Transcription
Assessment and Managementof FibromyalgiaFM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution
Program Discussion Points:1.2.3.4.Fibromyalgia (FM) ismanageable in the primarycare setting1,2Managing FM can be likemanaging other chronicconditions2Screening and diagnostictools are available to facilitateidentification of potential FMpatients3,4Effective managementintegrates multimodalnonpharmacologic andpharmacologic approaches2Brown TM, et al. Pain Week ’10, the Annual Meeting of the ASPE; September 8-11, 2010; Las Vegas, NV.McCarberg BH, et al, eds. Fibromyalgia. New York, NY: Informa Healthcare;2009:152-158. - 1-0FM-LYR-0023Arnold LM, et al. Mayo Clin Proc. 2011;86(5):457-464.ApprovedMcCarberg BH. Am J Therap. 2012;19(5):357–368.For your personal use. Not for further distribution2
Potential Benefits of AppropriateFibromyalgia ManagementGoals of FM management: Result in fewer visits to the healthcare provider(HCP) and has the potential to save money for theprimary care practice1 Streamline follow-up visits2 Empower patients to better manage their disease2,3 Improve patients’ functional ability2,3HCP healthcare provider.1. Brown TM, et al. Pain Week ’10, the Annual Meeting of the ASPE; September8-11, 2010; LasVegas, NV.FM-LYR-0023- 1-02. McCarberg BH, et al, eds. Fibromyalgia. New York, NY: Informa Healthcare; 2009:152-158.Approved3. McCarberg BH. Am J Therap. 2012;19(5):357–368.For your personal use. Not for further distribution3
Patients With FM Often Present and SeekOngoing Care in the Primary Care Setting1 Managing FM is similar to managing other complexchronic conditions (eg, asthma, diabetes) Key features of FM and other chronic conditions:––––There is no cureThe condition is associated with comorbiditiesThe condition affects many aspects of patients’ livesThe condition requires patient self-management Key features of disease management:– Pharmacologic therapy– Nonpharmacologic therapy– Patient self-management strategies and behaviorsFM-LYR-0023 - 1-0Approved1. McCarberg BH, et al, eds. Fibromyalgia. New York, NY: InformaHealthcare;2009:152-158.For yourpersonaluse. Not for further distribution4
A Chronic Disease Management Framework forManaging FM1Explain theConditionSet TreatmentGoalsApply MultimodalTherapyTrackProgress Integrate diseaseeducation withdiagnosis Assess symptomseverity Considerpharmacotherapyas appropriate Measureprogress againsttreatment goals Treat comorbidconditions Adjust treatmentplan accordingly Provide credibleinformationsources Prioritizefunctional areasand symptoms tobe treated Set expectationsfor patients1. Arnold LM, et al. Mayo Clin Proc. 2012;87(5):488-496. IncorporatenonpharmacologictherapiesFM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution5
What Are the Benefits of Engaging the Patientto Understand FM? Diagnosis and subsequent education sets thestage for effective management– Diagnosis provides validation, relief, andreassurance1 May improve certain outcomes2– Education provides empowerment, leading to betterself-management2,3 Setting basic expectations for you and your patientcan help establish a productive, more efficientpartnership, and may minimize frustration41.2.3.4.Sim J, Madden S. Soc Sci Med. 2008;67(1):57-67.Burckhardt CS. Disabil Rehabil. 2005;27(12):703-709.FM-LYR-0023 McCarberg BH, et al, eds. Fibromyalgia. New York, NY: Informa Healthcare; 2009:152-158.ApprovedPaiva ES, Jones KD. Best Pract Res Clin Rheumatol. 2010;24(3):341-352.1-0For your personal use. Not for further distribution6
Pain PathophysiologyFM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution7
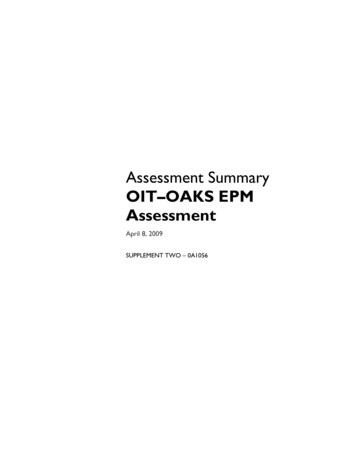
Chronic Pain Conditions Can Be ClassifiedBased on Type of Pain PathophysiologyThree Main Types of Pain oryHypersensitivityPain related todamage of somatic orvisceral tissue, due totrauma or inflammationPain related todamage of peripheralor central nervesPain without identifiablenerve or tissue damage;thought to result from persistentneuronal dysregulationEXAMPLES:painful diabetic peripheralneuropathy (pDPN),postherpetic neuralgiaEXAMPLES:rheumatoid arthritis,osteoarthritis, goutPhillips K, Clauw DF. Best Pract Res Clin Rheumatol. 2011;25(2):141-154.FM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distributionEXAMPLES:fibromyalgia
FM Is the Prototype"Sensory Hypersensitivity" Condition Patients with FM often exhibit1,2:– Pain in multiple body regions– Multiple somatic symptoms eg, fatigue, memory difficulties, sleep problems,disturbancemood– Higher current and lifetime history of chronic pain inseveral body regions– Family history of chronic pain– More sensitive to other sensory stimuli eg, bright light, loud noises, odors– Pain may be triggered or exacerbated by stressors– Generally normal physical examination except for diffuse tenderness andnonspecific neurologic signsFM-LYR-0023 - 1-01. Arnold LM, et al. Mayo Clin Proc. 2011;86(5):457-464.Approved2. Staud R, et al. Arthritis Research & Therapy. 2006;8(3):208.For your personal use. Not for further distribution9
Identifying the FM PatientFM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution10
Clinical Features of FMChronic Widespread Pain1 CORE criteria of FM Pain is in all 4 quadrants of the body 3 months Patient descriptors of pain include: Aching, exhausting, nagging, and hurtingTenderness2,3 Sensitivity to pressure stimuli Tender point exam given to assess tenderness Features of FM Hyperalgesia AllodyniaOther Symptoms3,4,5 Fatigue3 Pain-related conditions/symptoms Chronic headaches/migraines Subjective morning stiffnessOtherSymptoms Neurologic symptoms Subjective, tingling in extremities Sleep disturbances Non-restorative sleep, RLS1.2.3.4.5.Leavitt F, et al. Arthritis Rheum. 1986;29(6):775-781.Staud R. Arthritis Res Ther. 2006;8(3):208-214.Wolfe F, et al. Arthritis Rheum. 1995;38(1):19-28.FM-LYR-0023 - 1-0Yunus MB. Semin Arthritis Rheum. 2008;37(6):339-352.ApprovedVadivelu N, et al, eds. Essentials of Pain Management. ersonalNot forfurther distribution11
FM Often Seen With Other ChronicMedical Conditions Other Pain States1– IBS– Headaches/migraines Infection and Inflammation2– Crohn’s disease Psychological Disorders1– Depression– Anxiety disorders Rheumatic Disorders3– Rheumatoid arthritis– Systemic lupus erythematosusConsider FM in patients with chronic conditions who also suffer fromchronic widespread pain, fatigue, and sleep disturbances41.2.3.4.Chakrabarty S, Zoorob R. Am Fam Physician. 2007; 76(2):247-254.Hershfield NB. Can J Gastroenterol. 2005; 19(4):231-234.FM-LYR-0023 - 1-0Weir PT, et al. J Clin Rheumatol. 2006; 12(3):124-128.ApprovedMease P. J Rheumatol. 2005; 32 (suppl 75):6-21.For your personal use. Not for further distribution12
Screening Tools for IdentifyingPotential FM Patients Proper screening is a critical first step to managingfibromyalgia1– Several validated screening tools include: FibroDetect2 Fibromyalgia Survey Questionnaire (FSQ)3– ACR 2010 modified forpatient report London FM Epidemiology Study Screening Questionnaire (LFES-SQ)4These screening tools are provided to inform choice and theiruse is not prescriptive. They are not a clinical diagnosis, nor designed totake the place of a physician consultation.3,41.2.3.4.Arnold LM, et al. Mayo Clin Proc. 2011;86(5):457-464.Data on file. Pfizer Inc. FibroDetect; 2011.Wolfe, et al. J Rheumatol. 2011;38(6):1113-1122.White KP, et al. J Rheumatol.1999;26(4):880-884.FM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution13
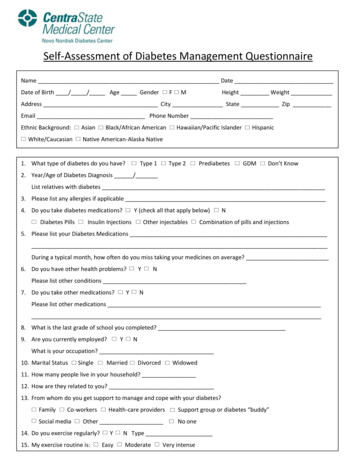
1990 American College of Rheumatology(ACR) Classification Criteria for Fibromyalgia1 The 1990 ACR criteria for theclassification of FM include:– Chronic widespread pain (core feature)for 3 months Pain above and below the waist Pain on left and right sides of body Pain in the axial skeleton– Pain at 11 of 18 tender points whenpalpated with 4 kg/cm2 of digital pressureDiagram Showing 18 Tender PointsThe 1990 ACR criteria are1: Sensitive (88.4%) – proportion of patients correctly identified as having the condition Specific (81.1%) – proportion of patients correctly identified as not having the conditionFM-LYR-0023 - 1-0Approved1. Wolfe F, et al. Arthritis Rheum. 1990;33(2):160-172.For your personal use. Not for further distribution14
2010 ACR Preliminary DiagnosticCriteria for FM1According to the 2010 ACR preliminary criteria, FM can bediagnosed based on a HCP-administered questionnaire:1. Widespread pain index (WPI)– The number of painful body regions2. Symptom severity (SS) scale that assesses the severity of:––––FatigueWaking unrefreshedCognitive symptomsQuantifies the occurrence of other somatic symptoms3. Pain and symptoms present for 3 months or longerThe 2010 preliminary ACR criteria1: Not meant to replace current ACR classification criteria, but to offer an alternative method of FM diagnosis Accurately identified 88% of the same FM cases initially identified by the 1990 ACR classification criteriaFM-LYR-0023 - 1-0Approved1. Wolfe F, et al. Arthritis Care Res. 2010;62(5):600-610.For your personal use. Not for further distribution15
ACR: Two Types of Classification andPreliminary Diagnosis Criteria for FM1990 ClassificationCriteria12010 PreliminaryDiagnostic Criteria2Consider pain to be acentral symptom of FMYesYesInclude assessment ofsymptoms other thanpain in diagnosisNoSpecify use of a tenderpoint examYesParameterAlthough definition of FM is broadened toinclude other symptomsYesSymptom Severity Scale assesses somaticsymptoms such as fatigue, sleep, cognitionNoHowever, a physical exam isrecommended for all patients A May 2010 article in Arthritis Care & Research proposed new criteria for the diagnosis of FM2 Among the objectives of the study was to identify non-tender point diagnostic criteria2 These criteria are not intended to replace the 1990 ACR Classification Criteria, but to represent analternative method of diagnosis21. Wolfe F, et al. Arthritis Rheum.1990;33(2):160-172.2. Wolfe F, et al. Arthritis Care Res. 2010; 62(5):600-610.FM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution16
Managing theFibromyalgia PatientFM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution17
Manage Expectations UpfrontExpectations Regardingthe Course of Disease Goal of treatment improvement in function andsymptoms (not cure)1 FM is dynamic, with potentialfor flare-ups and setbacks2Expectations Regardingthe Treatment Process Process of care utilizes acollaborative healthcareteam2– The patient is a criticalmember of this team Other expectations mayinclude:– Frequency of office visits– How much time will beavailable at each visit– Prioritization of goals– Position on disabilityFM-LYR-0023 - 1-01. McCarberg BH, et al, eds. Fibromyalgia. New York, NY: Informa Healthcare; 2009:152-158.Approved2. Arnold LM, et al. Mayo Clin Proc. 2012;87(5):488-496.For your personal use. Not for further distribution18
What Are the Benefits of SettingMeaningful Treatment Goals? Goal setting helps focus and streamline follow-up visits1,2– Provides a plan of action– Focuses the patient on targeted functional outcomes– Provides structure for follow-up visits Appropriate goals for FM asurableReflect the patient’s prioritiesHave a target date for completionAim for improved functionality in key domains Assess potential barriers and help the patientproblem-solve to minimize them41.2.3.4.McCarberg BH, et al, eds. Fibromyalgia. New York, NY: Informa Healthcare; 2009:152-158.Arnold LM, et al. Mayo Clin Proc. 2012;87(5):488-496.FM-LYR-0023 - 1-0Burckhardt CS. Disabil Rehabil. 2005;27(12):703-709.ApprovedFiloramo MA. Pain Manag Nurs. 2007;8(2):96-101.For your personal use. Not for further distribution19
Tools to Document Baseline Status andManage Treatment ProgressToolDescription Revised FibromyalgiaImpact Questionnaire(FIQR)1Modified Visual AnalogScale of theFibromyalgia ImpactQuestionnaire(mVASFIQ)2ACR 2010 PreliminaryDiagnostic Criteria3Numeric rating scale(NRS)4 21 questions to assess functional status and symptoms overprevious 7 daysCan be used to track specific functional domains or symptoms at initialassessment and at each visit thereafterPhysician or office staff administer, taking 2 minutes Quantifies the severity of individual FM symptomsProvides the basis for initial treatment planIdentifies most bothersome symptomsPatients can complete, taking 2 minutes Comprises widespread pain index (WPI) and2 symptom severity (SS) scalesProvides alternative FM diagnostic criteria to ACR Tender Point Exam;SS portion may be used to track progress over timeValid, reliable diagnostic tool; not yet validated for tracking progressPhysician or office staff administer Can be used to assess functional impact/symptom severityValues directly entered into patient’s chart or electronic medical recordPatient can complete, taking 2 minutes 1. Bennett RM, et al. Arthritis Res Ther. 2009;11(4):R120.FM-LYR-0023 - 1-02. Boomershine CS, Crofford LJ. Nat Rev Rheumatol. 2009;5(4):191-199.Approved 4. Johnson C. J Chiropr Med. 2005;4(1):43-44.3. Wolfe F, et al. Arthritis Care Res. 2010;62(5):600-610.For your personal use. Not for further distribution20
The Multimodal ApproachFM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribution21
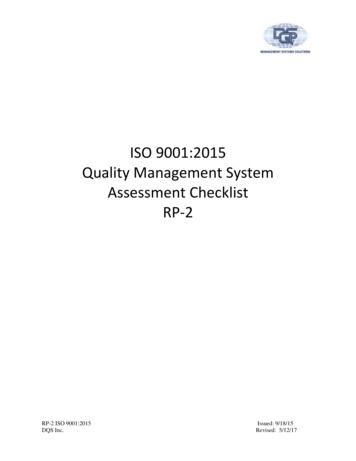
Why Apply Multimodal Therapy?Mood disturbance1Sleep disturbance1No single treatmentapproach for FMtargets every symptom;a multimodal treatmentapproach can enhancecare and maximizeresults2Chronic widespreadpain and tenderness1Morning stiffness1Fatigue11. Arnold LM, et al. Mayo Clin Proc. 2011;86(5):457-464.2. Mease P. J Rheumatol. 2005;32(suppl 75):6-21.FM-LYR-0023 - 1-0ApprovedFor your personal use. Not for further distribut
fibromyalgia1 – Several validated screening tools include: FibroDetect2 Fibromyalgia Survey Questionnaire (FSQ)3–ACR 2010 modified for patient report London FM Epidemiology Study Screening Questionnaire (LFES-SQ)4 These screening tools are provided to inform choice and their use is not prescriptive. They are not a clinical diagnosis, nor designed to