Transcription
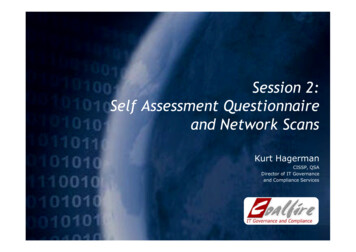
Self-Assessment of Diabetes Management QuestionnaireName DateDate of Birth / / Age GenderFMHeight WeightAddress City State ZipEmail Phone NumberEthnic Background:White/CaucasianAsianBlack/African AmericanHawaiian/Pacific IslanderHispanicNative American-Alaska Native1. What type of diabetes do you have?Type 1Type 2PrediabetesGDMDon’t Know2. Year/Age of Diabetes Diagnosis /List relatives with diabetes3. Please list any allergies if applicable4. Do you take diabetes medications?Diabetes PillsY (check all that apply below)Insulin InjectionsOther injectablesNCombination of pills and injections5. Please list your Diabetes MedicationsDuring a typical month, how often do you miss taking your medicines on average?6. Do you have other health problems?YNPlease list other conditions7. Do you take other medications?YNPlease list other medications8. What is the last grade of school you completed?9. Are you currently employed?YNWhat is your occupation?10. Marital StatusSingleMarriedDivorcedWidowed11. How many people live in your household?12. How are they related to you?13. From whom do you get support to manage and cope with your diabetes?FamilyCo-workersSocial mediaHealth-care providersOther14. Do you exercise regularly?15. My exercise routine is:YEasySupport group or diabetes “buddy”No oneN TypeModerateVery intense
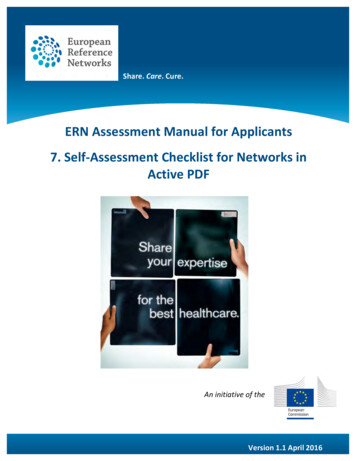
16. Do you use any particular guidelines for a specific meal plan?YNIf yes, please describe:About how often do you use this meal plan?Do you read and use food N17. Do you have any dietary restrictions?SaltNeverYNNoneOtherGive a sample of your meals for a typical day:Time: Breakfast:Time: Lunch:Time: Dinner:Time: Snack:Time: Snack:18. Do you do your own food shopping?19. Do you drink alcohol?How many:YYNN Type:Per day Per week OccasionallyDo you use tobacco:Cigarette20. Do you check your blood sugars?PipeYCigarChewingNoneQuit—how long agoNTypical or usual blood sugar range: toHow often:When:Once a dayBefore meals2 or more/day2 hours after meals1 or more/weekOccasionallyBefore bedtimeWhat is your target blood sugar range? toHow would you describe your usual results over the past month?21. In the last month, how often have you had a low blood sugar reaction?NeverOnceMultiple times/weekWhat are your symptoms?How do you treat your low blood sugar?22. Can you tell when your blood sugar is too high?YN23. What do you do when your blood sugar is high?
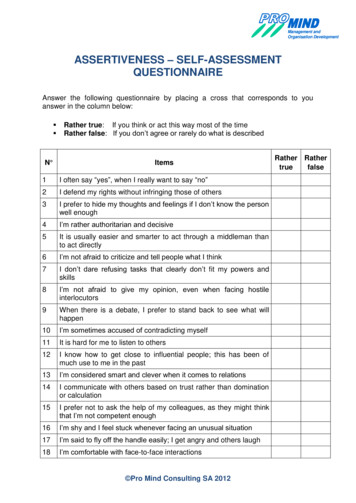
24. Check any of the following tests/procedures you have had in the last 12 months:Dilated eye examUrine test for proteinFoot exam—health care professionalFlu ShotDental examBlood pressureFoot exam—selfWeightCholesterolA1cPneumonia shot25. In the last 12 months, have you:Gone to the emergency room (ER)Was the ER visit or hospital admission diabetes-related?26. Do you have any of the following:Eye problemsYBeen admitted to a hospitalNKidney problemsNumbness/tingling/loss of feeling in your feetDental problemsHigh cholesterolSexual problemsHigh blood pressureDepression27. Have you had previous instruction or ever had anyone teach you about caring for your diabetes?YNHow long ago:28. In your own words, what is diabetes?29. How do you learn best?Listening30. Do you have any difficulty kingExplain any checked:31. Do you have any special cultural or religious observances, practices, or beliefs that influence how you care for yourdiabetes?YNPlease describe:32. Do you use computers to:EmailLook for health and other information33. Please state whether you agree, are neutral, or disagree with the following statements:I feel good about my general health:AgreeNeutralMy diabetes interferes with other aspects of my life:My overall level of stress is high:AgreeNeutralI often feel as if I am failing in managing my NeutralI often feel overwhelmed by the demands of living with diabetes:I feel I will get long-term complications, no matter what I e34. How do you handle the stress in your life? What are your feelings about diabetes?
35. What concerns you most about your diabetes?36. What is hardest for you in caring for your diabetes?37. What are your thoughts or feelings about this issue (e.g. frustrated, angry, guilty)?38. What are you most interested in learning from these diabetes education sessions?Pregnancy and FertilityAre you:Pre-MenopausalAre you pregnant?MenopausalPost-MenopausalN/AY—When are you expectingN—Are you planning on becoming pregnant?Have you been pregnant before?Do you have any children?YNY—AgesNAre you aware of the impact of diabetes on pregnancy?Are you using birth control?YNY—Please specifyN*Please do not write below this line*Educator Assessment Summary:Education Need/Education Plan:Medication UseMonitoringBehavior-Change StrategiesDiabetes Disease ProcessAcute ComplicationsNutritional ManagementPsychological AdjustmentPhysical ActivityChronic ComplicationsHealth PromotionDate: Educator Signature:Date: Educator Signature:
Welcome to the Novo Nordisk Diabetes Center at CentraState Medical Center. We are pleasedyou are taking the most important step toward the self-management of your diabetes. Ourprogram is designed to equip you with the tools and information that will lead to health andlifestyle improvements.If you are unable to keep your appointment, please call 24 hours in advancePlease arrive 15 minutes before the appointed time to allow for registration.We are located in the Star and Barry Tobias Ambulatory Campus. We offer free ValetParking, Monday through Friday, between 8 am and 4 pm. Parking is also available in theNorth Parking Lot.Bring the following checked items with you for your appointment: Your blood glucose meter and all related supplies. (Important) Your prescription for the program visit(s). It must have a diagnosis code onit (for insurance coverage). WE CANNOT SEE YOU WITHOUT A PRESCRIPTION. Identification, primary and secondary insurance cards Completed assessment forms The results of your latest blood work from the physicianPLEASE CALL INSURANCE COMPANY TO VERIFY COVERAGE PRIOR TO YOUR FIRST VISITWhat you need to know from your insurance company: How many visits they allow Deductibles, co-insurance and co-pays. We bill as a hospital outpatient facility, not asan office visit. Ask how this will affect the amount of your co-pay and if you are subjectto a deductible. A reference number and the name of the person that you spoke withCentraState Medical Center (not Novo Nordisk Diabetes Center)Tax ID number:221750190NPI number:1295718450Procedure codes:G0108 (assessment) and G0109 (classes)97802 (medical nutrition therapy, initial)97803 (medical nutrition therapy,Re-assessment)If you have any questions, please contact us at 732-294-2574.
35. What concerns you most about your diabetes? _ _ 36. What is hardest for you in caring for your diabetes? _ _ 37. What are your thoughts or feelings about this issue (e.g. frustrated, angry, guilty)? _ 38. What are you most interested in learning from these diabetes education sessions? _ _