Transcription
Using Screeners for Religious orSpiritual Struggle: Why, How, What?April 30, 2017National Association of CatholicChaplainsAnnual ConferencePatricia E Murphy, rscj, PhD, BCCPatricia Murphy@rush.eduRush University Medical CenterCaterina MakoSystem Director of Spiritual Care andPastoral EducationDiocese of Rockville CentreCatholic Health Service of Long Island
2Why?Spiritual Inquiry is thefoundation for: Guiding chaplain’s care Communicating withcolleagues Evaluating our careChaplainsHospital SystemHealth Care ColleaguesElectronic MedicalRecords
Vocabulary Spiritual Screen* – a few questions to elicit basicpreferences and any obvious distress that warrantsfollow up (minimal expertise & time required) Often completed at admission Triage level care Spiritual History – collecting the basicspiritual/religious story (medium expertise & timerequired) Can be completed by MD, RN, or other healthcareprofessional Common history tools include: FICA, HOPE, & SPIRIT* Spiritual screens, histories, and assessments were first defined and differentiatedfrom each other in 2004 by Massey, Fitchett, & Roberts.
Vocabulary Spiritual Assessment – detailed process of listening to,interpreting, and evaluating spiritual needs and resources(significant expertise & often more time required) Completed by a professional chaplain
5Screening, History Taking, AssessmentSpiritual Assessment (7 x 7)Belief and MeaningVocation and ObligationsExperience and EmotionsDoubt (Courage) and GrowthRitual and PracticeCommunityAuthority and GuidanceFitchett & Risk, 2009Fitchett, 1993
6Screening for Religious/Spiritual StruggleScreening for religious/spiritual struggle is anattempt to identify patients who may potentiallybe experiencing religious/spiritual struggle.Screening for religious/spiritual struggleemploys a few, simple, non-threateningquestions that can be asked by health carecolleagues.A positive screen for religious/spiritual struggletriggers a referral to the chaplain whoconducts a more thorough assessment andprovides care as indicated.
SPIRITUAL SCREENINGBrent Peery, DMin, BCCWith his permission
Memorial Hermann We assembled a task force of 5 chaplains fromthroughout our 14 hospital health system We conducted a thorough search of published researchliterature on spiritual screening models We consulted via phone and email with other chaplaincyleaders regarding best practices for screening We identified the Rush Protocol from Rush UniversityMedical Center in Chicago as the most researched andvalidated spiritual screening tool (2009. Fitchett and Risk)
Memorial Hermann We slightly modified the Rush Protocol to fit our contextand to facilitate its inclusion in the nurse admission historyin in our electronic medical record (EMR) software We sought feedback from bedside nurses and furtherrevised the process according to their feedback We received approval from the system CNO Council for itto be built into in the nurse admission history in the EMR We worked with the system informatics department tobuild the screening process into the EMR
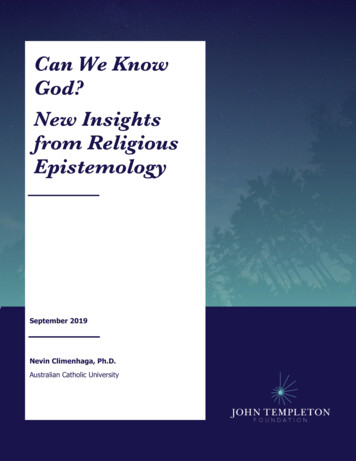
Introductory statement: Many patients and families have religious or spiritual beliefs that givethem strength, comfort, and contribute to health.1. As you cope with your condition/illness/injury, is religion or spirituality important to you?YESNO2. How much strength or comfortare you getting from yourreligion or spirituality?4. The chaplain may make rounds,would you like to request spiritual oremotional support from a chaplain?A) all that you need For A, go to Question 3YESNOB) less than you needC) none at all For either B or C, thankpatient. (automated chaplainreferral)3.Would you like to requestspiritual or emotional supportfrom a chaplain?YESNO(automated chaplainreferral)Continue nursingadmission history(automated chaplainreferral)Continue nursingadmission history
Memorial Hermann
Memorial Hermann
Memorial Hermann
Memorial Hermann
Memorial Hermann
Memorial Hermann An average increase in electronic chaplaincy referrals of109% One campus saw an increase of 151% An average increase in Press Ganey percentile rankingon “staff addressed spiritual needs” of 24 points Three campuses saw an increase of over 35 percentile points. 61% of patients/families screening for potential spiritual orreligious struggle were assessed to have spiritual orreligious struggle Eight chaplains participated in this research. There was widevariability in their data. At the extremes one chaplain found 92%screening accuracy and another found 36%.
17Another Screener
18Method Sample 57 patients with advanced cancer a prognosis of death in sixmonths. 84.2% were Christian Measures:1. What is spiritual pain to you?2. Are you experiencing spiritual pain right now?3. How would you rate the intensity of your pain? (0 to 10) Results Next Slide Significant correlation between spiritual pain and morphine intakeas well as between spiritual pain and depression. Religiosity not associated with spiritual pain.
19Another example of a Screener:Spiritual Pain Among Cancer PatientsA. Are you experiencing spiritual pain rightnow?61%“A pain deep in your being that is not physical.”B. What is spiritual pain to you?Focus of spiritual painPercent Associated Emotions48%Despair/resignation (40%)Isolation/abandonment (20%)Regret (10%)Anxiety (10%)38%Isolation (71%)Regret (24%)13%Resignation/despair (32%)Anxiety (28%)Isolation (8%)1. Intra-psychic(suffering with despair, loss, regret,anxiety)2. Interpersonal(unwanted by family, disconnected fromothers)3. Divine(abandonment by God, without faith orreligious/spiritual community)Mako et al, J Palliative Medicine, 2006
20Recent research with spiritual pain Patients at MDAnderson CancerCenter (N 292) To fill a void, thespiritual pain scale wasadded to a tool used tomeasure discomfort inpatients with cancer orchronic disease.
21Recent research with spiritual pain Results 44% had Spiritual pain at baseline and 57% at follow up. Those with fairly high levels of spiritual pain (4 or more) had higherlevels of most of the symptoms on the scale compared with thosewith no spiritual pain. When all the symptom items were used in a multiple correlationmodel with Spiritual Pain to find out which symptoms stood on theirown, higher levels of depression and financial distress wereassociated with higher levels of spiritual pain. Discussion This tool makes it possible to quickly identify those with spiritualpain. The tool that includes spiritual pain makes it possible to addressspiritual needs early in treatment.Delgado-Guay et al, 2016
22HOW GOOD IS ASCREENER?Patricia Murphy RSCJ, PhD, BCC and Stephen D.King, PhD, BCC
23Paper and Lead AuthorKing et al. (2017).“Determining bestmethods to screen forreligious/spiritualdistress”. SupportiveCare in Cancer, 25,471-475.Stephen D. King, PhD, BCCSeattle Cancer Care Alliance
24The Best Screener Identify close to 100% ofthose with struggle. I could do that by creating aquestion almost every onewould endorse. Example: Do you feel a littleless like yourself when you arein the hospital than when youare at home? A good screener does notcatch too many falsepositives – those who areidentified as having strugglewhen they really don’t. Whywould that matter in terms ofpastoral care?
25Steps in creating a Gold Standard A gold standard is assumed to be the best way tomeasure a construct – in our case, religious or spiritual(R/S) struggle; For a construct like depression, a diagnosis, based onsymptoms, done by a psychiatrist, is the gold standard forpaper and pencil instruments. To date, the gold standard for r/s struggle is KenPargament’s Negative Religious Coping Scale (NRC;Pargament, Koening, & Perez, 2000 ). In the future, what could be gold standard?
26Terminology for Evaluating a ScreenerThis is not something we talk about often!!!
27Terminology Sensitivity of a screenerSpecificity of a screener The ability to correctly identify The ability to correctly identifythose with struggle based on thescreener. Sensitivity is simply the rationumber detected by screenernumber detected by NRC The NRC is a little long so asimple screener is a good firststep. The desired ratio is at least 85%.only those with struggle basedon the screener. A screener might indicate r/sstruggle incorrectly. A chaplainneeds to assess patients whoscreen positive for struggle.Why is it a problem if some whoare positive on the screenerdon’t really have r/s struggle? The desired specificity is 85%.
28Methods Sample: 341 survivors of hematopoietic celltransplantation in the Northwest who were two years orless away from the transplant; Measures: NRCope with six other frequently usedscreeners; Choose a cut point of three (a little more complicated thanthat) for the NRCope rather than a total score of 1 or moreas an indication of struggle; Look for sensitivity and specificity of 85%.
29Negative Religious CopingScored 0 to 3 with 3 high1.2.3.4.5.6.7.I wondered whether God/Higher Power had abandonedme;I felt punished by God/Higher Power for my lack ofdevotion;I wondered what I did for God/Higher Power to punishme;I questioned God’s/Higher Power’s love for me;I wondered whether my church/faith community hadabandoned me;I decided the devil/an evil force made this happen;I questioned the power of God/ Higher Power.Pargament, Koening, & Perez, 2000
30Distribution for 341 Respondents Whohad their transplant 2 years ago or lessPossible responses:0 not at all1 somewhat2 quite a bit3 a great deal
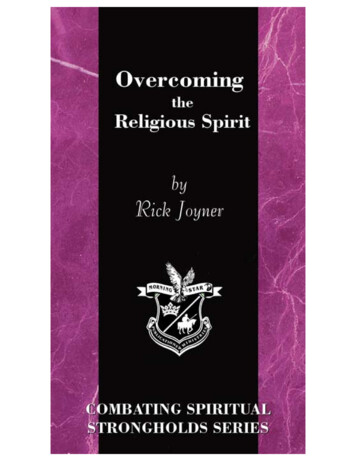
31Properties of Religious/Spiritual (R/S) ScreenersDo you struggle with the loss of meaning and joy in your life?Somewhat /Quite a bit/ a great dealNot at allDo you currently have what you would describe as religious orspiritual struggles?Somewhat/Quite a bit/great dealNot at allAre you at peace? (Steinhauser)Not at all/a little bit/ A moderate amountQuite a bit/ CompletelyRush ProtocolPotential struggleNo struggleDoes your religion/spirituality provide you all the strength andcomfort you need from it right now?Not at all/somewhatNot applicable /Quite a bit/ A great dealDo you have any spiritual/religious concerns? (NationalComprehensive Cancer Network )YesNoSensitivity Specificity65%58%61%75%55%80%31%90%43%85%25%87%
32Stuck at the CrossroadsOh no! None of thescreeners met our criteriaof 85%.It is a fair and a commonpractice to use twoscreeners at a time.Stephen King decided to dothat using the strongestscreeners.Because it was not in theoriginal plan, the methodwas a post hoc analysis. Itis not statistical cheating.
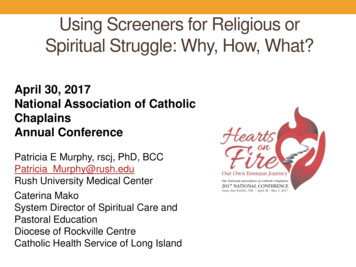
33Two Screening Items Used %47%Comfort/strength and Meaning/joy80%50%Peace and Self-described struggle83%60%Comfort/strength and Self-described struggle78%64%R/S concerns and Meaning/joy74%51%Comfort/strength and Peace74%68%R/S concerns and Self-described struggle71%65%Peace and R/S concerns66%70%Comfort/strength and R/S concerns57%74%ItemsLoss of Meaning/joy and Self-describedstrugglePeace and Meaning/joy
Summary Screening for struggle Can be done through a protocol suitable to EMR Is an important way to find those most in need of spiritual care Engages staff and increases referrals and improved scores on“staff addressed spiritual needs.” Indicates the level of prevalence and, therefore, staffing needs Chaplains might need better training to assess struggle To date, no screener meets the standard of 85%sensitivity Continue to work on screeners Determine the best Gold standard Consider using two screeners simultaneously
35Research on What Works Best A common screener for all chaplains that has the bestpsychometric properties? Continuing with chaplains’ intuitive approach that looks forstruggle? Get more chaplains Involved in simple research or screenerdevelopment? Including presence/absence of struggle in dropdown menu ofelectronic medical record? Rush Menu Patient seems to be coping well at present Patient doesn’t seem to be coping well at present Patient expressed feelings of guilt about lapse of religious practice
36A Little ConversationDo you screen for struggle?How do you screen?Are you likely to screen in the future?
37Publications about Spiritual AssessmentPubMed, 1015
Terminology Sensitivity of a screener The ability to correctly identify those with struggle based on the screener. Sensitivity is simply the ratio number detected by screener number detected by NRC The NRC is a little long so a simple screener is a good first step. The desired ratio is at least 85%. Specificity of a screener