Transcription
ISVMA 2017November, 2017Canine SeizureManagement:Update on the ACVIMand IVETF ConsensusStatementsPanel MembersDr. Michael Podell (Chair)Affiliate Professor, U of Chicago,Pritzker School of Medicine ;Chicago Veterinary Specialty Group,USAMichael Podell MSc, DVM, Diplomate ACVIM (Neurology)MedVet Chicagompodell@medvetforpets.com773-281-7110Dr. Mette BerendtProfessorUniversity ofCopenhagen, DenmarkDr. Ned PattersonAssociate ProfessorUniversity ofMinnesota, USAInternational Veterinary Epilepsy Task ForceDr. Wolfgang LöscherProfessorUniversity of HannoverGermanyDr. Karen MuñanaProfessorNC State University,USADr. Simon PlattProfessorUniversity ofGeorgia, USADr. Holger VolkCo-ChairProfessorThe RoyalVeterinary College,London, UKBerendt et al. BMC Veterinary Research (2015) 11:182International veterinary epilepsy task force consensus report on epilepsy definition, classificationand terminology in companion animalsHülsmeyer et al. BMC Veterinary Research (2015) 11:175International Veterinary Epilepsy Task Force’s current understanding of idiopathicepilepsy of genetic or suspected genetic origin in purebred dogsRusbridge et al. BMC Veterinary Research (2015) 11:194International Veterinary Epilepsy Task Force recommendations for a veterinary epilepsy-specific MRIprotocolThe International Veterinary Epilepsy TaskForce (IVETF) isformed by a mondial (among others Europe, United Statesof America, Australia) group of (veterinary) scientistsinterested and specialised in the field of epilepsy. Ourgroup consists of clinical veterinary neurologists,neuropharmacologists, and veterinary l Approach Standardization of terminology Parallel work with InternationalVeterinary Epilepsy Task ForcePotschka et al. BMC Veterinary Research (2015) 11:177International veterinary epilepsy task force consensus proposal: outcome of therapeuticinterventions in canine and feline epilepsy Latin from consentire (to allow)ACVIM General agreement: unanimity The judgment arrived at by most of those concernedevaluation and recommendationveterinary clinical and humantranslation studiesBhatti et al. BMC Veterinary Research (2015) 11:176International Veterinary Epilepsy Task Force consensus proposal: medical treatment ofcanine epilepsy in EuropeCON-SEN-SUS Provide foundation of scientific Establish a framework forDe Risio et al. BMC Veterinary Research (2015) 11:148International veterinary epilepsy task force consensus proposal: diagnostic approach to epilepsy in dogsECVIMANDECVNDr Michael Podell MedVet ChicagoIVETF Group solidarity in sentiment and belief1
ISVMA 2017November, 2017Guidelines for the Diagnosis and Treatmentof Canine EpilepsyOur ApproachProblemsObjectivesprocess Incomplete diagnostic capabilities1.When should treatment be started?2.Which drug should be used first? Focus on epilepsy of undetermined3.How should AED monitoring be performed?4.What are the risks of treatment?5.What is drug-resistance?6.When and which second AED should be started?cause (idiopathic/genetic/primary) Chronic treatment only Wide-variability in treatmentapproaches Recommendations based on publishedreports and clinical expertise opinion Small database of strong evidence-based clinical studies Level OfEvidenceIBlinded, randomized clinical trials anddrug efficacy of 50% seizure reductionfor at 6 monthsIICase-control or cohort studies (N 15)Any peer-reviewed study without languagerestrictions in which an antiepileptic drugwas used and in dogs with epilepsy Proceedings Annual Congresses of the European Societyand College of Veterinary Neurology and theAmerican College of Veterinary InternalMedicineGrade Of RecommendationNon-blinded, randomized, or non-blindedand non-randomized clinical trials and/ordrug efficacy of 50% seizure reductionfor 12 weeksIIIIV Emergency treatment strategies (not included in this paper)Appropriately designed, controlled trialsIB Studies were included following modified Type Of EvidenceBlinded, randomized clinical trials anddrug efficacy of 50% seizure reductionfor at least 6 monthsPub Med (www.ncbi.nlm.nih.gov/PubMed)CAB Abstracts (www.cabdirect.org) and Webof Science (http://wok.mimas.ac.uk) searchstrategies included reference lists ofpublished papers and proceedingscriteria laid out in detail by Charalambouset al. 2014 Guidelines to enhance patient response and quality of lifelogical sequential approach to seizuremanagementestablished for people Standard electronic databases Complimentary and alternative treatment strategies Establish a predetermined, concise and Use of antiepileptic drugs (AED)Published evidence in the peer-reviewedliterature Decision making treatment strategiesstatement for canine seizuremanagement Unpredictable clinical outcomeMETHODOLOGY Seizure identification and diagnosis (not included in this paper) Present a working clinical consensus Epilepsy is a heterogeneous diseaseCase-control or cohort studies: (N 15)Non-blinded and non-randomized clinicaltrials with cohort size of less than 15and/or drug efficacy of 50% seizurereduction for 12 weeksExpert opinion only withoutdocumentation by case reports or seriesAHigh and likely tobe effectiveBModerate andlikely to beeffectiveCLow and may notbe effectiveDNotrecommended Allocation concealment Blinding of participants Personnel and outcome assessors Completeness of outcome data Selective reporting of outcome measures Other sources of biasCharalambous et al. Treatment incanine epilepsy- a systematicreview. BMC Veterinary Research,2014Levels of evidence and grades of recommendation. Table adapted from the NationalInstitute for Health and Care Excellence (NICE) guidelines (Eccles & Mason 2001)When Should Treatment Be Started? Decision to treat is a reflection of thetreatment goals: Reduce or eliminate epileptic events Reduce seizure severity Avoid adverse effects Reduce seizure-related mortality and morbidity Risk factors for seizure recurrence are notwell-established for dogs Seizure density is considered a strong riskfactor for seizure recurrence Packer et al. Clinical risk factors associated with AEDresponsiveness in canine epilepsy, 2014http://journals.plos.org/plosone/ Random sequence generationCochrane Risk ofBias AssessmentTool Guidelines for people to start AED: Diagnosis of current or previous definedcerebral lesions or trauma Presence of inter-ictal EEG epilepticdischarges (up to 90 % recurrence rate) History of marked post-ictal adverse effects First unprovoked, seizure for adult onset? Individual risk and quality of life assessment Recurrence risk 21-45% within first 2 years Immediate treatment improves seizure freeprediction by 50%American Academy of Neurology,Summary of Evidence – Based Guidelines, 2015Dr Michael Podell MedVet ChicagoACVIM Panel Recommendations:The Reasons to Start AED Therapy Identifiable structural lesion present or prior history of brain disease or injury Acute repetitive seizures / status epilepticus has occurred Ictal event 5 minutes or 3 or more generalized seizures occur within a 24 hour period or 2 or more seizures without completely regaining consciousness between seizures Two or more seizure events occur within a 6 month period Prolonged, severe, or unusual post-ictal periods occur IVETF : “The epileptic seizure frequency and/or duration is increasing and/orseizure severity is deteriorating over 3 inter-ictal periods”2
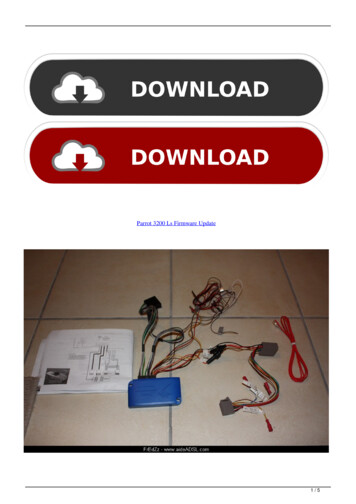
ISVMA 2017November, 2017Phenobarbital MonotherapyWhich AED Should Be Used First?HighRecommendation8 studies (n n Approved in USand Europe Approved inEuropeLevetiracetamZonisamide82% with 50%seizure reduction(N 255)ModerateTreatment Risk ofComplications6 studies:Duration of 5 to 32months5 studies (n 15)15% with noimprovement(N 47)Grade ofRecommendation ALevel Evidence I3% with 0 and 50% seizure reduction(N 9)Low Risk ofBiasHigher Risk of BiasModerateRisk of Bias 2 studiesHigh Risk ofBias 1 study 4 studies31% with seizurefree status (N 96)Cochrane Risk of Bias Assessment (Charalambous et al, 2014)Potassium Bromide MonotherapyPrimidone MonotherapyLevel Evidence I1 studyRISK OFBIAS6 months durationLow Risk ofBias74% with 50%seizure reductionModerate Riskof Bias 1 0Higher TreatmentRisk ofComplicationsHighLower Risk of Bias(n 1)High Risk ofBias 05 studies (n 15)38% with 50%seizure reduction(N 39)5 studies:Duration of 6 to 35months21% with noimprovement(N 22)41% with 0 and 50% seizure reduction(N 42)Low RiskLevel Evidence I38% with 50%seizure reduction(N 78)4 studies:Duration of 5 to 8 months2 % with noimprovement(N 3)60% with 0 and 50% seizurereduction(N 123*)Low TreatmentRisk ofComplicationsLow Risk ofBias 2 studies40% with seizurefree status (N 82)LevetiracetamMonotherapyHighRecommendation4 studies (n 205)2 studies (n 15)Grade ofRecommendation ALow to ModerateRisk of BiasHigh Risk of Bias 2 studies 0 studies* EstimatedCochrane Risk of Bias Assessment (Charalambous et al, 2014)Dr Michael Podell MedVet ChicagoLevel Evidence IV 3 studiesGrade ofRecommendation CInsufficient Data toRecommendLow TreatmentRisk ofComplicationsNo published reports evaluating theuse of levetiracetam as first linetherapy in dogs with epilepsyModerate Riskof BiasHigh Risk of Bias 3 studiesCochrane Risk of Bias Assessment (Charalambous et al, 2014)Cochrane Risk of Bias Assessment (Charalambous et al, 2014)Imepitoin MonotherapyHigher Risk ofBiasModerateRisk of Bias 0 studies35% with seizurefree status(N 36)16% with 0 and 50% seizure reductionGrade ofRecommendation DNot Recommended6 studies (n 103)ModerateRecommendationModerateTreatment Risk ofComplicationsN 23Level Evidence IIGrade ofRecommendation B (n 1)Low Risk 0 studiesUnknown Risk ofBiasModerate Riskof BiasHigh Risk of Bias 0 studies 0 studiesCochrane Risk of Bias Assessment (Charalambous et al, 2014)3
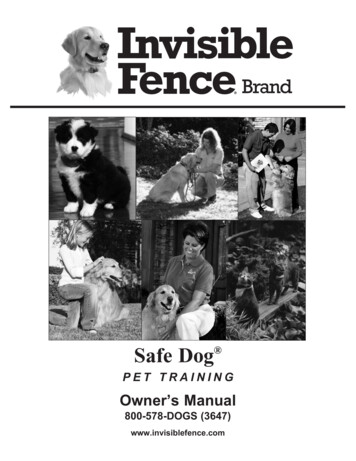
ISVMA 2017November, 2017Zonisamide MonotherapyLevel Evidence III60% with 50% seizurereduction (n 6)Duration of 12 to 36months40% with noimprovement(N 4)ACVIM Panel Monotherapy Recommendations:DRUGLEVEL OF EVIDENCEGRADE cient Data toRecommend1 study (n 10)0 studies (n 15)Grade ofRecommendation C0% with 0 and 50% seizurereduction0 % with seizurefree statusLow TreatmentRisk ofComplicationsLow Risk 0 studiesHigher Risk ofBiasModerateRisk of BiasHigh Risk of Bias 0 studies 1 studyCochrane Risk of Bias Assessment (Charalambous et al, 2014)ACVIM Panel Grade of Recommendations(Level of Evidence) for AED MonotherapyHow Should AED Monitoring Be Performed? Objectives Determine effective drug levels afterinitiation of successful therapy (asappropriate )A (HIGH) Phenobarbital(I) Imepitoin (I)B (MODERATE) Bromide (I)C (LOW)D (NO) Levetiracetam(IV) Zonisamide(III) Primidone (II) Determine if drug failure is due to: Pharmacokinetic factors to focus on a changein dose (metabolic tolerance) or Pharmacodynamic factors to focus on achange of drugs (functional tolerance) Determine if treatment failure is due toTOLERANCEpoor compliance, an inadequate or achange in drug levelDOSE Prevent toxic effects from occurring[SERUM] Aid with individualization of therapylaboratory /clinical study for apopulation Toxicity: Upper limit below which toxicresponse is likely Therapeutic range is the range of drugconcentrations associated with bestachievable results in an individual InitialFUNCTIONAL Elimination half-life of 24-40 hours Auto-induction of hepatic metabolism results in enhancedPhenobarbital Sub-therapeutic: Lower limit below whichtherapeutic response is unlikelyTIMEMETABOLIC PharmacologyDrug Monitoring Reference range is established byTIMEclearance over 6 weeks High degree of drug-drug interactions due to hepaticmetabolism and higher protein binding Panel recommendationsEvidence level: IGrade of Recommendationfor Monitoring: A Initial dose of 2.5 mg/kg q 12 hours Monitor levels at 2 and 6 weeks and every 6 months, 2 weeks after a dose change or with increase in seizure frequency Monitor if signs of toxicity Patient therapeutic range of 15-35 ug/ml Collect trough sample for dogs with recurrent seizures6 weeksStart Steady clearance Target2 weeks Steady stateDr Michael Podell MedVet Chicago4
ISVMA 2017November, 2017 Pharmacology Pharmacology Elimination half-life 15 -20 days Renal elimination No protein bindingPotassium BromideEvidence level: IGrade of Recommendation forMonitoring: A Rapidly metabolized to its major active metabolitephenobarbital that is responsible for more than 85% of thetotal anticonvulsant activity Panel recommendations : Initial dose or 30 to 40 mg/kg /day (single or divided) Monitor at 8 to 12 weeks after initiation and every 12monthsPrimidone Similar pharmacokinetic profile as phenobarbital Panel recommendations Initial dose of 10 mg/kg q 12 hours Monitor levels at 2 and 6 weeks and every 6 months, 1 month after a dose change, or if increase in seizure frequency Monitor if signs of toxicity Patient therapeutic range is 1000 to 3000 ug/ml formonotherapy and 800 to 2500 ug/ml for combined therapy Collect sample after 2 hours of dosing Avoid peak concentration 2 weeks after a dose change or with increase in seizureEvidence level: IGrade of Recommendation forMonitoring: Afrequency Monitor if signs of toxicity Patient therapeutic range of 15-35 ug/ml Collect trough sample for dogs with recurrent seizures6 to 12 monthsStart6 weeks Cumulative effectStart2 months2 weeks Steady state Steady state Pharmacology Pharmacology Elimination half-life Elimination half-life of approximately 2 hoursImepitoin Monotherapy: 4-8 hours No known therapeutic concentration Low inter-individual metabolism variabilityLevetiracetam No indication of drug-drug interactionEvidence level: IGrade of Recommendation: CApproved in Europe Steady clearance Panel recommendation:Evidence level: I Initial dose of 10-30 mg/kg q 12 hours Drug monitoring is not recommended except inGrade of Recommendationfor Monitoring: C With phenobarbital 2-4 hours Low hepatic metabolism Low drug-drug interaction Panel recommendations: Initial dose of 20 mg/kg q 8 hours Monitoring is not routinely recommended Monitoring may be indicated with concomitantrare cases of concern for owner compliancephenobarbital treatment if satisfactory seizurecontrol is not achieved. Trough and Peak levels are most helpful PharmacologyWhat Are The Risks Of Treatment? Elimination half-life of 15-20 hours Hepatic metabolism but without hepatic autoinduction Increased clearance with concomitant phenobarbital useZonisamide Weak carbonic anhydrase inhibitor Panel recommendations with the following criteria:related to pharmacological effectsin a dose dependent fashion Type 2: Unpredictable Initial dose Monotherapy: 5 mg/kg q 12 hours With phenobarbital : 10 mg/kg q 12 hoursEvidence level: IIGrade ofRecommendation forMonitoring: A Type 1: Predictable and directly Monitor levels at 2 weeks and then every 6 months, 2 weeks after a dose change or with increase in seizure frequency Collect trough time if used as monotherapy Collect trough and peak (3 hours) if used with phenobarbital Patient therapeutic range of 10-40 ug/mlStart6-12 weeks(idiosyncratic) and may be lifethreatening Type 3: Cumulative effects withEFFICACYTherapeutic IndexTOXICITYlonger term therapy and may belife-threatening Type 4: Delayed consequences(carcinogenic/teratogenic) andlife-threatening2 weeksDr Michael Podell MedVet Chicago5
ISVMA 2017November, 2017Type 1PhenobarbitalPotassiumbromideBehavioural changesType 2Type 3 Immune-mediated anemia,neutropenia or thrombocytopenia, Acute, idiosyncratic hepatotoxicreactions Superficial necrolytic dermatitis indogs Psychogenic polydipsia with associatedpolyuria Elevation of the serum alkaline phosphataselevel Factitious decrease in serum total and freethyroxine (T4) Drug-induced hepatotoxicity ( 35 ug/ml) Physical dependence and associatedwithdrawal effectsNot reportedPolydipsia and polyphagiaPelvic limb ataxia and weaknessAltered behaviourMegaesophagusCaution should be used when treating dogswith underlying renal insufficiencyNot reportedPancreatitis and gastrointestinalintoleranceIdiosyncratic allergic bronchitisPanniculitisType 4International League Against Epilepsy Task ForceKwan et al, Epilepsia 52:1069-1077, 2010Increased lethargy andmild ataxia withincreasing serumconcentration PrimidoneSimilar to PhenobarbitalSimilar to phenobarbital Higher prevalence of hepatotoxicity thanphenobarbitalNot reportedImepitoin Somnolence/sedation Polyphagia, polyuriaand polydipsia Hyperactivity AtaxiaNot reportedNone reportedImepitoin is notgenotoxic,teratogenic orimmune toxicLevetiracetamAtaxia only parameter todiffer from baselineNot reportedNot reportedNot reportedZonisamideSedation, ataxia andgastrointestinal upset KCSPolyarthropathyAcute toxic hepatic necrosisRenal tubular acidosis Lower total T4 levelsLower total C02What is Drug-Resistant Epilepsy?Drug Treatment Success Seizure free duration at least 3 timesthe longest seizure free period prior toonset of treatment Minimum duration of 12 months Undetermined outcome Inadequate time or drug dose Monotherapy failure Continued seizure recurrence despiteappropriate drug selection, time oftreatment and serum concentration Level 2 Failure of adequate trials of 2 toleratedand appropriately chosen AEDsNot reportedWhat Causes DrugResistance?Drug-Resistant Epilepsy Level 1When Should a Second AED Be Started? Transporter hypothesis (1) Reduced AED CSF concentration Strict criteria for decision-making strategy Target hypothesis (2) Decrease AED action at receptor Risk factors associated with pooreron starting a second AED is lacking inveterinary medicineseizure control include male dogs andprior cluster seizure activity Network hypothesis (3) Altered connectivity (Packer et al. 2014) Factors to consider Gene variant hypothesis Genetic protein alteration Selection of an AED with a differentmechanism of action Minimizing drug-drug interactions, avoiding Intrinsic severity hypothesis High seizure density and/orfrequency correlated with poorerprognosis Panel Recommendations: Documentation of appropriate drugand maximal level of first AED for aminimum of 3 months 50% increase in seizure frequencyover 3 months New onset of status epilepticus New onset of cluster seizures Presence of drug-toxicityadditive toxicity Determination of risk-benefit ofpolypharmacy versus quality of lifeKwan P et al. Drug-Resistant Epilepsy N Engl J Med 2011; 365:919-926Phenobarbital:Add-on TherapyLevel Evidence IVModerateRecommendation No reported studies evaluatingphenobarbital as an add-on AEDtreatment were found Recommendation is based onknowledge of efficacy asmonotherapy treatmentGrade ofRecommendation BModerateTreatment Risk ofComplicationsLow Risk ofBias 0 studiesHigher Risk of BiasModerate Riskof Bias 0 studiesHigh Risk ofBias 0 studiesCochrane Risk of Bias Assessment (Charalambous et al, 2014)Perucca et al Epil Beh, 2012Dr Michael Podell MedVet Chicago6
ISVMA 2017November, 2017Potassium Bromide: Add-on TherapyLevel Evidence II5 studies (n 232)All with phenobarbital orprimidone as primary AED4 studies (N 15)49% with 50%seizure reduction(N 114)ModerateRecommendationRISK OFBIASModerateTreatment Risk ofComplicationsAll studies 6monthsduration6 % with noimprovement(N 14)46% with 0 and 50% seizurereduction (N 118)*HighHigher Risk of BiasPrimidone:Add-on TherapyLevel Evidence IVphenobarbital as an add-onAED treatment were foundHigh TreatmentRisk ofComplicationsknowledge of efficacy asmonotherapy treatment 2 studiesLow Risk ofBiasHigh Risk ofBiasLevel Evidence III1 studyN 17 0 studies 3 studies35% with noimprovement(N 6)24% with 0 and 50% seizurereduction (N 4) 048% with 50%seizure reduction(n 34) 0Level Evidence III0 studies N 15)Low TreatmentRisk ofComplications3 studies 6 months(Duration of 4-18months )27 % with noimprovement(N 9)Grade ofRecommendation BModerateRecommendation3 studies (n 33)9 %with 0 and 50% seizurereduction (N 3)Low Risk 0 studiesModerateRisk of Bias 2 studiesModerate Risk ofBiasLow TreatmentRisk ofComplicationsLow RiskNOTE: 67% (6/9) increasefrequency 4-8 months(Volk et al, 2008)7 % with seizurefree status (N 5)Low Risk of Bias49% with 0 and 50% seizurereduction 1 studyNOTE: No statistical differencefrom placebo (Munana, et al 2012)Moderate Riskof BiasHigh Risk of Bias 1 study 1 studyCochrane Risk of Bias Assessment (Charalambous et al, 2014)ACVIM Panel Add-on Therapy Recommendations:DRUGLEVEL OF EVIDENCEGRADE h Risk of Bias 1 studyCochrane Risk of Bias Assessment (Charalambous et al, 2014)Dr Michael Podell MedVet Chicago3 % with noimprovement (N 2)Grade ofRecommendation BModerateRecommendationN 1 6 months(Duration of 9-95 months )High Risk ofBias 1Level Evidence IB3 studies (n 71)HighCochrane Risk of Bias Assessment (Charalambous et al, 2014)Zonisamide: Add-on TherapyLevetiracetam: Add-on TherapyHigher Risk of Bias(n 1)Moderate Riskof BiasLow Risk ofBiasCochrane Risk of Bias Assessment (Charalambous et al, 2014)2 studies (n 15)Low TreatmentRisk ofComplications6 months durationGrade ofRecommendation C (n 1)Insufficient Data forRecommendationRISK OFBIAS6% seizure free(N 1)24 % withseizure freestatus (N 8)High Risk ofBias 0 studies* EstimatedImepitoin: Add-On Therapy64% with 50%seizure reduction(n 21)Higher Risk of BiasModerate Riskof Bias 0 studiesCochrane Risk of Bias Assessment (Charalambous et al, 2014)41% with 50%seizure reduction(N 7)Grade ofRecommendation DNot recommended No reported studies evaluating Recommendation is based onModerate Riskof BiasLow Risk ofBias 0 studies6% seizurefree (N 10)Grade ofRecommendation B7
ISVMA 2017November, 2017ACVIM Panel Grade of Recommendations(Level of Evidence) for Add-On AED TherapyA (HIGH)B (MODERATE) Levetiracetam(IB) Bromide (II) Zonisamide(III) Phenobarbital(IV)C (LOW)FelbamateD (NO) Imepitoin (III)Additional AEDInformation forUse Primidone (II)Insufficient DataFor TreatmentRecommendationsGabapentin 2 clinical studies N 25 (III) 11/25 with 50% reduction for 3 or 4 monthsPregabalin 1 clinical study (n 9) (III) 7/9 with 50% reduction for 3 monthsTopiramateLacosamideRufinamideWhat AlternativeNon-PharmacologicalTreatments AreAvailable?Vagal NerveStimulation (VNS)Vagal NerveStimulation 1 clinical study (N 6) (III) 6/6 with 50% reduction for 6 months (CP seizures) 1 clinical study (n 10) (III) 5/10 dogs with 50% reduction for 6-15 months No clinical studies No clinical studies Placebo-controlled, cross-over study evaluating theuse of VNS in 10 dogs with medically refractoryidiopathic epilepsy (Muñana et al, 2002) Treatment and control periods were both 13 weeksin duration No significant difference seizure frequencybetween groups over the total study time periodHomeopathyComplimentaryand AlternativeMedicine Significant decrease in seizure frequency of 34%Dietwas detected with VNS for the final 4 weeks oftreatmentAcupunctureCourtesy of Dr. MunanaDietKetogenic (MCT)Level of evidence: IBInsufficient Data toRecommendRandomized placebo cross-over for6 months (N 11) Patterson et al, 2005 No difference in seizure control 3 cases pancreatitisFatty acidsupplementationHypoallergenicLevel of evidence: IBInsufficient Data toRecommendSingle blinded randomized,placebo cross over for 3 months(N 15) Matthews et al 2012 No difference in seizure controlRandomized, blinded placebo control for3 months (N 21) (Law et al. 2015) 7 with 50% improvementDr Michael Podell MedVet ChicagoLevel of evidence: IVInsufficient Data toRecommendOne retrospective non-controlledstudy (abstract N 8) with report ofimprovement (Luján et al, 2004)Eastern BasedAlternativeTherapyAcupuncture(Gold BeadImplantation)HomeopathyEvidence level IIIInsufficient Data forRecommendationEvidence level IIIInsufficient Data forRecommendationOverall decrease inmean seizurefrequency of 38.7%(N 15 with 7 on AED)for 15 weeks (Goiz-Belladonna /Cocculus 6C (N 10) forup to 8 months withvariable degree ofimprovement (Varshney,Marquez et al, 2009)2007)8
ISVMA 2017November, 2017What Are The Guidelines for Success And Quality of Life Parameters?Etiology Symptomatic Breed risksTreatmentTolerance Developed a working clinical consensus statement for canine seizure management Demonstrated that a collaborative international approach is achievableSeizure severityOwner Considerations Cluster Prolonged post-ictal Restrictive lifestyle Cost Emotional stress Family stressEfficacy Frequency NocturnalQualityof LifeWhat We AccomplishedClient Educationand SupportDr Michael Podell MedVet Chicago Established a predetermined, concise and logical sequential approach to seizuremanagement Established a framework for future veterinary clinical and translational epilepsy treatmentstudies Revealed a great need for controlled clinical trialsInternational Veterinary League Against Epilepsy ?9
Tool Random sequence generation Allocation concealment Blinding of participants Personnel and outcome assessors Completeness of outcome data Selective reporting of outcome measures Other sources of bias Charalambous et al. Treatment in canine epilepsy- a systematic review. BMC Veterinary Research, 2014 When Should Treatment Be Started?