Transcription
WASH IN HEALTH CARE FACILITIESUNICEF Scoping Study in Eastern and Southern Africa1
WASH in Health Care FacilitiesUNICEF Scoping Study in Eastern and Southern AfricaAugust 2019 United Nations Children’s FundUNICEF Eastern and Southern Africa Regional Office (ESARO)Nairobi, KenyaAuthor: Magdalene Matthews Ofori-Kuma, UNICEF ESAROCo-Author: Tsion Gebreyesus, UNICEF Ethiopia Country OfficeCover Image: UNICEF/UN0318391/RamasomananaMother and newborn baby, Moramanga Hospital, MadagascarReviewers and Contributors: Samuel Godfrey, Bernard Keraita, Gabriele Fontana, Fatima Gohar, Lara Burger and Shem Okiomeri.The ESARO Team extends its gratitude to the governments, line ministries, technical resource persons and dedicated UNICEF WASH and healthcolleagues working to advance WASH in health care facilities in the 21 UNICEF programming countries in Eastern and Southern Africa Region fortheir valuable contributions, insights and inputs to the study.Special acknowledgements to the following UNICEF staff for their contributions of time, content, knowledge and experience to the enrichmentof the final publication:AngolaTomas Lopez de Bufala, Edson MonteiroBurundiDaniel Spalthoff, Yves Shaka, Remegie NzeyimanaComorosSylvain Bertrand, Maarouf MohamedEritreaDavid Tsetse, Hanna Berhe, Yirgalem SolomonEswatiniBoniswa DladlaEthiopiaKitka Goyal, Jane Bevan, Netsanet Kassa, Getachew HailemichaelKenyaAndrew Trevett, Maya Igarashi Wood, Agnes MakanyiLesothoNadia AlHarithi, Ubong Ekanem, Anthony AsijeMadagascarBrigitte Pedro, Bodovoahangy Andriamaroson, Tata Venance (Ministry of Public Health),Ranarison Volahanta Malala (WHO)MalawiMichele Paba, Blessius Tauzie, Chimwemwe NyimbaMozambiqueChris Cormency, Mayza Tricamegy, Jesus TrellesNamibiaMatheus ShuuyaRwandaCindy Kushner, Jean Marie Vianney RutagandaSomaliaMahboob Ahmed Bajwa, Charles MutaiSouth SudanVictor Kinyanjui, Robert Taban Lominsuk, Prakash Raj LamsalUgandaShiva Narain Singh, Mary NawembeUnited Republic of TanzaniaAmour Seleman, John Mfungo, Francis OdhiamboZambiaMurtaza Malik, Lavuun VerstraeteZimbabweAidan Cronin, Shelly Chitsungo, Moreblessing Munyaka, Jennifer Barak, Mitsuaki Hirai
WASH IN HEALTH CARE FACILITIESUNICEF Scoping Study in Eastern and Southern Africa
4 UNICEF/UN0306399/Abdul
Table of ContentsLIST OF FIGURES & TABLES VIABBREVIATIONS AND ACRONYMS VIIINTRODUCTION 11. WASH AND HEALTH: CURRENT CONTEXT 41.1 GLOBAL FRAMEWORK FOR WASH IN HEALTH CARE FACILITIES41.2 UNICEF’S VISION FOR WASH IN HEALTH CARE FACILITIES61.3 WASH IN HEALTH IN EASTERN AND SOUTHERN AFRICA82. WASH COVERAGE IN HEALTH FACILITIES 92.1 JOINT MONITORING PROGRAMME SERVICE LADDERS FOR WASH IN HEALTH92.2. GLOBAL BASELINE FOR WASH IN HEALTH CARE FACILITIES102.3 WASH IN HEALTH COVERAGE IN EASTERN AND SOUTHERN AFRICA123. THE ENABLING ENVIRONMENT FOR WASH IN HEALTH CARE FACILITIES IN EASTERN ANDSOUTHERN AFRICA 143.1 DEFINITION AND SCOPE 143.2 METHODOLOGY 153.2.1 REGIONAL SURVEY AND ANALYSIS 153.2.2 CASE STUDIES 163.3 SOURCES OF INFORMATION 173.4 SPECIAL ACKNOWLEDGEMENT 174. FINDINGS 204.1 REGIONAL ENABLING ENVIRONMENT FOR WINHCF IN ESAR204.2 SECTOR POLICY/STRATEGY 224.3 INSTITUTIONAL ARRANGEMENTS 244.4 SECTOR FINANCING 254.5 PLANNING, MONITORING AND REVIEW 274.6 BUILDING CAPACITY FOR WASH IN HEALTH CARE FACILITIES295. CROSS-CUTTING & EMERGING ISSUES 325.1 WASH AND MATERNAL, NEWBORN AND CHILD HEALTH (MNCH)325.2 GENDER INCLUSIVITY AND MENSTRUAL HEALTH AND HYGIENE325.3 DISABILITY INCLUSION IN WINHCF POLICY FRAMEWORKS335.4 ANTIMICROBIAL RESISTANCE 335.5 CLIMATE-RESILIENCE PROGRAMMING FOR WASH IN HEALTH CARE FACILITIES335.6 COUNTRY PERSPECTIVES 346. DESCRIPTIVE CASE STUDIES 35UGANDA 35KENYA 39ERITREA 427. RECOMMENDATIONS 45REFERENCES 48ANNEX 1: SUMMARY OF WHO PUBLICATIONS ON HEALTH CARE AND WASTE50ANNEX 2: SDG CORE QUESTIONS FOR MONITORING WINHCF52ANNEX 3: INDICATORS IN REGIONAL ENABLING ENVIRONMENT SURVEY53ANNEX 4: A CLOSER LOOK AT ETHIOPIA’S ENABLING ENVIRONMENT FOR WASH INHEALTH CARE FACILITIES 54ANNEX 5: STAKEHOLDER PERSPECTIVES ON BOTTLENECKS AND RECOMMENDED ACTIONSFOR WINHCF SCALE-UP 56ADDITIONAL WASH IN HEALTH CARE FACILITIES RESOURCES59v
List of Figures and TablesFigure 1: Map of the 21 Countries in Eastern and Southern AfricaFigure 2: Multiple benefits of adequate WASH in health care facilitiesFigure 3: WASH FIT five step process for improving facility-level WASH ServicessFigure 4: Causes of newborn deaths in the regionFigure 5: New JMP service ladders for global monitoring of WASH in health care facilitiesFigure 6: Water services in health care facilities by SDG regionFigure 7: Proportion of health care facilities in sub-Saharan Africa with basic water supplyFigure 8: Sanitation coverage in health facilities in select countries in ESARFigure 9: UNICEF’s Strategy for WASH (2016-2030): A SnapshotFigure 10: Water coverage in health facilities in selected countries in Eastern and Southern AfricaFigure 11: Sanitation coverage in health facilities in selected countries in Eastern and Southern AfricaFigure 12: UNICEF’s Strategy for WASH (2016-2030): A snapshotFigure 13: WASH sector-strengthening building blocks and expected resultsFigure 14: Regional WASH in health care facilities enabling environment scorecard for countries in ESARFigure 15: Regional enabling environment scorecard for WASH in health care facilitiesFigure 16: Map of country performance for overall enabling environment indicators for WinHCF in ESARFigure 17: Country performance for enabling environment indicators on sector policy and strategy in ESARFigure 18: Proportion of countries with policy instruments and frameworks addressing WinHCF in ESARFigure 19: Country performance for enabling environment indicators on institutional arrangements in ESARFigure 20: Country performance for enabling environment indicators on sector financing in ESARFigure 21: Country performance for enabling environment indicators on planning, monitoring and reviewFigure 22: Proportion of countries in ESAR with HMIS indicators on usage and functionality for WinHCFFigure 23: Country performance for enabling environment indicators on capacity development in ESARFigure 24: JMP service ladders for water services in health care facilities in UgandaFigure 25: KJMP service ladders for sanitation services in health care facilities in UgandaFigure 26: JMP service ladders for waste disposal in health care facilities in UgandaFigure 27: Kenya Essential Package for Health (KEPH) Health Service levels, Source: Kenya HRH StrategyFigure 28: JMP service ladders for water services in health care facilities in KenyaFigure 29: Country scores for enabling environment indicators for WASH in healthcare facilities in EritreaFigure 30: WHO/UNICEF practical steps to achieve universal access to quality careFigure 31: SDG core questions for monitoring 6363940424651Table 1: Essential Environmental Health Standards in Health Care Facilities5Table 2: Enabling environment survey response, score and colour-coding guideline16Table 3: Regional WinHCF Enabling Environment Scores by Sector Strengthening Building Blocks21Table 4: Uganda’s referral health care system based on level and services provided35vi
List of Abbreviations and AcronymsDHSDemographic and Health SurveyDHISDistrict Health Information SoftwareESAREastern and Southern Africa RegionESAROEastern and Southern Africa Regional OfficeHCWMHealthcare Waste ManagementHMISHealth Management Information SystemIPCInfection Prevention and ControlJMPJoint Monitoring ProgrammeMDGsMillennium Development GoalsMHHMenstrual Health and HygieneMICSMultiple Indicator Cluster SurveysM&EMonitoring and EvaluationMoHMinistry of HealthMoWMinistry of WaterO&MOperations & MaintenanceRORegional OfficeSDGsSustainable Development GoalsUNICEFUnited Nations Children’s FundWASHWater, Sanitation and HygieneWHOWorld Health OrganizationWinHCFWASH in Health Care Facilitiesvii
8 UNICEF/UN0306439/Abdul
INTRODUCTIONAvailability of sustainable water, sanitation andhygiene (WASH) services is essential to quality of careand infection prevention and control in health carefacilities. The linkage between safe water for hygieneand handwashing in health facilities and reductionin disease transmission has long been established inliterature. Given the importance of water availability andgood hygiene during childbirth in particular, WASH isconsidered both a precondition and an entry point forgood quality of care.According to the World Health Organization (WHO), oneof the leading global actors working to improve WASH inhealth care facilities, clean and safe healthcare facilities,equipped with adequate WASH services, can: a) increasedemand for and trust in services; b) reinforce the role ofhealthcare services and staff in setting societal hygienenorms; c) increase the motivation and retention of healthworkers; d) result in cost savings from infections averted;and e) lead to more efficient service delivery. SustainableDevelopment Goal (SDG) 3 (ensure healthy lives andpromote well-being) and SDG 6 (ensure availability andsustainable management of water and sanitation for all)reinforce the need to ensure safe management of waterand sanitation, reduction in maternal mortality, endingpreventable newborn deaths, and providing qualityuniversal health coverage.Despite the critical role that water, sanitation, hygiene,waste disposal and environmental cleaning services playin the continuum of healthcare, access to WASH servicesglobally remains alarmingly poor. The gaps in currentWASH services in health care facilities are significant.According to the 2019 Global Baseline Report on WASHin Health Care Facilities, one in four health care facilitieslacks basic water services, and 896 million people haveno water service at their health care facility. For children,this has far-reaching effects on their level of growth,development, morbidity and mortality, especially at thevery start of life.In recent times, several developments have helpedstrategically position WASH in health care facilities(WinHCF) as a priority on the global developmentalagenda. In March 2018, at the Launch of InternationalDecade for Action, 2018-2028, United Nations SecretaryGeneral Antonio Guterres issued a global call to actionfor WASH in all health facilities. Elevating WinHCF asa global issue, in his remarks, the Secretary Generalstated: “We must work to prevent the spread of disease.Improved water, sanitation and hygiene in healthfacilities is critical to this effort.”In April 2019, the WHO/UNICEF Joint MonitoringProgramme for Water Supply, Sanitation and Hygienepublished the Global Baseline Report on WASH in HealthCare Facilities, the first ever harmonized estimates forwater, sanitation, hand hygiene, health care wastemanagement and environmental cleaning services inhealth care facilities across the world. The report findingshelped raised further awareness on the magnitude ofthe problem on the global scale.Meanwhile, at the 72nd World Health Assembly inMay 2019, Ministers of Health from Member Statesunanimously approved a resolution on WASH in HealthCare Facilities, committing to advancing WinHCFprogramming through: a) the development of nationalroadmaps; b) the setting and monitoring of nationaltargets; c) increased investments in infrastructure andhuman resources; and d) targeted systems strengtheningto improve and sustain WASH services in health carefacilities.In response to these unfolding developments, WHO andUNICEF are co-leading global efforts on monitoring,standard setting, advocacy and learning. Under theSDGs, the global targets are to ensure that at least 50per cent of all health care facilities globally and in eachSDG region1 have basic WASH services by 2022, 80 percent by 2025, and 100 per cent by 2030. In countrieswhere WASH services exist, the target is advanced levelsof service, with the aim of 100 per cent by 2030. Asa children-focused organization, UNICEF is committedto helping every child gain access to drinking water,sanitation and hygiene, including in schools and healthcentres, and in emergency/humanitarian situationswhere children are most vulnerable. In the words ofUNICEF Executive Director Henrietta Fore: “Every birthshould be supported by a safe pair of hands, washedwith soap and water, using sterile equipment, in a cleanenvironment.”As part of UNICEF’s Global WASH Strategy (2016-2030),the organization will continue working with WHO andministries of health to formulate, promote and supportSDG Regions: a) Sub-Saharan Africa; b) Northern Africa and Western Asia; c) Central and Southern Asia; d) Eastern and South-Eastern Asia; e) Latin America and the Caribbean; f) Oceania;g) Europe and Northern America; h) Least Developed Countries (LDC); i) Landlocked developing countries (LLDC) and j) Small island developing States (SIDS).11
viable approaches for ensuring adequate WASH inhealth care facilities, with a focus on facilities providingmaternal and newborn health services. UNICEF’sinitiatives to improve water, sanitation and hygienepractices in health care facilities will focus on improvingthe safety and dignity of childbirth, with provisions madeto sponsor targeted research to improve the knowledgebase in the area for enhanced programme design andmore effective advocacy.On this premise, UNICEF Eastern and Southern AfricaRegional Office conducted a regional scoping studyand deep dive on the Enabling Environment forWASH services in Health Care Facilities across its 21programming countries in Eastern and Southern AfricaRegion. The aim was to assess the status of the enablingenvironment for WASH services in health facilities,identify related gaps and explore avenues to enhanceprogramming in the region. The objectives of the studywere:1. To assess the status of the enabling environment forWinHCFs programming in the region;2. To document best practices on WinHCFsprogramming from selected countries for furtherlearning, and knowledge-sharing in the region; and3. To increase awareness of WinHCFs programmingthrough evidence generation for enhancedprogramming and targeted advocacy.The study consisted of an online survey completedthrough multi-stakeholder consultations in countriesin the region, followed by visits to health care facilitiesin rural and urban settings in selected countries in the2region (Eritrea, Uganda and Kenya). Assessment wasbased on UNICEF’s Enabling Environment Framework,using the five sector strengthening building blocks: a)Sector policy/strategy; b) Institutional arrangements; c)Sector financing; d) Planning, monitoring and review;and e) Capacity development.The study forms part of evidence generation andknowledge sharing within the region and contributesto UNICEF’s global strategic focus (2016-2030) aswell as to the 2018-2021 Regional Priorities forEastern and Southern Africa Region which call for theinstitutionalization of WinHCFs programming, theprioritization of health facilities that provide maternal,neonatal and child health services; and the establishmentand enforcement of national standards for WASHservices in health care facilities.This report summarizes the findings of the study andconsists of five main parts:1. A literature review of the current global,organizational and regional frameworks for WinHCFprogramming;2. A summary of regional WASH coverage in healthcare facilities based on the 2019 Joint MonitoringProgramme global baseline findings;3. An analysis of the enabling environment for WinHCFderived from an administered online survey;4. Descriptive case studies of selected countries withinthe region; and5. Strategicrecommendationsforadvancingsustainable WinHCFs programming in the region.
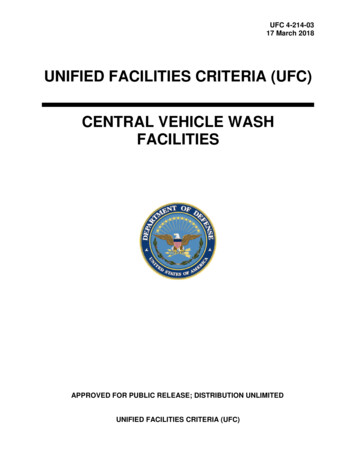
Figure 1: Map of the 21 Countries in Eastern and Southern Africa22Swaziland is the current Kingdom of Eswatini.3
Chapter 1WASH AND HEALTH: CURRENTCONTEXT1.1 GLOBAL FRAMEWORK FORWASH IN HEALTH CARE FACILITIESAs defined by the World Health Organization (WHO),3the term ‘health care facilities’ refers to “all formallyrecognized facilities that provide health care, includingprimary (health posts and clinics), secondary, andtertiary (district or national hospitals), public and private(including faith-run), and temporary structures designedfor emergency contexts (e.g., cholera treatmentcenters).” ‘WASH in health care facilities’ is defined as“the provision of water, sanitation, health care waste,hygiene and environmental cleaning infrastructure, andservices across all parts of a facility.” The organic roleWASH plays in ensuring quality of care, strengtheninginfection prevention and control, enhancing maternal,child and adolescent health and minimizing antimicrobialresistance cannot be overemphasized (Figure 2). Researchshows that the benefits extend far beyond the point ofcare to boosting staff morale and the performance ofhealth care workers, minimizing the national health careburden and providing a platform to promote improvedhygiene practices within the community.Figure 2: Multiple benefits of adequate WASH in health care facilities, Source: WHO/UNICEF Factsheet4Given the linkage between patient care service delivery and public health in any given context, several global guidancedocuments have been developed to help streamline quality of care within health facilities, including WASH servicedelivery. WHO and partners, including UNICEF, have, over the years, developed numerous frameworks to help reducethe disease burden caused by inadequate infection prevention and control (IPC) measures and poor health care wastemanagement (HCWM) through enhanced safety standards. Annex 1 provides a summary of publications addressingWASH, IPC and HCWM developed over the last decade and a half.53WHO WASH in Health Care Facilities, www.who.int/water sanitation health/facilities/healthcare/en/4WHO/UNICEF Global WinHCF Action Plan Factsheet, lobalActionPlanOct20151.pdf5WHO Publications, www.who.int/water sanitation n/4
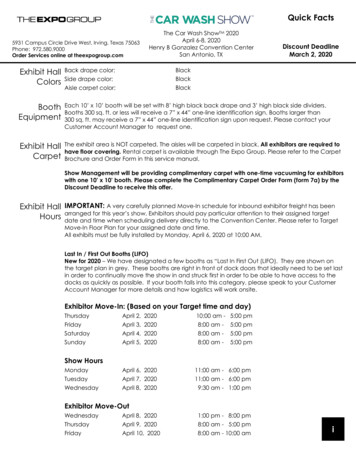
WHO Essential Environmental Health Standards in Health Care FacilitiesOne of the key guidance documents on WinHCF is the WHO Essential Environmental Health Standards in HealthCare Facilities. This was developed as guidance on essential environmental health standards required for health carein medium- and low-resource countries to guide the development and implementation of national policies. It lists therecommended minimum standards for water, sanitation and hygiene services in health facilities as 5–400 litres/person/day.Outpatient services require less water, while operatingtheatres and delivery rooms require more water. Theupper limit is for viral haemorrhagic fever (e.g. Ebola)isolation centres.Water accessOn-site supplies.Water should be available within all treatment wardsand in waiting areas.Water qualityLess than 1 Escherichia coli/ thermotoleranttotal coliforms per 100 ml.Presence of residual disinfectant.Water safety plans in place.Drinking water should comply with WHO Guidelinesfor Drinking-water Quality for microbial, chemicaland physical aspects. Facilities should adopt a riskmanagement approach to ensure that drinking water issafe.Sanitationquantity1 toilet for every 20 users for inpatient setting.At least 4 toilets per outpatient setting.Separate toilets for patients and staff.A sufficient number of toilets should be available forpatients, staff and visitors.SanitationaccessOn-site facilities.Sanitation facilities should be within the facility groundsand accessible to all types of users (females, males,those with disabilities).SanitationqualityAppropriate for local technical and financialconditions, safe, clean, accessible to all usersincluding those with reduced mobility.Toilets should be built according to technicalspecifications to ensure excreta are safely managed.HygieneA reliable water point with soap or alcohol-based hand rubs available in all treatmentareas, waiting rooms and near latrines forpatients and staff.Water and soap (or alcohol-based hand rubs) shouldavailable in all key areas of the facility for ensuring safehand hygiene practices.Table 1: Essential Environmental Health Standards in Health Care Facilities, Source: WHO6WHO/UNICEF Water Sanitation and Hygiene Facility Improvement Tool (WASH FIT)With several frameworks addressing different components of health care service delivery, to bridge the gap betweenenvironmental health, IPC and health care waste management at facility level, in 2018, WHO and UNICEF jointlypublished the Water and Sanitation for Health Facility Improvement Tool7 (WASH FIT) as a practical guide forimproving quality of care through WinHCF. WASH FIT is a risk-based approach for improving and sustaining water,sanitation and hygiene and health care waste management infrastructure and services in health care facilities in lowand middle-income countries (LMICs). It is designed as an improvement tool to be used on a continuous and regularbasis, to help HCF staff and administrators prioritize and improve services, and to inform broader district, regionaland national efforts to improve quality health care.WASH FIT guides multi-sectoral teams through a continuous cycle of assessing and prioritizing risks, defining andimplementing improvements, and continually monitoring progress. WASH FIT provides a systematic approach toimproving WASH through a health lens. According to WHO, since it was first developed in 2015, WASH FIT, as a tool,has been piloted in over 20 countries across the world.8 In eastern and southern Africa, Comoros, Ethiopia, Kenya,Madagascar, Malawi, Rwanda, Uganda and the United Republic of Tanzania have all piloted WASH FIT to some extentin health care facilities, making gains at facility level while learning implementation lessons along the way for furtherscale-up.WASH FIT implementation involves a five-step process beginning with the enabling environment and culminating inthe desired health-based objectives, thus emphasizing the role of the enabling environment as a starting point forsustainable WinHCFs (Figure 3). A strong enabling environment at national, sub-national and facility levels, is key to6WHO (2008), Essential Environmental Health Standards in Health Care Facilities, www.who.int/water sanitation health/publications/ehs hc/en/7WHO/UNICEF (2018), WASH FIT www.who.int/water sanitation h-facility-improvement-tool/en/According to WHO, countries in which WASHFIT has been piloted are Bangladesh, Bhutan, Cambodia, Chad, Comoros, the Democratic Republic of the Congo, Ethiopia, Ghana, Guinea, India,Indonesia, Iraq, Kenya, Lao People’s Democratic Republic, Liberia, Madagascar, Malawi, Mali, Nepal, the Philippines, Senegal, Tajikistan, the United Republic of Tanzania, Togo and Viet Nam.85
ENABLING ENVIRONMENTLeadership, political commitment and community engagement1. Assemble and trainthe WASH FITteam and holdregular meetings5. Continuouslyevaluate andimprove the plan4. Develop andimplement animprovement plan2. Conduct anassessment of thefacility3. Identify andprioritize areas forimprovementFigure 3. WASH FIT five-step processFigure3: WASH FIT five step process for improving facility-level WASH Services9every six months) visits to the facility by local or nationalSeveralother orglobalframeworksto WinHCFgovernmentsupportingpartnersspeakcan helpguide encourage facilities through the WASH FIT process. withmaternal,newbornchild forhealthThese visitsare also rlychildhooddevelopment(ECD).Theend goalevaluation of WASH FIT (see Practical Step 3,Liberiais caseto securea more profound impact on child healthstudy) (47).outcomes in the first 1,000 days of life.Every Newborn Action Plan (ENAP)WASH FIT trainingUnder the broader Every Woman, Every Child globalA set of trainingmodulesofis theavailableonlinein English,movementin rainingmodulesareprovided andGeneral’s Global Strategy for Women’s, Children’s,as a guide andHealthshould10beadapted to eryNewbornexampleswappingwith more ItrelevantexamplesActionPlan(ENAP)photoswas launched.calls fora reductionthe regionnewbornand ledeathswith guidancea focus onandhealth,whereand iestostandards,packagealsobeincludesequippedwith appropriateincludingan overviewof the WASH infrastructureFIT ilities,a module foreachsanitationof the nmentalwomen to giveHealthtoilets,Standards(e.g., water,spacessanitation,birthwith healthprivacy,dedicatedareasto managesickcleaning,careandwaste).Materialsfor runninganewbornssafely.11sample agendas, evaluation sheets, andtraining, includinga pre- and post-test quiz are also available. For technicalassistance or to share experiences of using the tool, pleaseand .intthe Nurturing CareFrameworkfor HelpingThe Nurturing Care FrameworkHuman Potential12 was developed. The Framework hasa special emphasis on early childhood development(ECD). To protect children’s health and support theirMobileapplicationdevelopment,it is essential that they have access toclean water and sanitation, good hygiene practices,A cleanmobileairapplicationof WASHFIT is availableand free Careand a safeenvironment.The NurturingtoFrameworkdownload (www.washfit.org).The applicationallows wholecalls for an integrated,multi-sectoral,facilityteams toapproachtrack moreand rapidly byandactionsfollow fromgovernmenttoeasilyECD supporteduptheon health,actions andgovernmentand partnersprovide childnutrition,education,social toprotection,real-timeIn addition,can be bour,it financeandbyWASHteamsto sharechallengesor careincludingtheapproachesavailabilityonof overcomingWASH servicesin healthengagein friendlycompetitions.facilitiesat the timeof birth and at community level formothers and newborns.Relatedreading: VISION FOR WASH IN1.2 UNICEF’SHEALTH CARE FACILITIESWater and Sanitation for Health Facility ImprovementToolFIT):A practicalguide(2016-2030)for improvingThe(WASHUNICEFWASHStrategyquality of care through water, sanitation and hygiene inThe UNICEFStrategyfor Water,Sanitationand Hygienehealthcare facilities[Internet].Geneva,World nkingOrganization and UNICEF, 2018 [cited 1 March lable from: http://www.who.int/water sanitation WASHin institutions – consisting of WASH in schools r-healthWASH in health care facilities (WinHCFs) and WASH infacility-improvement-tool/en/early childhood care centres – is one of the five strategicresults areas: 1) Water; 2) Sanitation; 3) Hygiene; 4)WASH in institutions; and 5) WASH in emergencies.Children Survive and Thrive to Transform Health and9WHO/UNICEF (2019), WASH in health care facilities: Practical steps to achieve universal access to quality care, www.who.int/water sanitation en/10The Global Strategy for Women’s, Children’s, and Adolescents’ Health, oads/2017/10/EWEC GSUpdate Brochure EN 2017 web.pdfEvery Newborn Action Plan, plan-(enap).pdf?sfvrsn 4d7b389 211Nurturing Care Framework (2018), 72603/9789241514064-eng.pdf12647PRACTICAL STEPS TO ACHIEVE UNIVERSAL ACCESS TO QUALITY CAREimproving the quality of care and internal IPC measuresin health facilities, and to promoting overall well-beingwithin a given context.ANNEX 3HEALTH-BASED OBJECTIVESMake improvements to meet accreditation scheme or national quality standards
To advance the global agenda on WinHCF programming,UNICEF commits to: Encouraging the institutionalization of WinHCFwithin the national health sector; Advocating for and supporting the inclusion ofWASH in health sector baseline studies and nationalsurveys; Supporting the development of national standardsfor WinHCFs and evidence-based models for scalingup with quality; while promoting cost-effectiveapproaches; and Encouraging the implementation of hygieneprotocols, including hygiene practices of healthworkers.The UNICEF Health Strategy (2016-2030)UNICEF’s Strategy for Health (2016-2030), in turn,stresses the importance of an integrated approachto early child health care, drawing on the diversity ofthe organization’s programmatic scope (nutrition,education, early childhood development (ECD), HIV,child protection, and WASH) and calls for nutritionscreening and intervention, improved community-levelhealth literacy, support to community-level interventionsrelated to early child development, and appropriatesupport to community-level and health facility WASHservices and practices.13Every Child AliveIn addition, as part of its efforts on reproductive,maternal, newborn, child and adolescent health(RMNCAH), UNICEF recently launched, Every Child Alive,a priority organizational integrated campaign aimed atsignificantly reducing morbidity and mortality at the verystart of life. Global statistics show that children face thehighest risk of dying in their first month of life. In 2016,there were 2.6 million newborn deaths, mostly withinthe first week. About 1 million died on
2.1 joint monitoring programme service ladders for wash in health 9 2.2. global baseline for wash in health care facilities 10 2.3 wash in health coverage in eastern and southern africa 12 3. the enabling environment for wash in health care facilities in eastern and southern africa 14