialty care access. Dr Chang is a coinvestigator on an NIH funded study looking at symptom burden in patientcaregiver dyads with end stage liver disease to better understand the trajectory ofsymptoms and how best to support this challenging population.Sarah Diamond, MD is an Assistant Professor of Medicine. Dr. Diamond attendedThe University of Miami, Miller School of Medicine in Miami, FL and thencompleted her internal medicine residency, chief residency and gastroenterologyfellowship at Oregon Health and Science University. She joined the OHSU GIfaculty in 2015. She is the medical director of the Digestive Health Center and theassociate fellowship director for the GI program. Her clinical interests includenutrition and gastrointestinal motility.6
Best of AASLD and DDW 2019 Speaker BiographiesJanice Jou, MD, MHS is an Associate Professor in the Division of Gastroenterologyand Hepatology at OHSU, and is primarily based in the VA Portland Health CareSystem. Dr. Jou is the program director for the OHSU Gastroenterology fellowship.She completed medical school at Northwestern University, internal medicineresidency and chief residency at the University of Wisconsin, andgastroenterology and transplant hepatology fellowships at Duke University. Herclinical and research interest is in hepatocellular carcinoma. She is also an activemember on education and training committees of the American Association forthe Study of Liver Diseases and American Gastroenterological Association.Dekey Lhewa, MD earned her medical degree from the University of WashingtonSchool of Medicine where she also completed her internal medicine residency.This was followed by a fellowship in gastroenterology and hepatology at theUniversity of California San Francisco-Fresno program and a transplanthepatology fellowship at the University of Michigan.She has special interests in the management of liver tumors along with issuesregarding access to care and outcomes of chronic liver disease and livertransplantation especially among underserved populations.She has spent majority of her life in the Pacific Northwest and is very happy to beback home.David Lieberman MD, is a Professor of Medicine and Chief of the Division ofGastroenterology and Hepatology at OHSU and the Portland VA Medical Center.Dr. Lieberman is internationally recognized as an expert on colon cancerscreening with landmark publications in the New England Journal of Medicine,Gastroenterology and Annals of Internal Medicine. He is Chairman for the VACooperative Study # 380, which utilized colonoscopy to screen asymptomaticsubjects for colorectal cancer. Dr. Lieberman was the Chairman of the MultiSociety Task Force on Colorectal Cancer (2006-2012), and authored colon cancerscreening recommendations in 2008 and the polyp surveillance guideline in 2012as well as colonoscopy quality indicators in 2007. He is the Director of the ClinicalOutcomes Research Initiative (CORI), supported by NIH since 1999. The projecthas created a national endoscopic data repository for research, with more than 90peer-reviewed publications to date, including papers in JAMA, Gastroenterologyand Gastrointestinal Endoscopy. From 2006 to 2008, Dr. Lieberman served as amember of the National Commission on Digestive Diseases. Dr. Lieberman wasPresident of the American Society for Gastrointestinal Endoscopy (ASGE) in 20012002. He was the Associate Editor of Gastroenterology (2011-2013). He was theClinical Research Councilor on the board of the American GastroenterologicalAssociation (2012-2015), and is the current President of the AGA.7
Best of AASLD and DDW 2019 Speaker BiographiesArnab Mitra, MD is an Assistant Professor at OHSU who specializes in caring forpatients with liver disease, including those who have undergone liver transplant.He received his medical degree from the University of Alabama, internal medicineresidency at the University of Wisconsin, and gastroenterology and transplanthepatology fellowships at Oregon Health and Science University. He joined theOHSU Hepatology faculty in 2019.Scott Naugler, MD is one of the transplant hepatologists at OHSU. He serves at theMedical Director for Liver Transplant as well as the Multi-Disciplinary LiverTumor group, with clinical interests in Hepatocellular Carcinoma and livertransplantation. He also works in the lab on liver regeneration and HCC. Scottgraduated from Rhodes College in Memphis, TN with a B.A. in Creative Writing. Hethen attended medical school in Little Rock, AR, followed by internal medicineresidency first at Washington University then OHSU (including a chief residency),after which he completed a Gastroenterology fellowship at UC San Diego. Hejoined the OHSU faculty as a Transplant Hepatologist in 2007.Anthony Sofia, MD is a gastroenterologist that specializes in the care of patientswith inflammatory bowel disease. Anthony earned his degree in medicine fromthe University of Chicago Pritzker School of Medicine. After medical school, hecontinued at the University of Chicago Medicine for internal medicine residencyand gastroenterology fellowship. His research focuses on ways to deliver optimalclinical care for people with inflammatory bowel disease, including clinical trialsof emerging therapies and the use of intestinal ultrasound for bedside diseaseactivity assessments. He joined the faculty at OHSU in 2018.Jessica Yu, MD focuses on patients with diseases of the bile duct and pancreas,gastrointestinal cancer and pre-cancerous conditions. She performs proceduresincluding ERCP, EUS, small bowel enteroscopy, endoscopic mucosal resection, andenteral stenting. She has a special interest in bariatric endoscopy and endoscopicsuturing. Her research focuses on understanding and improving the outcomes ofendoscopy.8
Best of AASLD and DDW 2019Saturday, December 14, 2019FACULTY DISCLOSURE INFORMATIONIn accordance with the requirements of the Standards for Commercial Support of the Accreditation Council for ContinuingMedical Education, each instructor and member of the planning committee has been asked to disclose any relevant financialrelationships with commercial interests (defined as: any entity producing, marketing, re‐selling, or distributing health care goodsor services consumed by, or used on, patients). The information disclosed for this activity is listed below.In addition, the planners and instructors listed have agreed that all recommendations involving clinical medicine will be basedon evidence that is generally accepted within the profession as adequate justification for their indications and contraindicationsin the care of patients; that all scientific research used in support or justification of a patient care recommendation will conformto the generally accepted standards of experimental design, data collection and analysis; and that material to be presented willbe made available for advance peer review if requested.INSTRUCTORS/MODERATORSJoseph Ahn, MD, MS, MBAConsultant to Gilead, for which he receivesconsulting fees.Nothing to discloseJanice Jou, MD, MHSDekey Lhewa, MDSarah Diamond, MDDavid Lieberman, MDNothing to discloseNothing to discloseConsultant, Scientific Advisory Boards forCEGX, Freenome, Check-Cap, Ironwood,for which he receives consulting fees.Nothing to discloseNothing to discloseNothing to discloseNothing to discloseNothing to discloseNothing to discloseMark Anthony Sofia, MDArnab Mitra, MDJessica Yu, MDMichael Chang, MD, MScWillscott Naugler, MDNorah Terrault, MD, MPHPROGRAM PLANNING COMMITTEEJanice Jou, MD, MHSDekey Lhewa, MDMark Anthony Sofia, MDRebecca Matro, MDNothing to discloseNothing to discloseNothing to discloseAdvisory board for Pfizer for which shereceives an honorarium.9
No DisclosuresBest of AASLDLiver TransplantMichael F. Chang, MD, MSc, MBASection Chief GI & HepatologyAssociate Professor of MedicineVA Portland Healthcare SystemOutlineHCV AND TRANSPLANT HCV and Transplant HCC and Transplant High risk transplant Changing landscape of liver transplant and liver cancer Current state of transplant re‐districting Abstract 3: Multicenter Experience Evaluating Outcomes of HCVSeropositive Donors to HCV Seronegative Recipients LiverTransplantation Abstract 38: Transplantation from HCV Infected Donors to HCV‐Uninfected Recipients: Short Course Therapy to Prevent Transmission Abstract 117: Transplantation of Hepatitis C Positive Kidneys Into HCVNaïve Patients Reveals Early Development of a Robust Viral Burden:Implications for the Initiation of TherapyHCC AND TRANSPLANTHigh Risk Transplant Abstract 15: US Multicenter Analysis of 2529 HCC PatientsUndergoing Liver Transplant: 10 year Outcome Assessing the Role ofDownstaging to Within Milan Criteria Abstract 225: Six‐month Waiting Rule Lowered WaitlistMortality/Dropout and Decreased Regional Disparity in LiverTransplant Candidates with HCC Abstract 226: Acceptable Liver Transplantation Outcomes AmongOlder Recipients with HCC Despite Higher Risk Features on Explant ina Large Multicenter US Cohort Abstract 91: Abstract 92: Simultaneous Liver Kidney Transplant in the Elderly: Is Therean Appropriate Age Cut Off? Abstract 94: Liver transplant recipients with BMI 40‐50 have excellentpatient and graft survival Abstract 1142: Outcomes of Liver Transplantation in Patients with Pre‐existing Coronary Artery Disease Abstract 1148: Presence of Any Degree of Coronary Artery Disease AmongLiver Transplant Candidates is Associated with Decreased TransplantEligibility and Increased Rate of Post‐Transplant Major Cardiac AdverseEvent10
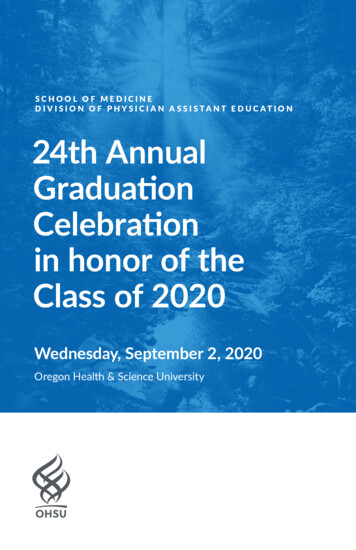
Liver allocation for HCCCHANGING LANDSCAPE OF LIVERTRANSPLANT AND LIVER CANCERLiverHospital statusWaitlist timeHCC1996NotmetastaticIn Milan 75% 35%Mazzaferro, NEJM, 1996Liver allocation for HCCLiverHospital statusWaitlist timeLiver allocation for HCCMELDLiverHCCNotmetastatic19962002In MilanT1 24T2 29NotmetastaticT1 1 nodule 2 cmT2 MilanLiver allocation for HCCLiverHospital statusWaitlist timeMELDHCCHospital statusWaitlist time20022003In MilanT1 24T2 29T1 20T2 24T1 1 nodule 2 cmT2 MilanLiver allocation for HCCMELDLiverHCCNotmetastatic1996Hospital statusWaitlist timeMELDHCC1996200220032004In MilanT1 24T2 29T1 20T2 24T1 0T2 24NotmetastaticT1 1 nodule 2 cmT2 Milan19962002200320042005In MilanT1 24T2 29T1 20T2 24T1 0T2 24T1 0T2 22MELD exception points 22Listing253 months286 months31T1 1 nodule 2 cmT2 Milan34379 months 12 months 15 monthsThis is the “MELD elevator”—a stepwise increase in MELD score in a patient witha MELD exception (most common is HCC) that ultimately results in the patientgetting to the top of the list11
Liver allocation for HCCLiverHospital statusWaitlist timeLiver allocation for 420052015In MilanT1 24T2 29T1 20T2 24T1 0T2 24T1 0T2 22T1 0T2 28*MELD exception points BioBio283 monthsListing6 months31Notmetastatic349 months 12 months 15 months20022003200420052015In MilanT1 24T2 29T1 20T2 24T1 0T2 24T1 0T2 22T1 0T1 0T2 28* T2 28*Down‐stagingAFP 1000ListingBio3 months286 months31342017349 months 12 months 15 monthsMELD elevator in effect (after 6 month wait)Liver allocation for HCCHospital statusWaitlist time1996MELD exception points Bio34MELD elevator in effect (after 6 month wait)LiverHospital statusWaitlist timeOHSU “A” LT waitlist, Nov 3, 17In MilanT1 24T2 29T1 20T2 24T1 0T2 24T1 0T2 22T1 0T2 28*T1 0T1 0T2 28*T2 MMAT‐Down‐staging3AFP 1000MMAT ‐3MMAT ‐3MELD exception points BioListingBio3 monthsMMAT ‐36 months2019MMAT ‐39 months 12 months 15 monthsMELD elevator is goneMMAT Median MELD at Transplant ( 32 in Portland now, thus MMAT ‐3 29OHSU “A” LT waitlist, Nov 3, 2019HCC patients with MMAT‐3MELD exceptionsOHSU “A” LT waitlist, Nov 3, 2019{HCC patients with MMAT‐3MELD exceptionsThis is where a new patient withHCC (who has already waited 6months) would be placed12{
Current national down‐staging policyUPDATE ON DOWNSTAGING One tumor 8 cm Two or three tumors, all 5 cm, total 8 cm Four or five tumors, all 3.0 cm, total 8 cmCurrent national down‐staging policyCurrent national down‐staging policy One tumor 8 cm Two or three tumors, all 5 cm, total 8 cm Four or five tumors, all 3.0 cm, total 8 cmTimeline for down‐stagingPatient presents Out of Milan Inside down‐stagingAfter locoregional treatment, tumor burden is withinMilan (“down‐staged”)**Based on hypervascular/washout tumor sizeLoco‐regionaltreatmentCurrent national down‐staging policyCurrent national down‐staging policyTimeline for down‐stagingTimeline for down‐stagingPatient presents Out of Milan Inside down‐stagingPatient presents Out of Milan Inside down‐staging1 month1 monthLoco‐Insideregional MilantreatmentLoco‐Insideregional Milantreatment13“ASAP”List forLT
Current national down‐staging policyCurrent national HCC policy Milan criteria as noted Down‐staging into Milan as noted AFP must be 1000 ng/mL*Timeline for down‐stagingPatient presents Out of Milan Inside down‐staging1 month“ASAP”3 months3 monthsMMAT ‐3 until transplanted**In CTP A patients who are within Milan, if the AFP is 1000 ng/mL, and locoregional treatment brings it to 500 ng/mL, the standard exception can be grantedLoco‐Insideregional MilantreatmentList forLTScanScan*Must stay within Milan entire timeCaveats to HCC policyCaveats to HCC policyIf HCC present (in or out of Milan) and last locoregionaltreatment was 2 years prior, the lesions areconsidered dead and will not count toward a MELDexception.HCC tumors for purposes of LT policy are notcumulative.Patient 1: outside down‐staging, can never be transplantedBut if new HCC (within Milan, etc) appears, anexception based on the new tumors is acceptable.4 cm HCC5 cm HCCRealities of HCC at MMAT ‐3Caveats to HCC policyIntendedHCC tumors for purposes of LT policy are notcumulative.1. More sick cirrhotics will be transplanted, and atlower MELD scoresPatient 1: outside down‐staging, can never be transplanted4 cm HCC5 cm HCCPatient 2: always within Milan, can get standard exception4 cm HCC Y90 4 cm HCC non‐viableNew 5 cm tumor14
Realities of HCC at MMAT ‐3HCC LandscapeIntendedRealities1. More sick cirrhotics will be transplanted, and at lowerMELD scoresThe necessary corollary1. Increasing incidence of HCC2. More patients eligible for transplant listing3. Fewer patients getting transplant for HCC1. Fewer HCC patients will get transplanted––There is a “log‐jam” of patients listed at MMAT ‐3Those at MMAT ‐3 are ordered by time on list with anexception (not by HCC burden, etc.)ManifestationsMore and more HCC management withouttransplantNeed to move away from “bridging”From:“Bridging” to anuncertain transplantPractical differences in approach?To:Chronic disease that mustbe managed indefinitelyVery little but1. Transplant will no longer be a near‐guarantee forpatients, and should be communicated as such evento patients within transplantable criteriaTACEResection2. We may want to consider treating patients with T1disease (HCC 2 cm) immediately Rather than observe them until they grow into T2(transplantable) criteriaSystemictherapyRFATransplant in selectfewAASLD Guidelines HCC managementCURRENT STATE OF TRANSPLANTREDISTRICTING6. Should adults with cirrhosis & T1 HCC on thetransplant list get treatment or be observed?Recommendation: Observe with imaging inhopes/anticipation of HCC growth to T2, thus qualifyingfor priority on the list. Quality of evidence: very low Strength of recommendation: conditionalHeimbach, Hepatology, 201715
Geographic disparities in allocationBurden of liver disease vs those on transplant listsGeographic disparities in allocation% deaths from liverdisease captured withwaitlist deaths, 2012 11.5%6.2‐9.9%3‐5.9% 2.7%Goldberg, Liv Transplant, 2016Geographic disparities in allocationGeographic disparities in allocation More doctors More centers Better accessMore listedpatients/donor higher MELD attransplantGeographic disparities in allocationGeographic disparities in allocationMove donor livers More doctors More centers Better accessMore listedpatients/donor higher MELD attransplant16Not listed Not advantaged
Geographic disparities in allocationGeographic disparities in allocationMELD at transplant may not reflect all disparities1. MELD exceptions vary widely among regions Move donor livers? Not listed Not advantagedDeceased donor liver allocationintroducedDemand exceedssupplyNIH: LT acceptableas rx for ESLDFinal RuleChild’s scoreaddedMELDShare g proposal went for regional vote fall 2016CyclosporinIncreases local MELD on waitlist3. Center competition affects listing practices More doctors More centers Better accessAffects overall allocation MELD2. Regions with better health care access list a higher percentage ofthe lNat’l Organ Transplant ActOrgan Procurement &Transplant Network created17Increases local MELD on waitlist
Disclosure I have no financial relationships to disclose2019 BEST OF AASLD AND DDWCONFERENCENon-viral liver diseaseArnab Mitra, MDAssistant Professor of MedicineOHSU Department of GI/HepatologyLearning Objectives Updates in: NAFL and NASHNON-ALCOHOLICFATTY LIVER DISEASE Cholestatic and Autoimmune liver diseaseWorldwide estimated prevalence of NAFLD and distribution of PNPLA3 genotypesNon-Alcoholic Fatty Liver Disease Evidence of hepatic steatosiswithout secondary causes offat accumulation Spectrum of diseaseNormal20-40% of general population Risk Factors Central obesity Hypertension Dyslipidemia Type 2 Diabetes Metabolic syndrome Advancing ageSteatosis15-25%NASH10-29% in 10 yearsCirrhosis HCCYounossi, Z. et al. (2017) Global burden of NAFLD and NASH: trends, predictions, risk factors and preventionNat. Rev. Gastroenterol. Hepatol. doi:10.1038/nrgastro.2017.10918
PathogenesisMortality Cardiovascular disease is the most common cause ofdeath Cancer-related mortality is among top 3 causes of deathin patients with NAFLD NAFLD is 3rd most common cause of HCC Histological feature associated with long-term mortality isfibrosis (particularly zone 3 sinusoidal fibrosis)Non-Invasive Tests for Fibrosis NAFLD Fibrosis Score FIB-4 ELF (available in Europe) Elastography MR VCTEManagement Lifestyle Interventions 5% body weight loss had improved hepatic steatosis 7% body weight loss associated with improvement in NAFLD activityscore, with 7-10% body weight loss being associated with higherlikelihood of reversing histopathologic features/fibrosis of NASH Medications Pioglitazone Improves liver histology with biopsy-proven NASH with or without DM Vitamin E Improvement in aminotransferases and steatosis, inflammation, andballooning have previously been seen Consideration for use in biopsy-proven NASH in those who are nondiabetic or non-cirrhotic Bariatric Surgery Improvement in fibrosis and NAS, resolution of NASH in some cases Increased mortality in those with cirrhosis, particularly decompensated19
THE BEST OF THE LIVER MEETING 2019 NAFLD/NASH 13 2019 American Association for the Study of Liver Diseases. Not for Commercial UseTreatments on the Horizon Obeticholic Acid FXR agonist approved for PBC Awaiting FDA approval for NASH Phase 3 REGENERATE study – 25 mg daily demonstratedimprovement in liver fibrosis ( or 1 stage) without worsening NASH(achieved primary endpoint) Saroglitazar PPAR alpha/gamma agonist Tropifexor FXR agonistAssessment of disease severity ALT is not a reliable indicator of disease severity 2018 AASLD Guidelines Metabolic syndrome predicts the presence of steatohepatitis NFS or FIB-4 index can be used to identifying NAFLD patients withhigher likelihood of having bridging fibrosis (stage 3) or cirrhosis(stage 4) VCTE or MRE are clinically useful tools for identifying advancedfibrosis in patients with NAFLD20
Primary Biliary Cholangitis (PBC) Female MaleCHOLESTATIC ANDAUTOIMMUNE LIVERDISEASE Prevalence: Diagnosis: Elevated alkaline phos AMA (seen in 95% ofpts) Biopsy PBC Treatment Ursodiol 1st line Obeticholic acid 2nd line(approved in 2016)Clin Gastro Hepatology 2018Emerging PBC Therapies: Fibrates 1 RCT Benzafibrate In addition to urso ininadequate urso responsepatients Adverse events: Hepatoxicity CPK elevation Advance disease?Corpicot C et al, NEJM 2018Fibrates Only approved by FDA as lipid-lowering medications Activate PPAR-alpha, gamma and delta PPAR-alpha – regulates bile acid synthesis and detoxification PPAR-delta and PPAR-gamma – anti-inflammatory and anti-fibroticproperties21
Safety and efficacy of seladelpar in PBC related cirrhosis: 52-weekanalysis from a randomized phase 2 study: Abstract LB-3 Aim To assess safety and efficacy ofdaily seladelpar Method Randomized open-label, doseranging, phase 2 study Patients with inadequateresponse or intolerance to urso Conclusion Good anti-cholestatic efficacy Results--52 weeksSeladelpar5/10 mg10 mgResponders59%71%AP MeanChange-47%-46%APNormalization24%29% Well tolerated Phase 3 studyBowlus C, et al, Abstract LB-3Update:Seladelpar moved to phase3 study given positivesafety resultsPrimary Sclerosing Cholangitis Male Female 2/3rds: concurrent IBDWeismuller, T et al. Gastro 201722
Conflict of Interest DisclosuresBest of AASLD 2019:Update in HCC I have nothing to disclose.Janice Jou, MD MHSAssociate ProfessorDivision of Gastroenterology and HepatologyOregon Health and Science UniversityPortland VA Medical CenterImpact of Healthy Lifestyle on HCC andcirrhosis riskPrevention of HCC Nationwide prospective cohort adult men and women without known liverdisease at baseline, 1986‐2012 N 121,893 121 HCCs Low risk lifestyle met all criteria Never smoker (pack years 5)No/moderate EtOH ( 1 drink day women, 2drinks/day men)BMI 18.5‐24.9Weekly physical activity 6 MET hoursHealthy diet (upper 40% of the Alternative Healthy Eating Index)HR 3.59 (95% CI 1.50‐7.42) for HCCHR 4.27 (95%CI 2.06‐11.69)Single modifiable risk factor with largest Population attributablerisk was overweight/obesity BMI 25, PAT 36% (95%CI 22‐50), 42%(95% CI 19‐54)Simon TG et al. AASLD Abstract #16 High risk lifestyle‐ all other patientsSimon TG et al. AASLD Abstract #1623
AASLD Guidelines for HCC Surveillance Ultrasound with or without AFP, every 6 months Do not perform surveillance in Child’s class C cirrhosis unlessthey are on the transplant waiting list, given the low anticipatedsurvival for patients with Child’s C cirrhosis Comorbidities precluding diagnosis, surveillance, or treatment (renalfailure) Randomized controlled trials supporting surveillance/screeningfor HCC are sparseHeimbach J et al. AASLD Guidelines for HCC 2017AASLD guidelines regarding HCV after DAAtherapyAASLD Guidelines for HCC Surveillance Multiphase CT and MRI are generally equivalent Choose test based on center expertise Breath holding, patient movement, ascites make MRI more variable Discourage biopsy of every indeterminate lesion Patients with Child’s A cirrhosis with T1 or T2 HCC should undergoresection over ablation (Quality: Mod, Strength: conditional) In the absence of portal hypertensionHeimbach J et al. AASLD Guidelines for HCC 2017LI‐RADS: Liver Imaging Reporting andData System‐ 2018GALAD for early detection of HCC24
HCC AASLD Guidance: Diagnostic algorithmUltrasound /‐ AFP every 6 monthsIf a lesion is 1cm or new AFP 20: Multiphase CT or MRIf benign, LiRADS 1‐2:Resume U/S every 6monthsIf indeterminate, LiRADS 3:repeat CT/MR in 3‐6 monthsIf probable HCC, LiRADS 4:Multidisciplinary discussionto consider biopsy or CT/MRin 3 monthsIf diagnostic of HCC,LiRADS 5:Multidisciplinarydiscussion of possibletreatment optionsAdapted from Dr. Julie Heimbach, AASLD 2019, HCC Guidance SummaryBCLC Staging:and MORE!Bolondi L et al. Semin Liver Dis 2012TARE Conventional Y‐90 Lobar Radiation segmentectomy Superselective delivery of an ablative dose of radiation ( 190 Gy) tosegmental artery feeding the tumor Assumes that there is an equal distribution of the Y‐90 dose to the entirevolume of liver perfused, and perhaps higher concentration to ahypervascular tumor like HCChttps://evtoday.com/articles/2018‐oct/Marrero JA et al. AALSD Practice Guideline HCC 201825
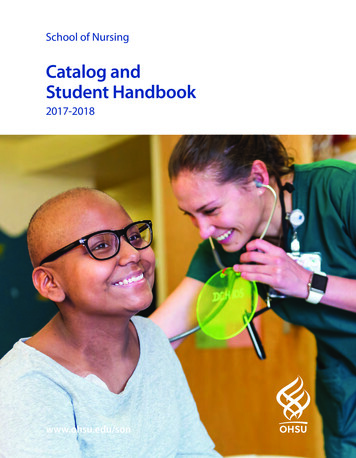
TARE vs TACE: Meta‐analysis 18 studies included 1 RCT 4 prospective cohort studies N 2561 patients Child’s A 63.6%, B 33.1%, C 2.1% BCLC A 26.1%, BCLC B 43.8%,BCLC C 30.2%Brown A et al. AASLD 2019 Abstract #369Sangro B et al. J Hepatol, 2012Sangro B et al. J Hepatol, 2012Systemic Treatment forAdvanced HCCTARE vs TACE: Meta‐analysis Significant heterogeneity Time to progression was 17.5 months (TARE) vs. 9.8 months (TACE) TARE with a longer TTP than TACE, but no significant difference inoverall survivalCheckMate 459: Nivolumab First lineLenvatinib‐induced thyroiditis N 60 Subclinical hypothyroidism n 7(11.7%) Overt hypothyroidism n 26 (43.3%) Thyrotoxicosis n 5 (8.3%) Of those with hypothyroidism,N 27, 84% developed symptomswithin 2 weeks Patient with hypothyroidism hadbetter prognosis Mechanism is unknown: VEGFinhibition leading to decreasedthyroid blood flow? Multinational studyNivolumab 240mg IV q2weeksSorafenib 400mg po BIDPrimary endpoint: overall survivalN 743 randomized 1:1Minimum F/U 22.8 monthsDid not meet primary endpointLess side effects Grade 3/4 22% vs49% Discontinuation 4% vs 8%Yau T et al. ESMO 2019 Annals of Oncology (2019) 30(suppl 5): v851‐v934. 10.1093/annonc/mdz394Koizume Y et al. AASLD 2019 Abstract #34626
IMbrave 150: Atezolizumab/Bevicizumab vs.SorafenibAtezolizumab PD1 Inhibitor Used previously Iung andbladder, breast CA 1st line treatment for HCC 2:1 randomization 336 patients treated with atezolizumab 1200 mg IV plus bevicizumabat 15 mg/k
California, San Francisco along with a concurrent master's degree in public health from University of California, Berkeley. Dr. Terrault has authored numerous original articles, reviews and book chapters on viral hepatitis, including the most recent AASLD Hepatitis B treatment Guidelines. She is an investigator on several NIH-funded clinical