Transcription
Research ReportThe State of Ultrasound Education in U.S.Medical Schools: Results of a National SurveyDavid P. Bahner, MD, RDMS, Ellen Goldman, EdD, David Way, MEd,Nelson A. Royall, MD, and Yiju Teresa Liu, MDAbstractPurposeTo determine the state of ultrasoundeducation in U.S. medical schoolsand assess curricular administrators’opinions on its integrationin undergraduate medicaleducation (UME).MethodIn 2012, curricular administrators at134 U.S. MD-granting medical schoolswere surveyed concerning the nature ofultrasound education in medical school.The questionnaire sought ultrasoundeducation program characteristics,structures, and objectives. It also soughtrespondents’ opinions on the role ofultrasound education in UME andUltrasound is an expanding tool inmodern patient care that allows forphysician-performed, rapid bedsideevaluation and interventional managementof patients with portable ultrasoundequipment.1 Unlike traditional, compre hensive ultrasonography, where both atechnologist and a radiologist attempt toanswer a series of diagnostic questions,focused ultrasonography enables asingle clinician to perform a bedsideassessment to answer a select series ofclinical questions and simultaneouslyinterpret and use the findings.2,3 Evidenceshows that focused ultrasonographycontributes to improved patient safety,higher patient satisfaction, and faster andmore cost-effective medical care.1 Yeteven though focused ultrasonographyPlease see the end of this article for informationabout the authors.Correspondence should be addressed to Dr. Bahner,Ohio State University College of Medicine, 756Prior Hall, 376 W. 10th Ave., Columbus, OH 43210;telephone: (614) 293-7380; e-mail: david.bahner@osumc.edu.Acad Med. 2014;89:1681–1686.First published online August 5, 2014doi: 10.1097/ACM.0000000000000414Supplemental digital content for this article isavailable at http://links.lww.com/ACADMED/A222.barriers to its integration. Frequency anddistribution analyses were conductedfor survey responses; Rasch analysis wasperformed for barrier responses.ResultsResponses were received from 82(61.2%) medical schools; theseinstitutions were representative of theU.S. medical school population. Fiftyone respondents (62.2%) reportedultrasound training was integratedinto their UME curriculum. Ultrasoundwas most commonly taught in thethird year (38/82; 46.3%), and thepurpose of training varied by curricularyear. There was agreement thatultrasound should be part of the UMEhas become the standard of care formany clinical scenarios, integration ofultrasound education programs into theundergraduate medical education modelremains a challenge.1,4Historically, the adoption of innovationsinto the medical paradigm is a processcharacterized by slow adoption until anational consensus is reached amongmedical leaders.5 Despite a technologicalrevolution, including societal adoptionof electronics, the structure of theU.S. medical school system remainsrooted in its original paradigm.6Although integration of focusedultrasound training offers opportunitiesto provide instruction in the use ofnovel educational and clinical practicetools, efforts to integrate ultrasoundtechnologies into undergraduate medicaleducation are limited, and a nationalconsensus has not been reached regardingtheir role in the medical educationsystem.7–10To date, graduate medical education(GME) programs have served aspioneers in ultrasound training. Infact, the Accreditation Council forGraduate Medical Education has specificAcademic Medicine, Vol. 89, No. 12 / December 2014curriculum (56/71; 78.9%), but fewrespondents reported it was a priorityat their institution (13/70; 18.6%).Respondents perceived lack of space inthe curriculum (logit 0.49; standarderror [SE] 0.11) and lack of financialsupport (logit 0.42; SE 0.11) as themost significant barriers to integration.ConclusionsDespite a general consensus thatultrasound is an important skill to teachin medical school, the integration ofultrasound education in U.S. schools ishighly variable. This study indicates aneed for national standards to guide theintegration of ultrasound education intoU.S. medical school curricula.requirements for ultrasound educationin specialties such as emergencymedicine, internal medicine, radiology,and obstetrics–gynecology.11–14 Thedevelopment of focused ultrasoundapplications across most specialtieshas led to growing interest amongundergraduate medical educators indeveloping their own ultrasound trainingprograms. Those programs that havebeen described in the literature rangefrom monthlong, specific courses tovertical four-year curricula.8,10,15–19 Earlystudies have shown that such programsnot only receive high satisfaction ratingsfrom medical students but also enhancemedical students’ overall knowledge base,improve the accuracy of their physicalexamination skills, and improve theircomprehension of relevant anatomy andphysiology.18–20Ultrasound education in U.S. medicalschools appears to be limited to programsat isolated institutions (the innovatorsand early adopters) and lacks a nationaldiffusion strategy.5 As diffusion ofeducational innovations follows the samepattern as diffusion of technologicalinnovations, there is a need for athorough understanding of the current1681
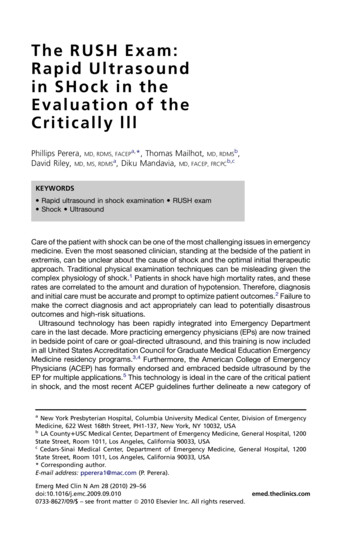
Research Reportlandscape with regard to ultrasoundeducation in U.S. medical schools andpotential barriers to its adoption. Suchan understanding will drive support forthe development of national guidelines toassist medical educators with integratingultrasound training into curricula at theundergraduate level.Therefore, in this study, we sought todetermine the current state of ultrasoundeducation in U.S. undergraduate medicaleducation. We also sought to exploremedical school administrators’ opinionsregarding ultrasound education andtheir perceptions of potential barriers toits integration into the medical schoolcurriculum. We hypothesized thatultrasound education diffusion was limitedto innovators and early adopters and thatthe most significant barrier to adoptionwas the presence of trained faculty capableof developing these programs.MethodIn 2011, we developed an eight-part, tieredquestionnaire for use in determiningthe level of integration of ultrasoundeducation within U.S. medical schoolcurricula. We considered ultrasoundintegration to be present if either lecturesor hands-on experiences with ultrasoundwere available to medical students duringthe preclinical or clinical years. Weconsidered both optional and requiredprograms as integration of ultrasoundeducation for the purposes of the study.We chose to exclude the term “focused”from the survey because of a lack offamiliarity with this terminology amongour target participants, medical schooladministrators.Respondents who reported ultrasoundeducation integration at their medicalschool were asked whether the ultrasoundexperiences were required, optional,or both. These respondents were alsoasked at what levels in the medicalschool curriculum and for what primarypurpose (knowledge enrichment, skillstraining, or other) ultrasound was taught.Additionally, respondents’ opinions aboutintegration of ultrasound education intothe medical education paradigm weresought; they were asked to rate their levelof agreement with eight statements using afive-point Likert scale. Finally, respondentswere asked to rank order, from most toleast significant, five potential barriersto integrating ultrasound into the1682undergraduate medical curriculum.Demographic information was also sought(respondent’s role and medical schoolcurriculum model).survey to nonrespondents to encouragesurvey completion. Survey collectioncontinued through April 2012, for a totalof three months.Prior to administration, the questionnairewas critically reviewed by two deansinvolved in curriculum design at the OhioState University College of Medicine andGeorge Washington University Schoolof Medicine and Health Sciences and asurvey development expert to identifyissues with survey structure and questiondesign. We subsequently modified thequestionnaire on the basis of theirfeedback. The final questionnaire (seeSupplemental Digital Appendix 1 athttp://links.lww.com/ACADMED/A222)was administered through an onlinesurvey service (SurveyMonkey, Palo Alto,California). The investigators were blindedto respondents’ institution informationprior to data analysis.Data analysisThe survey and study design werereviewed and approved by the Ohio StateUniversity institutional review board. Thestudy was deemed exempt from reviewby the George Washington Universityinstitutional review board.ParticipantsAt the time of the study in early 2012,there were 134 U.S. MD-granting medicalschools that were fully accredited by theLiaison Committee on Medical Education(LCME). (We excluded medical schoolsoperating under provisional LCMEaccreditation to ensure that curricularinformation would be available for allfour medical school years.) We identifieddeans for education and curriculumdesign (or equivalent faculty members)as the target participants because of theirfamiliarity with curriculum design andupcoming changes. We obtained contactinformation for the target participantat each medical school through areview of the school’s Web site or atelephone discussion with the school’sadministration office. We confirmedcontact information by contacting eachschool prior to survey administration.Survey administrationIn February 2012, we sent an initial e-mailinvitation to the 134 target participants;this message contained a cover letter and alink to the online survey. We sent followup e-mail reminders to nonrespondentsafter one week and three weeks. Afterone month, we mailed a hard copy of theWe determined frequency and percentagedistributions for respondent andinstitutional demographics (see below),curriculum models, and integration ofultrasound education. We performedchi-square tests and Fisher exact teststo evaluate whether our return samplewas representative of the population ofall fully accredited U.S. MD-grantingmedical schools. The institutionaldemographic categories we evaluatedwere faculty size (percentile),21 institutiontype (public or private),22 U.S. News &World Report research ranking,22 andAssociation of American Medical Collegesregional affiliation.23 Additionally,we performed frequency analysis forresponses regarding respondents’opinions on the integration of ultrasoundeducation in undergraduate medicalcurricula. All descriptive data analyseswere performed using SPSS version 17.0(SPSS Inc, Chicago, Illinois).We performed a Rasch analysis toevaluate responses regarding potentialbarriers to the integration of ultrasoundeducation.24 Rankings were convertedto Rasch logits with Winsteps Raschmeasurement software (version 3.75.0,Winsteps Inc, Beaverton, Oregon).25 Inthis analysis, Rasch logits represent themeasure of difficulty the barrier poses.A large and positive logit value indicatesa significant challenge to integratingultrasound education, whereas a small ornegative value indicates a relatively lesschallenging barrier. Incomplete surveyswere included in the study; however,missing responses were omitted duringstatistical analysis.ResultsWe received responses from 82 (61.2%)of the fully accredited 134 U.S. MDgranting medical schools. Our evaluationof these institutions’ demographicsindicated that they were representativeof the study population (see Table 1).Of the respondents, 71 (86.6%) helddecanal positions, 6 (7.3%) heldacademic program leader positions, and5 (6.1%) were designated as the “facultychampion” of ultrasound in medicaleducation at their institution.Academic Medicine, Vol. 89, No. 12 / December 2014
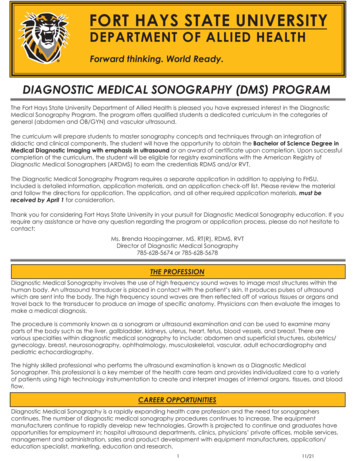
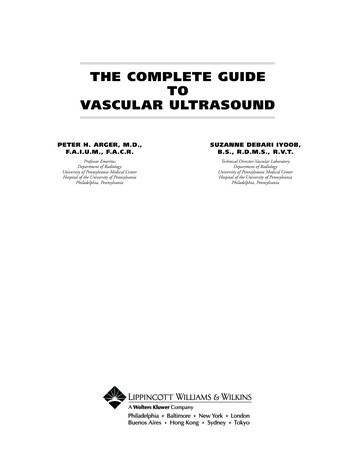
Research ReportTable 1Characteristics of the 134 U.S. MD-Granting Medical Schools Invited to Participatein a National Survey of Deans of Education/Curricular Leaders on the State ofUndergraduate Ultrasound Education, 2012aNo. (%) of institutionsTotal no. ofinstitutions Respondents NonrespondentsCharacteristicResponseFaculty sizeb13482 (61)52 (39) 25th percentile3421 (62)13 (38)25th–50th percentile3322 (67)11 (33)51st–75th percentile3420 (59)14 (41) 75th percentile3319 (58)14 (42)Research rankingcTop 10106 (60)4 (40)11–25158 (53)7 (47)26–502516 (64)9 (36) 508452 (62)32 (38)Northeast3723 (62)14 (38)Central3421 (62)13 (38)South4628 (61)18 (39)West1710 (59)7 (41)Private5029 (58)21 (42)Public8454 (64)30 (36)RegiondInstitution typecχ2 df P value0.683.880.683.880.063.990.591.46χ tests of proportion were used to determine whether the respondent sample was representative of thepopulation.bFaculty size data are based on the Association of American Medical Colleges (AAMC), U.S. Medical School Faculty,2011.21cResearch ranking and institution type are based on U.S. News & World Report’s Best Medical Schools, 2012.22dRegion is based on AAMC regional affiliation, from the AAMC Organizational Characteristics Database, 2012.23a 2Most of the 82 respondents describedtheir medical school’s preclinicalcurriculum as an organ systems model(32; 39.0%) or a hybrid model of organsystems and basic science curricula(33; 40.2%). Few reported disciplinebased (12; 14.6%) or problem-based(2; 2.4%) models. The majority ofrespondents described their institution’sclinical curriculum as discipline-basedblock rotations (65; 79.3%), with therest reporting longitudinal integratedrotations (3; 3.7%) or mixed-modelrotations (13; 15.9%). Two respondentsdid not indicate a preclinical curriculummodel, and one respondent did notidentify a clinical curriculum model.Integration of ultrasound educationFifty-one (62.2%) of the 82 respondentsreported that ultrasound educationwas integrated within their medicalschool’s curriculum. Table 2 shows thecharacteristics of responding medicalschools’ ultrasound education programsby medical school year. We foundultrasound education to be relativelyevenly dispersed across medical schoolyears. However, the most commonlyreported medical school level withultrasound training was the third year(38/82; 46.3%). We found no evidence ofa relationship between curriculum modeland ultrasound training integration atthe preclinical level (χ2 1.72; df 1;P .19) or the clinical level (χ2 1.14;df 1; P .29).The primary purpose of ultrasoundtraining varied by year of the medicalschool curriculum, as shown in Table 3.The majority of respondents at schoolsthat taught ultrasound in the first orsecond year of medical school indicatedthat it was used as a tool for teachingbasic science or medicine topics (27/31[87.1%] and 20/29 [69.0%], respectively).In contrast, third- and fourth-yearultrasound education programs wereprimarily designed to teach students howto obtain ultrasound scans (6/37 [16.2%]and 5/35 [14.3%], respectively) and howto interpret ultrasound scans (20/37[54.1%] and 18/35 [51.4%], respectively).Few respondents (3/51; 5.9%) reportedteaching students procedural guidanceusing ultrasound.Table 2Characteristics of Ultrasound Education Programs at U.S. MD-Granting MedicalSchools, as Reported by Deans of Education/Curricular Leaders, National Survey onState of Ultrasound Education, 2012aCurriculum integration,no. (%) of programsbTraining type,no. (%) of programsUltrasound educationprogram, no. (% of 82medical 1231 (37.8)29 (35.4)20 (64.5)19 (65.5)9 (29.0)7 (24.1)2 (6.5)2 (6.9)27 (87.1)25 (86.2)3 (9.7)2 (6.9)1 (3.2)1 (3.4)338 (46.3)20 (52.6)13 (34.2)4 (10.5)23 (60.5)11 (28.9)2 (5.3)435 (42.7)15 (42.9)13 (37.1)6 (17.1)9 (25.7)23 (65.7)3 (8.6)Medicalschool yearOf the 82 respondents, 51 (62.2%) reported that ultrasound education was integrated into one or more years oftheir medical school curriculum.bFormal integration indicates an ultrasound educational program contained within the medical school curriculum,whereas cocurricular integration indicates a program conducted outside the formal curriculum (e.g., interest group,student society).aAcademic Medicine, Vol. 89, No. 12 / December 20141683
Research ReportTable 3Primary Purposes of Ultrasound Education Programs Within Medical SchoolCurricula as Reported by Deans of Education/Curricular Leaders at U.S. MD-GrantingMedical Schools, National Survey on State of Ultrasound Education, 2012Year of medical school curriculum,no. (%) of respondentsPurpose of ultrasoundtrainingYear 1(n 31)Year 2(n 29)Year 3(n 37a)Year 4(n 35)Tool for teaching science ormedicine topicsTrain students to obtainultrasound scans27 (87.1)20 (69.0)6 (16.2)5 (14.3)1 (3.2)2 (6.9)6 (16.2)5 (14.3)2 (6.5)5 (17.2)20 (54.1)18 (51.4)0 (0)0 (0)0 (0)3 (8.6)1 (3.2)2 (6.9)5 (13.5)4 (11.4)Train students to interpretultrasound scansTrain students to use forultrasound-guided procedureOtheraA single school did not complete the survey items regarding the purpose of the ultrasound educationprogram and was omitted from this analysis.Perceptions of ultrasound in medicalschoolsRespondents’ attitudes regarding therole of ultrasound education within themedical education paradigm are shownin Table 4. There was a general consensusthat ultrasound education should beintegrated into medical school curricula(56/71 [78.9%] agreed or strongly agreed).Furthermore, respondents generallydisagreed or were neutral (42/70; 60.0%) tothe idea that ultrasound education wouldbe more appropriate at the GME level.However, only 13 (18.6%) of 70 respondentsbelieved that ultrasound education was apriority at their medical school.Table 4Medical School Curricular Administrators’ Opinions on the Role of UltrasoundEducation in Medical Education, National Survey on the State of UltrasoundEducation, 2012aAgree orstrongly agree,no. (%)Disagreeor stronglydisagree, no. (%)Neutral,no. (%)56 (78.9)4 (5.6)11 (15.5)22 (31.0)27 (38.0)22 (31.0)34 (49.3)13 (18.8)22 (31.9)7 (9.9)44 (62.0)20 (28.2)Ultrasound facilitates a medicalstudent’s ability to diagnose medicalproblems (n 72)58 (80.6)5 (6.9)9 (12.5)Ultrasound is more appropriate forgraduate medical education (n 70)28 (40.0)27 (38.6)15 (21.4)Ultrasound-guided procedures canimprove patient safety (n 71)70 (98.6)0 (0)1 (1.4)Ultrasound education is a priority atmy medical school (n 70)13 (18.6)34 (48.6)23 (32.9)Item (no. of respondents)Ultrasound should be a part of theundergraduate medical educationcurriculum (n 71)The best place for ultrasound in theundergraduate curriculum is in ananatomy course (n 71)The best place for ultrasound in theundergraduate curriculum is in theclinical clerkships (n 69)Due to the amount of material in ourundergraduate medical curriculum,ultrasound cannot be accommodated(n 71)Respondents were deans of education or equivalent curricular leaders at 82 U.S. MD-granting medical schools.a1684Respondents’ perceptions of barriers toultrasound education integration intoundergraduate medical education and theresults of our Rasch analysis are shownin Table 5. The two most significantbarriers were lack of space in the currentcurriculum (logit 0.49; standard error[SE] 0.11) and lack of financial support(logit 0.42; SE 0.11). Less significantbarriers were a lack of ultrasoundequipment (logit 0.18; SE 0.10)and lack of trained faculty (logit –0.09;SE 0.10). Lack of student interest wasnot perceived as a significant barrier(logit –1.00; SE 0.14).DiscussionThe adoption of technologies andinnovations in medicine appears tofollow a predictable pattern that relieson a serial progression of adopters, frominnovators through laggards.5 Unlikeother innovations in medicine, focusedultrasonography requires diffusion of boththe portable technology and techniques.Although focused ultrasound equipmenthas become increasingly more prevalent,with multiple specialties now usingfocused ultrasonography, the diffusion ofmany novel applications remains in theearly phases.26 Building support for thedevelopment and adoption of nationalstandards for ultrasound education,however, will likely require significantimprovements in and expansion ofultrasound education within the medicaleducation paradigm.The majority of ultrasound trainingcurrently takes place in the GME system.Adding focused ultrasound education toresidency training requirements may not befeasible, given that residency programs faceincreasing time and financial constraints.As ultrasound equipment continuesto become more portable and moreaffordable, and its utility rapidly expandsin clinical practice and as a teaching aid,we believe it is reasonable to considerwhether ultrasonography should be part ofthe medical school curriculum.9,10 A recentCarnegie Foundation Report, “EducatingPhysicians: A Call for Reform of MedicalSchool and Residency,” stresses that theinitial years of medical education should bestrengthened by incorporating more clinicalexperiences than those that currently exist.6Creating national guidelines for ultrasoundeducation programs in medical schoolscould be one way to increase medicalstudents’ early clinical exposures.Academic Medicine, Vol. 89, No. 12 / December 2014
Research ReportTable 5Medical School Curricular Administrators’ Ranking of Potential Barriers toIntegration of Ultrasound Education Into Medical School Curricula, NationalSurvey on the State of Ultrasound Education, 2012aResponse frequency, no. (% of 69)Rasch logitscStandarderrorRank12345Lack of space in currentcurriculumLack of financial support 0.490.11117 (25)19 (28)18 (26)12 (17)3 (4) 0.420.11215 (22)24 (35)10 (14)15 (22)5 (7)Lack of ultrasound equipment 0.180.10315 (22)14 (20)14 (20)16 (23)10 (14)Lack of trained faculty–0.090.1049 (13)13 (19)17 (25)12 (17)18 (26)Lack of student interest–1.000.1451 (1)4 (6)9 (13)18 (26)37 (54)Potential barrierbData are based on responses to the following survey item: “Please rank the following challenges to integratingultrasound into the medical school curriculum. Make ‘1’ the most significant barrier and ‘5’ the least significantbarrier.” Respondents were deans of education or equivalent curricular leaders at U.S. MD-granting medical schools.bBarriers are listed from most (1) to least (5) significant.cFit statistics were all within the acceptable range of 2.0 to 2.0.aThis study provides an overview of thestatus of ultrasound education in U.S.MD-granting medical schools. Our resultsindicate that a majority of medical schoolcurriculum leaders agree that ultrasoundeducation is more suited for undergraduateprograms than GME programs. However,it appears that only 62% of medical schoolsinclude ultrasound education at any pointin the curriculum. Given that the majorityof these ultrasound experiences occurduring the clinical years of the curriculum,the training provided is likely highlyvariable, as has been shown in rotationbased education.27,28 Considering that U.S.medical schools graduate more than 18,000students per year,29 this lack of consistentultrasound education creates a significanteducational strain on GME programs,requiring them to provide untrainedinterns and residents with both novice andadvanced levels of ultrasound training.Although there appears to be a consensusamong respondents that there is a needfor integration of ultrasonography inthe medical school curriculum, thereare clearly barriers which currently limitfurther adoption. Curriculum leaderswere concerned about adding content tothe current curriculum, possibly giventhe poor knowledge retention ratesreported among students in voluminouscurricula.30–32 Other barriers to integrationwere related to resources necessary forultrasound training programs. Forexample, the capital costs involvedinclude the purchase and maintenance ofultrasound equipment as well as hiringand training faculty. Lastly, few matureprograms exist at the undergraduatelevel.9,10,15,16 There has yet to be published amodel ultrasound curriculum that medicalschools can use to guide their developmentof new, integrated ultrasound experiences.These are all significant barriers to thedevelopment of comprehensive, standardultrasound training requirements, whichwill be necessary to encourage furtheradoption among medical schools in theUnited States.LimitationsAlthough this study had an adequateresponse rate and we demonstratedthat the participating institutions wererepresentative of U.S. MD-grantingmedical schools, the respondents maynot have been aware of all availableultrasound education programs withintheir institution’s curriculum. Whereastraditional ultrasound applications arespecific to radiology and obstetrics–gynecology specialists, more novelapproaches, such as focused ultrasound,are spread across other medicalspecialties to varying degrees. As there isa predominance of ultrasound trainingprograms within emergency medicine,the majority of ultrasound training maybe taught by emergency medicine facultyduring clinical clerkships; however, wewere unable to evaluate for this or otherspecialty-specific biases.33 Additionally,excluding new, provisionally accreditedmedical schools from our study may havehad the effect of underestimating thetrue prevalence of integrated ultrasoundeducation programs because thesenew medical schools have the abilityto develop novel training programs,such as in focused ultrasonography, apriori. Finally, there is the potential thatrespondents did not report in-processAcademic Medicine, Vol. 89, No. 12 / December 2014revisions to curricula, which couldinclude ultrasound education efforts.ConclusionsDiffusion of ultrasound education intoundergraduate medical education hasbegun only recently, despite evidencesupporting the use of ultrasonography inclinical practice. Among those medicalschools that have adopted ultrasoundtraining, there appear to be benefits tointegration in both the preclinical andclinical curricula. There is therefore aneed for the development of nationalstandards to facilitate widespreadadoption of ultrasound education inmedical school curricula.Funding/Support: This study was supportedfinancially by the Office of the Dean, GeorgeWashington University School of Medicine andHealth Sciences, Washington, DC.Other disclosures: None reported.Ethical approval: The study was approved bythe institutional review board at Ohio StateUniversity. The study was deemed exempt fromreview by the institutional review board atGeorge Washington University.Dr. Bahner is professor, director of ultrasound, andemergency medicine ultrasound fellowship director,Department of Emergency Medicine, Ohio StateUniversity College of Medicine, Columbus, Ohio.Dr. Goldman is associate professor, Departmentof Human and Organizational Learning, anddirector, Master Teacher Leadership DevelopmentProgram for the School of Medicine and HealthSciences, George Washington University,Washington, DC.Mr. Way is senior research associate, Ohio StateUniversity College of Medicine, Columbus, Ohio.Dr. Royall is a fourth-year resident in surgery,Department of Surgery, Orlando Health, Orlando,1685
Research ReportFlorida. He holds a joint appointment as residentinstructor, Department of Clinical Sciences, University ofCentral Florida College of Medicine, Orlando, Florida.Dr. Liu is assistant professor and emergencymedicine ultrasound fellowship director, Departmentof Emergency Medicine, George WashingtonUniversity School of Medicine and Health Sciences,Washington, DC.References1 Moore CL, Copel JA. Point-of-careultrasonography. N Engl J Med.2011;364:749–757.2 Greenbaum LD, Benson CB, Nelson LH 3rd,Bahner DP, Spitz JL, Platt LD. Proceedingsof the Compact Ultrasound Conferencesponsored by the American Institute ofUltrasound in Medicine. J Ultrasound Med.2004;23:1249–1254.3 Bahner DP, Hughes D, Royall NA. I-AIM: Anovel model for teaching and performingfocused ultrasound. J Ultrasound Med.2012;31:295–300.4 Rothschild JM. Chapter 21: Ultrasoundguidance of central vein catheterization. In:Agency for Healthcare Research and Quality,ed. Making Health Care Safer: A CriticalAnalysis of Patient Safety Practices. AHRQpublication 01-E058. Rockville, Md: Agencyfor Healthcare Research and Quality; 1.htm. Accessed May 23, 2014.5 Rogers EM. Diffusion of Innovations. 5th ed.New York, NY: Free Press; 2003.6 Cooke M, Irby DM, O’Brien BC. EducatingPhysicians: A Call for Reform of MedicalSchool and Residency. San Francisco, Calif:Jossey-Bass; 2010.7 Wittich CM, Montgomery SC, Neben MA,et al. Teaching cardiovascular anatomyto medical students by using a handheldultrasound device. JAMA. 2002;288:1062–1063.8 Hoppmann R, Cook T, Hunt P, et al.Ultrasound in medical education: A verticalcurriculum at the University of SouthCarolina School of Medicine. J S C MedAssoc. 2006;102:330–334.9 Bahner DP, Royall NA. Advanced ultrasoundtraining for fourth-year medical students:A novel training program at the Ohio StateUniversity College of Medicine. Acad Med.2013;88:206–213.10 Bahner DP, Adkins EJ, Hughes D, BarrieM, Boulger CT, Royall NA. Integratedmedical school ultrasound: Developmentof an ultrasound vertical curriculum. CritUltrasound J. 2013;5:1–9.168611 Accreditation Council for Graduate MedicalEducation. ACGME Program Requirementsfor Graduate Medical Education in EmergencyMedicine. Effective July 1, 2013. 013-PR-FAQ-PIF/110 emergencymedicine 07012013.pdf. Accessed May 23, 2014.12 Accreditation Council for Graduate MedicalEducation. ACGME Program Requirementsfor Graduate Medical Education in InternalMedicine. Effective July 1, 2013. 013-PR-FAQ-PIF/140 internalmedicine 07012013.pdf. Accessed May 23,2014.13 Accreditation Council for Graduate MedicalEducation. ACGME Program Requirementsfor Graduate Medical Education inDiagnostic Radiology. Effective July 1, sets/2013-PR-FAQ-PIF/420 diagnosticradiology 07012013.pdf. Accessed May 23,2014.14 Accreditation Council for Graduate MedicalEducation. ACGME Program Requirementsfor Graduate Medical Education inObstetrics and Gynecology. Effective January1, 2008. https://www.acgme.o
characteristics of responding medical schools' ultrasound education programs by medical school year. We found ultrasound education to be relatively evenly dispersed across medical school years. However, the most commonly reported medical school level with ultrasound training was the third year (38/82; 46.3%). We found no evidence of Medical