Transcription
Fiscal Year 2021-2022 DepartmentPerformance Plan
ContentsIntroduction. 3Department Overview . 3Mission and Vision. 5Organizational Chart . 6Department Descriptions . 6Environment . 8Fiscal Year 2020-2021, Q3: Performance Evaluation .14Fiscal Year 2021-2022: Wildly Important Goals & Measures.29Fiscal Year 2021-2022: Department Pillars .32Glossary.372
IntroductionThe Colorado Department of Health Care Policy & Financing Fiscal Year (FY) 20212022 performance plan is an annual report on progress made toward achieving ourmission and supporting goals. This report includes accomplishments, project status,findings, data, and policy and administrative difficulties in the operation of ourprograms as of FY 20-2021, Quarter 3. This report is completed for the ColoradoGeneral Assembly; stakeholders, providers, and contractors; the people of Colorado;and staff of the Department of Health Care Policy & Financing (herein referred toas “HCPF”).For reference, a glossary of acronyms and relevant terms is at the end ofthis document.Department OverviewHCPF is the single Colorado state agency responsible for administering the Medicaidprogram (Title XIX of the Social Security Act) and the Children’s Health InsuranceProgram (Title XXI of the Social Security Act). Colorado’s Medicaid program is calledHealth First Colorado and our Children’s Health Insurance Program is called ChildHealth Plan Plus (CHP ). In addition to these programs, HCPF administers theColorado Indigent Care Program (CICP), the Old Age Pension State Medical Program,the Primary Care Fund, and the School Health Services Program. We also providehealth care policy leadership – affordability best practices, health care innovationopportunities, policy guidance, and subject matter expertise – for the state’sexecutive branch, legislative branch, and to purchasers. As the largest payer in thestate – now covering 1 in 4 Coloradans through this COVID-19 economic downturn – wealso collaborate with the state’s largest insurance carrier payers to create bestpractices on shared initiatives to the benefit of Coloradans like value based paymentsor innovations like the prescriber tool, eConsults, centers of distinction (previouslycenters of excellence), and more. The Department also oversees the state’s All-PayerClaims-Database (APCD).HCPF does not directly provide or deliver medical services; rather, we administer anetwork of public and private providers who render services to members. We serveColoradans who are eligible for and/or enrolled in Health First Colorado and CHP ,and those who receive services through the other programs described above. Inserving these customers, we partner with medical, dental, behavioral health, vision,and other medical care providers, as well as long-term services and supportsproviders; other state agencies; the Centers for Medicare & Medicaid Services (CMS);groups that advocate for member populations; the Governor’s Office and the ColoradoGeneral Assembly; service contractors; expert consultants and advisors; variousnonprofit entities; commercial carriers; and entities that help individuals apply forbenefits such as Colorado counties, local government agencies, and medical3
assistance sites.Health First Colorado receives approximately 63% of its funding from the federalgovernment, while CHP is approximately 67% federally funded. Less than 4%of HCPF’s budget goes to administrative costs, while 96% goes to health careprovider payments.4
Mission and VisionOur Mission:Improving health care equity, access and outcomesfor the people we serve while saving Coloradansmoney on health care and driving value for Colorado.Our Vision:Coloradans have integrated health care andenjoy physical, mental and social well-being.HCPF modernized its mission this year, after engagement with stakeholders includingthe Member Experience Advisory Committee (MEAC, which includes Health FirstColorado and CHP members), the Program Improvement Advisory Committee (PIAC,which includes providers, advocates, and various stakeholders), and HCPF employees.The new mission statement has three new points of emphasis: first, our commitmentto health care equity; second, our increased focus on Medicaid cost controlrecognizing our increased membership, the programs impact on the state budget, andthe importance of member benefit as well as provider reimbursement protection;third, our work supporting health care affordability for all Coloradans. These keyconcepts are reflected in our goals and work this past year and will inform our work inthe coming year.5
Organizational ChartDepartment DescriptionsExecutive Director’s Office: Kim Bimestefer was appointed Executive Director of theDepartment by Governor Jared Polis after her first appointment effective January 8,2018. The Executive Director is responsible for setting the strategic direction of HCPF;creating alignment with other state agencies to achieve the health care agenda of theGovernor; overseeing the operations and programs of the Department which areprovided by both employees and contractors and ensuring HCPF operates in anefficient and effective manner; and leading HCPF to achieve its vision, mission, andannual goals. The office also leads collaborative efforts to drive down health carecosts and prices to the benefit of Coloradans, their employers, Medicaid, CHP , andthe state. Lastly, this office oversees human resources and learning and developmentto support HCPF employees.Cost Control & Quality Improvement Office: The Cost Control & QualityImprovement Office was established July 1, 2018, by the Medicaid Cost Containmentlaw (SB18-266) 1. This office manages the data repositories and tools, using theseresources to produce directional analyzes such as utilization, unit cost, quality, andoverall cost trends for Health First Colorado, CHP , and other health care safety netprograms administered by HCPF. The office oversees utilization review, populationmanagement, case and disease management, quality scorecard metrics, and costmanagement strategy, vendors, and program effectiveness, while sharing RegionalAccountable Entity innovations and performance evaluation with the Health PolicyOffice The office also secures insights into cost trend drivers and evolvingutilization iles/documents/2018A/bills/2018a 266 enr.pdf6
Health Programs Office: The Health Programs Office oversees Health First Coloradoand CHP acute care, physical, and behavioral health programs. The office managesbenefit policy development and oversight and is responsible for key functionsincluding benefit coverage appeals, federal and state compliance activities, and theAccountable Care Collaborative.Medicaid Operations Office: The Medicaid Operations Office oversees fraud, wasteand abuse function and the Medicaid and CHP health plan operations performed byboth Department employees and third-party contractors. In addition, this officeestablishes and monitors the operational performance standards for internaloperations as well as for Department contractors. Operations includes claimspayments, member and provider call centers, member enrollment, eligibilitydeterminations made by contracted partners, and provider network management.Policy, Communications and Administration Office: The Policy, Communications andAdministration Office manages the legislative agenda, government affairs,communications and media relations, and legal affairs. This includes collaboratingwith our stakeholders in the General Assembly, our county human servicesadministration, local public health and county commissioners, as well as our federallyrecognized tribes and urban American Indian communities.Health Information Office: The Health Information Office (HIO) develops,implements, and maintains HCPF’s claims payment system (Medicaid ManagementInformation System, or MMIS) and HCPF’s data management system (BusinessIntelligence Data Management System, or BIDM). The office also oversees HealthInformation Technology (HIT) projects and related Information Technology (IT)infrastructure. This office coordinates with the Governor’s Office of InformationTechnology, the Office of eHealth Innovation (OeHI), and other stakeholders on HITand IT projects that impact HCPF. In 2021, and in partnership with the MedicaidOperations Office, HIO assumed shared responsibility with OIT and the ColoradoDepartment of Human Services (CDHS) for the management of Colorado BenefitsManagement System (CBMS), the state’s eligibility system.Finance Office: The Finance Office is responsible for the financial strategy,budgeting, accounting, external and internal audits, and risk management andprocurement operations of HCPF. This includes presenting budgetary needs toColorado executive and legislative authorities and forecasting program caseload andexpenditures throughout the fiscal year. The office is also responsible for monitoring,developing, and implementing rates for payments to providers, including value-basedpayments and managed care rate setting.Office of Community Living: The Office of Community Living oversees Health FirstColorado’s long-term services and supports (LESS) programs and manages efforts totransform Colorado’s LTSS system to ensure responsiveness, flexibility, accountability,and person-centered supports for all eligible persons.7
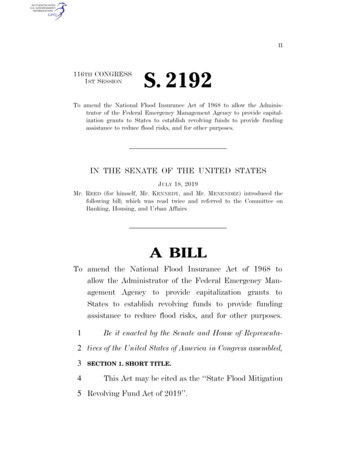
Pharmacy Office: The Pharmacy Office oversees the prescription drug benefitsprovided to Health First Colorado and CHP members. The office is responsible forensuring strong prescription drug policy and clinically appropriate and cost-effectiveuse of medications. Focus areas include the Colorado Preferred Drug List Program;drug-utilization review including analysis and input from the Colorado Drug UtilizationReview Board; value-based contracting; prescription drug affordability policy;reimbursement strategy; and contracting. The office also manages the point-of-salepharmacy claims adjudication system (the Pharmacy Benefit Management System,or PBMS).EnvironmentCOVID-19: The novel coronavirus (COVID-19) pandemic continues to have anunprecedented impact on the health care sector, the economy, and our mostvulnerable Coloradans. More than a year after the pandemic began, more than550,000 Coloradans have been infected and about 6,800 have died from COVID-19.Older Coloradans, those in congregate settings like nursing facilities, obese, andpeople of color disproportionately experienced higher rates of COVID-19 infectionsand related morbidity and mortality.The health care industry has been on the front lines of battling the pandemic, caringfor those infected, building up massive testing infrastructure, and now vaccinatingColoradans at an unprecedented rate. Our health care institutions and professionalshave risen to the challenge, working harder for an unparalleled, sustained length oftime. Health care workforce burnout was an issue even before the pandemic; thelong-term impacts on burnout due to COVID-19 remain unclear.Changes in Economic Conditions: An economic downturn primarily affects HCPF byincreasing Medicaid and CHP enrollment and membership (referred to technically ascaseload). During an economic downturn, unemployment rises, particularly for peoplewith lower incomes. As a result, membership rises rapidly. This was indeed trueduring the pandemic. After an extended period of declining enrollment in Medicaidand CHP , a dramatic increase began in April 2020 (see chart below). As of May 2021,the total number of Medicaid members increased from 1.25 million to 1.5 million,which is an increase of 20% in 13 months. Additionally, the federal governmentrequired medical assistance program coverage to be continuous during the declaredpublic health emergency (PHE), so people enrolled in Medicaid during the PHE havein most cases maintained their Medicaid coverage (more details are in thefollowing section).8
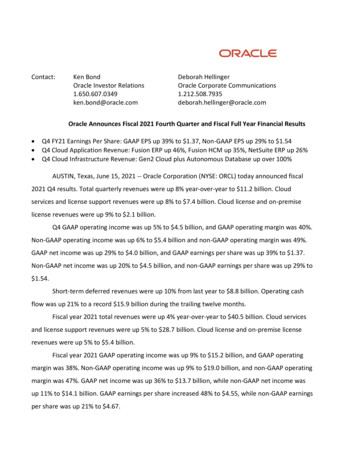
The influx in Medicaid and CHP members resulted in increased costs to the state at atime when the state had lower General Fund revenues. Even after the declared PHEends, and as Colorado’s economy recovers, program membership will likely remainabove pre-pandemic levels for some time. That is because people earning lowerwages suffered more job losses and are gaining those jobs back more slowly thanpeople earning medium or higher wages (see chart below from Colorado Departmentof Labor and Employment).HCPF will continue to closely monitor program enrollment. When membership doesstart going down, the Coloradans rising off Medicaid will favor the healthier memberswhile those who remain on Medicaid will be less healthy and have higher averagehealth care costs. The Department’s overall claim costs will go down while the per9
member per month claim costs will rise. Additionally, some Coloradans will haveforgone preventive, routine, and higher levels of needed care during this pandemic,which could lead to worse health outcomes and increased future costs for MedicaidPublic Health Emergency Wind Down: At the beginning of the COVID-19 pandemic,the federal government declared a public health emergency (PHE). In Section 6008 ofthe Families First Coronavirus Response Act, Congress conditioned temporaryenhanced federal Medicaid funding with a requirement that generally prohibits a statefrom disenrolling any individual who was enrolled as of the date of enactment untilthe last day of the month in which the PHE ends. As a result, Colorado must continuehealth care coverage for all medical assistance programs, even if a member’seligibility changes. In addition, Colorado elected to provide this same protection toCHP members. All Medicaid and most CHP members have remained enrolled and areeligible to receive benefits during the PHE. The PHE was recently extended to July 20,2021 and is expected to last through 2021, as per HHS communications.For members receiving Medicaid benefits and some members receiving CHP benefits,Colorado’s counties are responsible for processing eligibility redeterminations.Colorado is a state-supervised, county-administered system for public assistance.HCPF reimburses counties for eligibility determinations based on staffing and relatedadministrative costs. When the PHE ends, HCPF and Colorado’s counties will beresponsible for reviewing eligibility of all members whose coverage and/or benefitswere locked in during the PHE, processing redeterminations, and communicating withMedicaid and CHP members about any changes. Existing federal guidance requiresthat states complete post-enrollment verifications within a timeframe to bedetermined by the Centers for Medicare & Medicaid Services (CMS). Although CMS hasnot yet released official guidance about the end of the PHE, HCPF anticipates thetime frame will be no more than six months from the expiration of the PHE.American Rescue Plan Act of 2021: On March 10, 2021, President Biden signed intolaw the American Rescue Plan Act (ARPA). The ARPA provides 1.9 trillion in relief toaddress the continued impact of COVID-19 on the economy, public health, state andlocal governments, individuals, and businesses. The ARPA includes direct aid for stateand local governments. Legislative Council Staff expect 3.9 billion in state funds and 2.29 billion in local funds for Colorado.The ARPA includes a one-time 10% federal medical assistance percentage (FMAP)increase for Home and Community-Based Services (HCBS). HCPF estimates this couldbe an increase of 550 million, which must be spent by March 31, 2024. The increasedFMAP must be used “to supplement, and not supplant” the level of state fundsexpended for HCBS programs in effect as of April 1, 2021. HCPF is seeking to leveragethese funds for: COVID-19 response and recovery, supercharging existing initiativesand advancing system reform, and investing in infrastructure that has a long-termbenefit to the system and people of Colorado. HCPF collaborated with the JointBudget Committee to develop legislation to govern the use of the HCBS funding. HCPFis engaging providers, members, advocates, and stakeholders closely. We established10
a new website, 2 held a series of stakeholder meetings, and are collecting publiccomments. Colorado’s spending plan for this funding is contingent upon CMS approvaland the JBC. HCPF will continue to work closely with the Governor's Office, theLegislature, and stakeholders on how to utilize any ARPA funding allocated to HCPF.Mental Health Care in Colorado: Colorado is, overall, a physically healthy state,ranking #6 in the nation on the 2020 Commonwealth Fund’s Overall Health Ranking. 3However, in terms of mental health, Colorado lags far behind other states, ranking#47 (out of 50 states and Washington DC) for overall mental health in the MentalHealth America rankings. 4 Over fifteen percent of Coloradans reported poor mentalhealth in 2019, up from 11.8% in 2017. 5 In Colorado, in April/May 2021, 30.8% ofColoradan adults reported symptoms of anxiety and/or depressive disorder. Deaths inthe state from drug overdose increased from 16.9 per 100,000 population in 2015 to25.6 per 100,000 in 2020. 6 In 2019, Colorado had the fifth-highest suicide rate inthe nation. 7Many Coloradans report they are not able to access timely care because the servicesthey need are not available in their communities, wait times are too long, orproviders are unable to accommodate their disabilities. In a 2019 survey, 13.5% ofColoradans reported that they did not get mental health treatment that they needed,8and over 95,000 Coloradans 18 and older (2.3%) did not get treatment or counselingto address substance use disorder in 2019. 9 Mental Health America ranked Colorado31st worst among states in terms of access to care. 10 With approximately 1 millionpeople in Colorado in need of behavioral health services, Colorado needs acomprehensive system that puts people first, and that is why the Department isdedicated to continue working with our communities and state partners to implementbehavioral health reform in Colorado.Increasing Health Care Costs: The affordability of health care continues to be one ofthe most significant challenges facing HCPF, the state, and the nation. With theeconomic downturn, all payers – self-funded employers and Medicaid alike – benefitfrom a solid affordability strategy. As a trusted health care expert, and in partnershipwith other health care thought leaders, HCPF is focused on research, analytics,and reporting that identify drivers of rising health care costs and strategies toaddress org/sites/default/files/file attachments/2019%20CHAS%20Substance%20Use%20Brief 1.pdf10 e-mental-health-america11
CMS predicts that national health spending is projected to grow at an average rate of5.4% per year between 2019 and 2028, outstripping growth in the nation’s GrossDomestic Product. CMS predicts that Medicaid spending will also grow at a rate of5.5%, which is between the projected rate of Medicare growth at 7.6% and privatehealth insurance growth at 4.8%. CMS identifies that key trends involve rapidincreases in prescription drug spending, hospital spending, and physician andclinical services. 11For Colorado, rising health care costs will continue to create budgetary pressures.While HCPF continues to implement new payment methodologies that condition aportion of reimbursements on outcomes and performance metrics, implement deliverysystem innovations, and regulatory structures that prioritize member health, medicalinflation will continue to be a challenge. Below are prominent environmental factorsaffecting affordability that HCPF has focused on addressing.Prescription drug costs: The high cost of prescription drugs, especially specialtydrugs, is a challenge for Medicaid, CHP , and all health plans. In January 2021,HCPF released the second edition report titled, “Reducing Prescription DrugCosts in Colorado.” 12 Patent protections, specialty drugs, and lack of pricetransparency appear to be fueling rising drug costs. The report makes bothstate and federal recommendations to achieve meaningful reductions in thetotal cost of prescription drugs for not only Medicaid and CHP , but also forColorado and Coloradans.Hospital delivery system: Colorado’s hospital prices are some of the highest in thecountry. While Colorado is fortunate to have a healthy population thatcontributes to lower per capita costs, the prices for individual procedures,inpatient care, and outpatient care are higher than the average in Coloradoand vary widely across hospitals. HCPF’s Colorado Hospital Cost Shift Analysis, 13published in January 2020, provides a thorough analysis of prices and profitsacross the hospital industry in Colorado and debunks the cost shift myth. HCPFalso provided insights into Colorado hospitals’ prices, costs and profits in apresentation and webinar in April 2021 and will release an updated HospitalPrices, Costs and Profits report in the Summer of 2021.Population Utilization Norms: Like most health plans, less than 5% of theMedicaid population have conditions that are driving more than 50% of theclaim expenses. 84% of HCBS members have a chronic condition, 31% of whomhave 5 or more chronic conditions. Having strong reporting insights to helpframe strategic solutions is critical as is managing complex claimants to securethe right care, at the right time, and the right price to address this 20Edition.pdf13 t-shift-analysis12
Demographics: Colorado’s growing and aging population will continue to increasecosts in HCPF programs. The State Demography Office predicts a totalpopulation growth of close to 480,000 people (7%) between 2020 and 2025. 14 Asthe population grows, Medicaid and CHP membership will also grow. Growthrates are even higher among older adults, with 13% growth of people betweenthe ages of 65-74, and 30% growth of people aged 75 and older. 15 By 2050, thepopulation of people 65 and older is estimated to more than double. As peopleage and spend down their resources, they become eligible for Medicaid.Further, people who require assistance with activities of daily living qualify forMedicaid at higher income levels.Long-Term Care Direct Care Workforce: HCPF currently serves nearly 70,000individuals who receive long-term services and supports. As the third fastestgrowing state in the nation for aging and older adults, this number is onlyexpected to grow larger in the coming years. Current workforce shortagesreflect challenges with recruiting and retention, with some providers reportingas high as 82% turnover, particularly in rural areas. COVID-19 has exacerbatedthe challenges associated with high burnout rates these workers on the frontlines of serving our most vulnerable Coloradans report high burnout nts-ofchange15 oloradocounties13
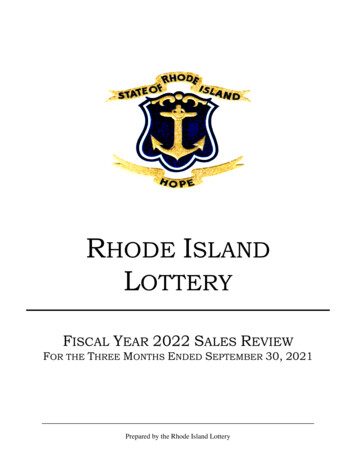
Fiscal Year 2020-2021, Q3: Performance EvaluationThere were two Wildly Important Goals (WIGs 16) in HCPF’s FY 2020-2021 performanceplan: 1) Access to Care and Customer Service, and 2) Medicaid Cost Control. Datafrom these measures is reported below and additional detail is available in the FY2020-21 Department Performance Plan. 17WIG 1, Q3: Access to Care and Customer ServiceThe economic downturn has caused an unprecedented number of Coloradans to losetheir employer-sponsored health coverage. HCPF saw a 19% increase in Coloradansreceiving services through Health First Colorado and CHP . Clearly, Coloradans needsupport through this challenging time. We have focused our WIGs on the areas thatare visible and meaningful to Coloradans, including enrollment support (call centerresponse and application processing time), member call center, provider call centerand payment turnaround time, provider recruitment and member access to providers,and connecting members who do not qualify for Health First Colorado or CHP toother coverage options through Connect for Health Colorado, the state’s insurancemarketplace.Successful completion of this goal will ensure Colorado’s most vulnerable residentsare able to get coverage in a timely manner, get their questions answered, and haveaccess to providers to meet their needs. Part of achieving this goal is also supportingour providers by answering their questions and paying claims in a timely manner. Q4results will be finalized in August 2021, and HCPF will meet or exceed these goals.16Learn more about Gov. Polis’ health care goals and priorities at ce/health17 cyfinancing14
WIG #1 Annual MeasureFY 20 YE FY 21 Q3 FY 21MayDeliver health care coverage, service and access to Coloradansduring this economic downturn. By June 30, 2021, out-performaverage monthly targets as measured by the number of newMedicaid providers, member application processing times, callcenter speed-of-answer time, provider payment turnaroundN/Atime, and timeliness of application referrals to Connect forHealth Colorado.FY 21GoalN/AN/A100%98.1%98.9%95%Q3 Evaluation: On track. Annual measure. Data to bereported at the end of FY.Process 95% of eligibility applications within 45 days throughJune 30, 2021.94.4%Q3 Evaluation: On track. March application processing rate is98.1% within 45 days.Answer calls at the provider call center, member call center,and enrollment call center in an average of less than 150seconds through June 30, 2021.32SecondsQ3 Evaluation: On track. Combined weighted average for allthree call centers is very favorable to goal.Enroll 10,000 new Health First Colorado providers by June 30,2021.9,549Q3 Evaluation: Currently on pace to exceed goal with anestimated 10,900 new providers enrolled by June 30, 2021.Pay 100% of Medicaid medical and pharmacy claims in anaverage of less than seven days through June 30, 2021.3.5 daysQ3 Evaluation: On track. Claims consistently process between3 and 4 days.Refer 90% of applicants determined not eligible for Health FirstColorado or CHP to Connect for Health Colorado within threedays of authorization date through June 30, 2021.N/A9247150Seconds Seconds Seconds8,10010,07810,000183.5 days 3.7 days 7 days99%99%90%Q3 Evaluation: On track. 99% of eligible applications arereferred within 3 days.18Starting point for FY21 goal is zero.15
WIG 2 Q3: Medicaid Cost ControlMedicaid cost control continues to be a high priority for HCPF and being an effectivesteward of Coloradans’ valuable financial resources remains paramount. Controllingcosts has been even more critical in the months and years ahead given the economicdownturn and the continued growth in Medicaid and CHP enrollment, which impactthe state budget (as described above). Successful completion of this goal ensureseffective stewardship of Colorado’s financial resources while maintaining ourcommitment to member access to care and health outcomes. For example, one of theleading indicators for this WIG is the implementation of condition management andcare support programs. Proactive engagement with our members who have complex,high cost health care needs, and conditions can improve outcomes and quality of lifefor these members while simultaneously lowering the cost to the state. Many of thesegoals were completed by Q3, and we are on track to meet or exceed the remainder ofour goals. All goals will be achieved.Medicaid Trend. The February 2020 to January 2021 Medicaid trend, compared to theprior 12-month period, is DOWN 3.0% PMPM (Gov’s WIG is PMPM trend increase 2%;includes claim payment runout). Risk-adjusted trend is up 1.4%. Paid trend is up 3.3%,which is low given membership is up 6.5% during the same period We havesignificantly outperformed this Medicaid cost control goal.16
WIG #2 Annual MeasureResponsibly manage health care costs to achieve an annualMedicaid trend19 of no more than 2.0% by June 30, 2021.Q3 Evaluation: Annual measure. Data to be reported after theend of FY. HCPF is on track to meet this measure.FY 20YEFY 21Q3FY 21MayFY 0%N/A100%100%100%100%100%100%Reduce Emergency Department visits per thousand members anaverage of 1.5% by June 30, 2021, by helping members maximizetelemedicine and the right settings for care.Q3 Evaluation: On track. Data for
resources to produce directional analyzes such as utilization, unit cost, quality, and overall cost trends for Health First Colorado, CHP , and other health care safety net programs administered by HCPF. The office oversees utilization review, population management, case and disease management, quality scorecard metrics, and cost