Transcription
Nursing Executive CenterAchieving Care ContinuityBest Practices for Building a System That Never Discharges the Patient 2015 The Advisory Board Company advisory.com
Nursing Executive CenterLEGAL CAVEATThe Advisory Board Company has made efforts toverify the accuracy of the information it provides tomembers. This report relies on data obtained frommany sources, however, and The Advisory BoardCompany cannot guarantee the accuracy of theinformation provided or any analysis basedthereon. In addition, The Advisory Board Companyis not in the business of giving legal, medical,accounting, or other professional advice, and itsreports should not be construed as professionaladvice. In particular, members should not rely onany legal commentary in this report as a basis foraction, or assume that any tactics described hereinwould be permitted by applicable law orappropriate for a given member’s situation.Members are advised to consult with appropriateprofessionals concerning legal, medical, tax, oraccounting issues, before implementing any ofthese tactics. Neither The Advisory BoardCompany nor its officers, directors, trustees,employees and agents shall be liable for anyclaims, liabilities, or expenses relating to (a) anyerrors or omissions in this report, whether causedby The Advisory Board Company or any of itsemployees or agents, or sources or other thirdparties, (b) any recommendation or graded rankingby The Advisory Board Company, or (c) failure ofmember and its employees and agents to abide bythe terms set forth herein.Project DirectorMarie Katz, MPHContributing ConsultantsNeil KondamuriJenna KoppelMicha’le Simmons, MHADesign ConsultantHaley ChapmanThe Advisory Board is a registered trademark ofThe Advisory Board Company in the United Statesand other countries. Members are not permitted touse this trademark, or any other Advisory Boardtrademark, product name, service name, tradename, and logo, without the prior written consentof The Advisory Board Company. All othertrademarks, product names, service names, tradenames, and logos used within these pages are theproperty of their respective holders. Use of othercompany trademarks, product names, servicenames, trade names and logos or images of thesame does not necessarily constitute (a) anendorsement by such company of The AdvisoryBoard Company and its products and services, or(b) an endorsement of the company or its productsor services by The Advisory Board Company. TheAdvisory Board Company is not affiliated with anysuch company.Practice ManagerKatherine Virkstis, NDManaging DirectorJennifer StewartExecutive DirectorSteven Berkow, JDIMPORTANT: Please read the following.The Advisory Board Company has prepared thisreport for the exclusive use of its members. Eachmember acknowledges and agrees that this reportand the information contained herein (collectively,the “Report”) are confidential and proprietary toThe Advisory Board Company. By acceptingdelivery of this Report, each member agrees toabide by the terms as stated herein, including thefollowing:1. The Advisory Board Company owns all right,title and interest in and to this Report. Exceptas stated herein, no right, license, permissionor interest of any kind in this Report is intendedto be given, transferred to or acquired by amember. Each member is authorized to usethis Report only to the extent expresslyauthorized herein.2. Each member shall not sell, license, orrepublish this Report. Each member shall notdisseminate or permit the use of, and shalltake reasonable precautions to prevent suchdissemination or use of, this Report by (a) anyof its employees and agents (except as statedbelow), or (b) any third party.3. Each member may make this Report availablesolely to those of its employees and agentswho (a) are registered for the workshop ormembership program of which this Report is apart, (b) require access to this Report in orderto learn from the information described herein,and (c) agree not to disclose this Report toother employees or agents or any third party.Each member shall use, and shall ensure thatits employees and agents use, this Report forits internal use only. Each member may make alimited number of copies, solely as adequate foruse by its employees and agents inaccordance with the terms herein.4. Each member shall not remove from thisReport any confidential markings, copyrightnotices, and other similar indicia herein.5. Each member is responsible for any breach ofits obligations as stated herein by any of itsemployees or agents.6. If a member is unwilling to abide by any of theforegoing obligations, then such member shallpromptly return this Report and all copiesthereof to The Advisory Board Company. 2015 The Advisory Board Company 303582advisory.com
Table of ContentsExecutive Summary . . . . . 6Nursing Executive Center Essay: Why We Need to Stop Thinking About “Care Transitions” . . . 7Imperative #1: Equip Clinicians to Provide Continuous Care 23Ensure Easy Access to “Need-to-Know” InformationPractice #1: The Critical Patient Information Summary . 25Practice #2: Motivational Interviewing . 30Practice #3: Patient Preference Discussion Guide . 35Connect the Care Plan Across SettingsPractice #4: Shared Cross-Setting APN . 40Practice #5: Cross-Continuum Care Agreement . 45Practice #6: Cross-Continuum Care Pathway . 49Imperative #2: Promote Clinician Ownership for Cross-Continuum Care . 55Broaden the Front Line’s Perspective Beyond Their Own SettingPractice #7: Cross-Continuum Shared Governance 58Practice #8: Alternative Care Setting Experience 64Practice #9: Community-Focused Nursing School Rotations 71Incentivize Continuous CarePractice #10: Continuum-Focused Leader Incentive Plan . . 76Practice #11: Frontline Organizational Alignment Bonus . . 80Imperative #3: Instill Patient and Family Ownership for Self-Care . 87Appeal to Patients’ Personal Motivators for InvolvementPractice #12: Personally Motivating Goal Incorporation 89Practice #13: Nonclinical Peer Advisor .92Equip Patients and Families with Tools for Self-ManagementPractice #14: Inpatient-Based Key Caregiver Skill Building .101Practice #15: Recorded Transition Instructions .106Practice #16: Personalized Patient Support Line 109Practice #17: Daily Text Reminders .113Imperative #4: Scale Up Support for Vulnerable Patients .119Invest in Targeted Services for Select PopulationsPractice #18: NP-Led Clinic for the Medically Complex . 121Practice #19: Justice Department Partnership for Behavioral Health .126Practice #20: ED Alternatives for Homeless Patients 131Practice #21: Remote Telemonitoring for the Frail Elderly . 137 2015 The Advisory Board Company 303583advisory.com
Available Within Your Nursing Executive Center MembershipIn recent years, the Nursing Executive Center has developed many resources to assist nurse leaders in coordinatingcare across the continuum. Select resources are shown here. All resources are available in unlimited quantitiesthrough the Nursing Executive Center.Coordinating Care Across the ContinuumNurse-Led Strategies for PreventingAvoidable ReadmissionsThe IntegratedNursing EnterpriseBest Practices for Coordinating Care forComplex Patients Across the ContinuumLessons from LeadingCross-Continuum Organizations Building a Readmission Prevention Strategy Guiding Patients to the Appropriate Care Setting Ensuring Patients Are Discharged to theAppropriate Care Setting Ensuring Interdisciplinary Collaboration AcrossCare Settings Facilitating Seamless Transfer to thePost-Acute Care Setting Instilling a System-Level Perspective AmongFrontline NursesPreventing AvoidableHospital AdmissionsNursing’s Role in SafeguardingAcute Care MarginsStrategic Considerationsfor Nurse ExecutivesThirteen Key Objectives andRecommended Initiatives Preventing Unnecessary Readmissions Identifying Patients at Greatest Risk forPreventable Admissions Redistributing Siloed Patient Care Tasksto a Cross-Continuum Navigator Achieving Patient Buy-In toSelf-Management Goals Preempting Unnecessary HospitalUtilization Re-Engaging Patients Missing CareAVAILABLE ONLINETo access these resources or order hard copies of the publications,please visit the Nursing Executive Center’s website: advisory.com/nec. 2015 The Advisory Board Company 303584advisory.com
Advisors to Our WorkThe Nursing Executive Center is grateful to the individuals and organizations that shared their insights,analysis, and time with us. We would especially like to recognize the following individuals for being particularlygenerous with their time and expertise.With Sincere AppreciationAurora Health CareMilwaukee, WISharon QuinlanBellin Health Care SystemsGreen Bay, WILois Van AbelCarolinas HealthCare SystemCharlotte, NCBarb DesilvaJoanne Hart-WrightMary Ann WilcoxCincinnati Children’s HospitalMedical CenterCincinnati, OHPamela FioriniCheryl HoyingMichele ScottBarbara TofaniCullman RegionalMedical CenterCullman, ALCheryl BaileyIntermountain HealthcareSalt Lake City, UTKim HenrichsenLinda HofmannMichelle Vandegraaff 2015 The Advisory Board Company 30358Mackenzie HealthRichmond, ONQunyu LiTiziana RiveraThe Center for Health Care ServicesSan Antonio, TXChristi A. GarfieldTrinity Mother Frances Hospitalsand ClinicsTyler, TXRobert RoseScott SmithMayo ClinicRochester, MNLisa CarterDebra CoxPam JohnsonVictor MontoriMethodist Le BonheurHealthcareMemphis, TNSally AldrichKimberly LamarNikki PolismHealth SolutionsLarkspur, CAAndrew DickPremier HealthDayton, OHBarbara JohnsonSylvain TrepanierScripps HealthSan Diego, CAAthena Philis-Tsimikas5University Health SystemSan Antonio, TXNancy RayC. Jean SmithUniversity of Iowa Collegeof NursingIowa City, IAEllen CramValley Health SystemRidgewood, NJMary CostaAnn Marie LeichmanToni ModakYale-New Haven HospitalNew Haven, CTPaula CrombieMichael FerrySue Fitzsimmonsadvisory.com
Executive SummaryThe Mandate to Provide Seamless, Cross-Continuum CareAll too often, patients receive fragmented, episodic care—which leads to suboptimal clinical outcomes,avoidable health care utilization, and unnecessary spending.Fragmented care is costly to both the nation and individual health care providers. Researchers estimateinadequate care coordination leads the US to waste between 25 and 45 billion each year. And individualproviders are increasingly accountable for the total cost of care for their patients. Neither the country, norproviders, can afford to continue to deliver fragmented and episodic care.Building a Health System That “Never Discharges” the PatientTo break down silos and deliver continuous care, health care providers need to fundamentally rethink howpatients transition between settings. Currently, the central element of any transition is a patient being“discharged” from one setting and “admitted” to the next. But by definition, “discharging” a patient impliesclinicians are relieved of the burden of responsibility for a patient’s care.Health systems must broaden their aspiration to include building a health system that “never discharges” thepatient. The goal is for clinicians in any setting to feel responsible for a patient’s care across the full continuum.For example, nurses on an inpatient medical unit feel responsible for the care and outcomes of their patientsboth on the medical unit as well as all other care settings the patients go to across the continuum—includingprimary care clinics, ambulatory clinics, post-acute care facilities, and patients’ homes.Avoiding the Trap of Perfecting One Transition at a TimeWhen it comes to building a health system that “never discharges” the patient, the Nursing Executive Centerrecommends against a one-off approach in which leaders perfect one individual transition before moving to thenext. This effort can be compared to assembling a puzzle—and piecing together each care setting one by one.The challenge with this approach is perfecting each transition is time consuming and resource intensive. Thereare simply too many “puzzle pieces” for it to be feasible. In addition, this approach can lead to a piecemeal endresult, rather than a cohesive system that seamlessly supports patients as they move through the carecontinuum.To build a system that “never discharges” the patient, the Nursing Executive Center strongly recommendsleaders address underlying, systematic issues that affect all patient transitions. The goal is to implementstrategies that improve transitions across multiple care settings at once—rather than working setting by setting.Read the Study in Full to Learn MoreAchieving Care Continuity equips nurse leaders with four imperatives to build a system that “never discharges”the patient. The four imperatives to achieve care continuity are:1. Equip clinicians to provide continuous care.2. Promote clinician ownership for cross-continuum care.3. Promote patient and family ownership for self-care.4. Scale up support for vulnerable patients.Read the complete study for detailed guidance and best practices to act on each imperative. 2015 The Advisory Board Company 303586advisory.com
Nursing Executive Center EssayWhy We Need to Stop ThinkingAbout “Care Transitions” 2015 The Advisory Board Company 303587advisory.com
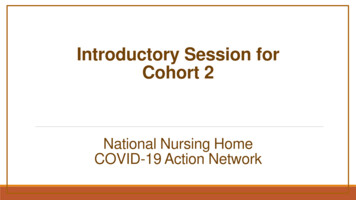
Despite health care leaders’best efforts to improve carecoordination, patients continueto receive fragmented, episodiccare. This manifests as caredelivered in one-off visits in highacuity settings, or as avoidableutilization. According to recentstudies, more than 70% of EDvisits are avoidable, 4.4 millionhospital trips are preventable,and 18% of hospitalized patientsare readmitted within 30 days.Huge Opportunity for ImprovementPercentage of ED Visits ThatAre Avoidable in the US171%4.4MEstimated number ofpreventable trips to UShospitals each year18%30-day all-causereadmission rate2Source: Truven Health Analytics, “Avoidable Emergency Department Usage Analysis,” /EMP 12260 0113 AvoidableERAdmissionsRB WEB 2868.pdf;Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, “Nationwide Frequency andCosts of Potentially Preventable Hospitalizations, 2006,” 2.jsp;CMS's 2012 Inpatient Standard Analytical File (SAF); Nursing Executive Center interviews and analysis.1) Based on Truven Health Analytics analysis of 6,135,002 ED visits in 2010; “Avoidable” includesall ED visits except those for which medical care was required within 12 hours in the ED setting.2) CMS, 2012. 2015 The Advisory Board Company 303588advisory.com
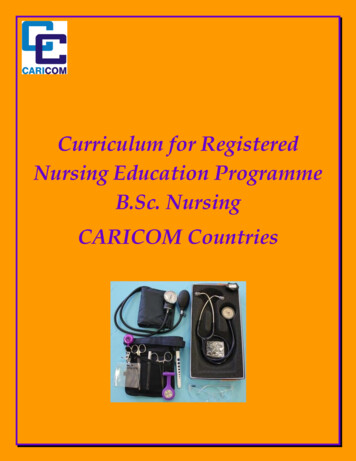
Not only does siloed caredelivery lead to sub-optimaloutcomes, it is also costly.Researchers estimate the USwastes between 25 and 45billion annually from inadequatecare coordination.The benchmarks shown hereprovide a closer look at the costof poorly coordinated care. Theyshow the difference in permember per-month costs forpatients whose care is “looselymanaged” versus “wellmanaged.” According to thisdata, patients with looselymanaged care cost at least 100per month more than those withwell-managed care.Poor Coordination Costing Billions NationallyDifference Between “Loosely Managed”and “Well-Managed” PMPM1 Spending2MedicaidCommercial 100.48LooselyManaged 131.84LooselyManagedWellManagedHealth care providers are keenlyaware of the high cost and suboptimal outcomes that resultfrom siloed care delivery.Accordingly, there is strong workalready underway to improvecare transitions.WellManaged 449.79LooselyManagedWellManaged 25B- 45BEstimated annual amount of wastefulspending resulting from inadequatecoordination31) Per member per month.2) 2011 data from Milliman.3) 2011. 2015 The Advisory Board Company 30358MedicareSource: Milliman; Health Affairs, “Health Policy Brief: Improving Care Transitions,” 2012, ?brief id 76; Nursing Executive Center interviews and analysis.9advisory.com
A common starting point forimproving care transitions ispreventing readmissions. Andnew policies—includingMedicare’s HospitalReadmissions ReductionProgram—have createdfinancial incentives that makereadmissions a logical place forhealth care leaders to start.For organizations tacklingreadmissions, the NursingExecutive Center recommendsreviewing our publication NurseLed Strategies for PreventingAvoidable Readmissions. Asshown here, it offers a strategicframework and best practicesfor improving two specifictransitions in care: the transitionfrom acute care to post-acutecare, and from acute care tohome.A Common Starting Point for Improving TransitionsNurse-Led Strategies for Preventing Avoidable ReadmissionsLeveraging the Inpatient Stay to Equip Patients for Long-Term Self-Management123Scale Interventionsto Level of RiskIdentify and ActivateKey LearnersEquip Patients with Accurateand Easily ActionablePost-Discharge InstructionsFacilitating Seamless Transfer to the Post-Acute Care Setting456Ensure Patients AreDischarged to theAppropriate Care SettingElevate PAC Qualityto Ensure Safe Carefor Complex PatientsEnable a Safe Transition Homewith Immediate Follow-Up Carefor Most Vulnerable PatientsAccess Nurse-LedStrategies for PreventingAvoidable Readmissions onadvisory.com/nec.Source: Nursing Executive Center, Nurse-Led Strategies for Preventing AvoidableReadmissions, 2011; Nursing Executive Center interviews and analysis. 2015 The Advisory Board Company 3035810advisory.com
While preventing readmissionsis a strong starting point forimproving care transitions,providers need to expand theirefforts. This is becauseproviders are increasinglyaccountable for the total cost ofcare for patients.As illustrated here, providersalready assume full risk foruninsured patients, MedicaidManaged Care patients, andhealth system employees. Overtime, many health careproviders will assume full risk foradditional patient populations,such as patients within anAccountable Care Organization(ACO) and commerciallyinsured patients.Being accountable for total costof care means organizationsmust focus on all caretransitions—not just the twotransitions that are part of typicalreadmission efforts—becauseunnecessary health carespending occurs at many pointsalong the care continuum. Whilepreventable readmissions costsMedicare about 12 billionannually, this is only a portion ofthe estimated 25 to 45 billionannual cost of inadequate carecoordination in the US.Providers Increasingly Accountable for Total Cost of CarePopulations for Which Health Care Providers Assume Full RiskCommerciallyInsured PatientsPopulationsat RiskACOPatientsUninsured, MedicaidManaged Care, HealthSystem Employees2015Time 12B 25B- 45BEstimated annual cost ofpreventable 30-day hospitalreadmissions1Estimated annual amount of wastefulspending resulting from inadequatecoordination21) Medicare.2) 2011. 2015 The Advisory Board Company 30358Source: Health Affairs, “Health Policy Brief: Improving Care Transitions,” 2012, ?brief id 76; Nursing Executive Center interviews and analysis.11advisory.com
There is an additional benefit tobetter coordinating care andimproving transitions betweenall settings: it keeps patientswithin your network.This benefits all health careproviders regardless of theirpayment environment. Forproviders in a fee-for-serviceenvironment, higher patientvolumes drive revenue. Forproviders in capitated contracts,keeping patients in networkmeans they can controlspending by providing care inthe lowest-cost, clinicallyappropriate setting within thenetwork.Keeping Patients in Network Through Care CoordinationCoordination Benefits All Organizations, Regardless ofPayment EnvironmentBenefits of Keeping Patients in Network by Reimbursement StructureReimbursementStructureBenefit ofKeepingPatients inNetworkFee forServiceFully CapitatedPaymentsDrive revenuethrough increasedpatient volumesControl spendingthrough high-quality,in-network careSource: Nursing Executive Center interviews and analysis. 2015 The Advisory Board Company 3035812advisory.com
In sum, health care providers’future success will hinge onimproving transitions betweenall care settings. But beforetaking action, it is important toclarify what it means to “improvetransitions.”Currently, the central element ofany transition is a patient being“discharged” from one settingand “admitted” to the next. Butthis concept of “discharging” apatient contributes to siloed caredelivery. By definition,“discharging” a patient impliesclinicians are no longerresponsible for the patient’scare.Clarifying Our AspirationBuilding a System That “Never Discharges” the PatientDefinition of “Discharge” “To relieve of a charge, load, or burden” “To release from an obligation”Merriam-Webster DictionaryIn order to improve caretransitions between all settingsand deliver seamless careacross the continuum, healthsystems must broaden theiraspiration beyond “discharging”patients from one setting to thenext. Instead, health systemleaders must build a healthsystem that “never discharges”the patient. The goal is forclinicians in any setting to feelresponsible for a patient’s careacross the full continuum. Forexample, nurses on an inpatientmedical unit feel responsible forthe care and outcomes of theirpatients both on the medical unitas well as all other care settingsthe patients go to across thecontinuum—including primarycare clinics, ambulatory clinics,post-acute care facilities, andpatients’ homes.Source: Merriam-Webster, e; Nursing Executive Center interviews and analysis. 2015 The Advisory Board Company 3035813advisory.com
When it comes to building ahealth system that “neverdischarges” the patient, theNursing Executive Centerrecommends against a one-offapproach in which leadersperfect one individual transitionbefore moving to the next. Thiseffort can be compared toassembling a puzzle—andpiecing together each caresetting one by one.The challenge with thisapproach is that perfecting eachtransition is time consuming andresource intensive. There aresimply too many “puzzle pieces”for it to be feasible. In addition,this approach can lead to apiecemeal end result, ratherthan a cohesive system thatseamlessly supports patients asthey move through the carecontinuum.To build a system that “neverdischarges” the patient, theNursing Executive Centerstrongly recommends thesecond approach shown on thispage, in which leaders addressunderlying, systematic issuesthat affect all patient transitions.The goal is to implementstrategies that improvetransitions across multiple caresettings at once—rather thanworking setting by setting.Building a System That “Never Discharges” the PatientEvolution of Patient Care PerspectivePerfecting Individual omeHealthAchieving Care ContinuityThe following pages describehow this systems approach hasbeen applied to a select patientpopulation.Source: Nursing Executive Center interviews and analysis. 2015 The Advisory Board Company 3035814advisory.com
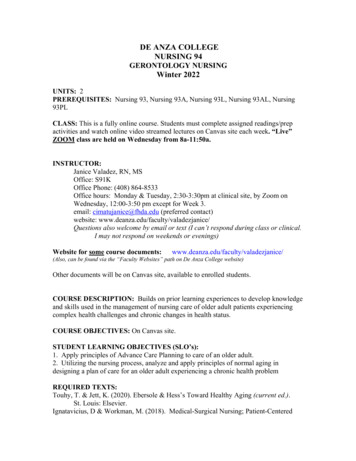
Some progressive organizationshave already begunimplementing a systemsapproach to improving carecontinuity for select patients. Anexample comes from PremierHealth in Dayton, Ohio.Care Navigator Role Gaining MomentumPremier has designed aprogram to improve crosscontinuum care for their 1%most costly patients, regardlessof condition. A key component ofthe program is a navigator1 whoserves as patients’ primary entrypoint to the health system andcollaborates with interprofessional team members toensure all of their patients’health and social needs are met.An excerpt of Premier’s “Top 1%Navigator” job description isshown here.The following pages describekey elements of Premier’s Top1% Navigator Program.A complete version ofPremier’s Top 1%Navigator job descriptioncan be accessed throughan online version of thispublication onadvisory.com/nec.Excerpt of Top 1% Navigator Job Description at Premier HealthPremier HealthJob Description: Advanced Illness Management Navigator, RN or MSWPosition Summary: The Navigator will be an integral member of the Advanced Illnessmultidisciplinary team. Together with nurses, social workers and community healthcoaches, the Navigator will oversee the enrollment of new patients into the project; assesshealth care needs and oversee care plan implementation; help develop care managementstrategies; and work with team members to provide linkages for the various health andsocial needs of patients with cost effective solutions.Nature and Scope: Must have available phone to communicate and transportation, withappropriate licensure and insurance, to visit homes and other sites. Interacts withphysicians, nurses, social workers and other disciplines, administrative personnel, andcommunity resources.Qualifications: Ability to effectively provide clinical care to socially and medicallycomplex patients in a variety of nontraditional settings; ability to work collaboratively ina team and manage multiple priorities, utilize effective time management skills, andexercise sound administrative and clinical judgment; demonstrated ability to work wellwith people of various ages, backgrounds, ethnicities, and life experiences.One navigatoron call to beavailable topatient 24/7by phoneCase in Brief: Premier Health Five-hospital health system headquartered in Dayton, Ohio; includes over100 sites of service In March 2014, piloted community-based navigator program for 25 patientsgenerating greatest number of readmissions and ED visits at one Premierhospital; staffed by one RN and one MSW Navigators serve as single point of contact for all patient medical andcommunity resource needs; coordinate with patient’s primary careclinician, home health Navigators are available to patient 24/7 by phone; conduct communitybased patient visits, call patient on regular basis (frequency based onpatient needs); timeframe of care is 10 months By January 2015, expanded program to include 175 patients acrossmultiple Premier hospitals; new model includes two RNs, two MSWs, oneLPN, one health coach Expanded program serves patients with the greatest number ofadmissions, and patients 64 and older with a large number of admissionsby CMS hospital penalty diagnosis CHF, COPD, and select high-risk patients are monitored by the RNnavigator via remote telemonitoring; monitoring units include ancillary toolsfor weight, pulse oximetry, blood pressure; parameter triggers directly alertnavigator of any abnormality, navigator then contacts patient 180 days post-implementation of Top 1% Navigator pilot, reducedreadmission rate of patient group by 52%, reduced monthly costs forpatient group by 50%1) A navigator team of an RN and an MSW share a panel of 50 patients. 2015 The Advisory Board Company 30358Collaborateswith RN orMSW to servemedicaland nonmedical needsSource: Premier Health, Dayton, OH; Nursing Executive Center interviews and analysis.15advisory.com
First, Premier selects patientsfor the program by analyzing EDencounters and admissions.Second, a navigator team of anRN and an MSW share a panelof 50 patients. Third, one of thetwo navigators is on call 24hours per day, seven days perweek. This enables the team tocollectively serve as the singlepoint of contact for the patient.Fourth, navigators coordinatewith a multidisciplinary careteam to meet patients’ medicaland psychosocial needs. Fifth,navigators use remotetelemonitoring for select1patients. Sixth, navigators adjustthe intensity of their support toeach patient’s risk level.Additional details on how this isdone are on the following page.Establishing a First Line of Defense for the Top 1%Key Elements of Premier’s Top 1% Navigator ProgramPatients selected forprogram based onnumber of EDencounters andadmissionsRN and MSWnavigator teamshares panel of50 patientsNavigators available24/7; serve as primarypoint of contactfor patientNavigators coordinatemultidisciplinary careteam to meet medicaland psychosocial needsNavigators trackpatient health viaremote telemonitoring1(including patients withCHF and COPD)Navigators interactwith patient minimumof twice per month;can be as often as 21times per month1) Remote telemonitoring used primarily for CHF, COPD, and other selected high-risk (high-touch) group patients as deemed appropriate. 2015 The Advisory Board Company 3035816Source: Premier Health, Dayton, OH; Nursing Executive Center interviews and analysis.advisory.com
Even within the top 1% of mostcostly patients, leaders shouldfurther stratify patients within thenavigator program to provideadequate support to those whoneed it most.As shown here, Premierstratifies patients in their Top1% Navigator Program intothree different groups, based onhow much support they need.Low-touch patients meetmonthly with the RN navigator.To make sure they stay ontrack, an LPN or health coachcalls them every other week tocheck in.Medium-touch patients meetweekly with the RN navigator,twice per month with the MSWnavigator, and three times permonth with an LPN. An LPN orhealth coach also calls mediumtouch patients every other week.High-touch patients receive themost hands-on support. Inaddition to multiple visits withthe two navigators each month,they have several in-person andtelephone check-ins with othermembers of the care team.Finally, the RN navigatorobserves select3 high-touchpatients through remotetelemonitoring.Scaling Support to Level of Patient RiskElements of Naviga
Mayo Clinic Rochester, MN Lisa Carter Debra Cox Pam Johnson Victor Montori Methodist Le Bonheur Healthcare Memphis, TN Sally Aldrich Kimberly Lamar Nikki Polis mHealth Solutions Larkspur, CA Andrew Dick Premier Health Dayton, OH Barbara Johnson Sylvain Trepanier Scripps Health San Diego, CA Athena Philis-Tsimikas The Center for Health Care Services