Transcription
Gaps In Successful EHRImplementations: The Challenges &Successes Of Providers In TheMarketplace#OMTechnologyJanuary 31st, 2017 at 2:00 PM ETMatthew Dorman, Chief Executive Officer, Credible Behavioral Health SoftwareJoseph P. Naughton-Travers, Senior Associate, OPEN MINDSSponsored Bywww.openminds.com163 York Street, Gettysburg, Pennsylvania 17325Phone: 717-334-1329 - Email: info@openminds.com1 2016. All Rights Reserved.
Agenda2I.2016 Survey Results On Behavioral HealthEHR ImplementationsII.Key Elements Of An EHR ImplementationIII.Seven Steps To Effective EHR ImplementationIV.Questions & Discussion 2016. All Rights Reserved.
The Big Picture On Behavioral HealthEHR Implementations3The GoodThe BadThe Ugly There is consensus amongbehavioral health providersthat implementation of anelectronic health record(EHR) system brings valuewhen things go right The majority of providersreport implementing an EHRin 6-12 months Challenges include lack ofinvolvement from executiveleadership, staff engagement,poor planning and projectmanagement, and failure toidentify and fully implementthe key components of theEHR system 10% reportingimplementations of two yearsor longer! 2016. All Rights Reserved.
2016 Survey Results OnBehavioral Health EHRImplementations4
2016 Behavioral Health EHR SurveyA 2016 survey of behavioral health organizations was conducted to study theirexperiences in implementing an EHR system. This survey identified areaswhere typical EHR implementations fall short and the greatest challengesorganizations face during their EHR implementation process.The survey distributed via e-mail to over 5,000 behavioral health organizationsover the course of three months on three separate dates. One follow-up callwas conducted for each unique contact for all organizations solicited.There was a 13% completion rate.5 2016. All Rights Reserved.
Key Findings126 80% of the providers surveyed have purchased an EHR 69% of providers with an EHR define their EHR as fully implemented, with mosthaving implemented their system in 6-12 months3 25% of those with incomplete implementation attribute the delay due to theEHR vendor, and 30% report that it was a combination of delays from thevendor and their own organization4 When implementation was not fully complete, the scheduling and billingmodules were the major functionalities reported as being fully implementedwith the clinical and reporting modules incomplete 2016. All Rights Reserved.
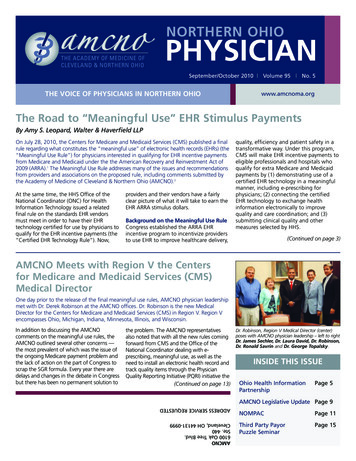
69% Of Providers Report Their EHR IsFully Implemented6%Fully implementedPartially implementedNot yet implemented25%69%7 2016. All Rights Reserved.
Top Reasons Organizations Have NotPurchased An EHR32%41%Too expensiveLimited TimeNo NeedOther2%8 2016. All Rights Reserved.25%
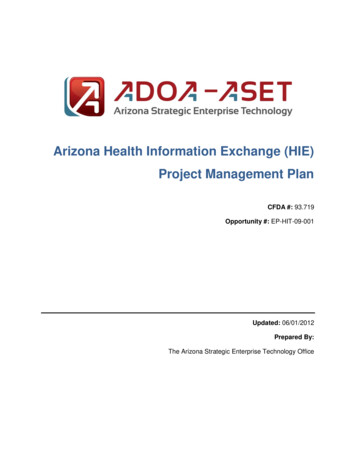
Overall EHR Implementation & Timelines80% of behavioral healthorganizations have purchased anEHR system already Of those who have not, 63% give thereasons as either that EHR systems areseen as too expensive or not neededThere is considerable variance inimplementation timelines withthe largest group (35%)implementing in 6-12 months More than one out of ten providers(12%) reported implementations of twoyears or longerKeep in mind when looking at the data that respondents are describingbased on their own definitions of the implementation completion andwhether or not they consider the EHR to be “fully implemented.” Thedata about core functionality that follows illustrates a slightly differentpicture.9 2016. All Rights Reserved.
The Time It Took To Fully Implement TheEHR (From Contract Execution To Go Live)12%27%7%0-6 months6-12 months12-18 months18-24 months19%24 months35%10 2016. All Rights Reserved.
EHR Implementation Delay Factors25% Twenty-five percent (25%) of providersreport the delays as being due to the EHRvendor, with another 25% attributing it totheir own internal challenges. Additionally one out of five providersreported that the delay was due to otheragency initiatives taking priority over theEHR implementation project itself.The fact that more than half of providers attribute the delayspartially or fully due to problems on the EHR vendor side highlightsthe need to choose the right EHR vendor partner, andthe importance of thorough research of EHR vendors’ experience andsuccess in doing implementations.11 2016. All Rights Reserved.
Top Reasons Organizations Report Their EHR IsNot Fully Implemented20%25%Delays from our internalorganizationDelay from our EHR vendorBoth delays from our internalorganization and from our EHRvendorOther agency initiatives havetaken priority30%25%12 2016. All Rights Reserved.
The Four Core EHR g 2016. All Rights Reserved.
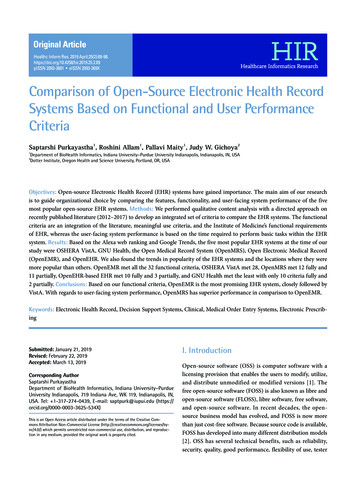
Core EHR Functionality Not Fully ImplementedIn the survey, the four corefunctionalities of an EHRsystem were defined asclinical, scheduling, billing,and reporting — all of whichare necessary to remaincompetitive in the changinghealth and human serviceslandscape.Yet, only 31% of providersindicated that all four of thecritical areas of functionalitywere fully implemented.Note that this finding differs from the previous finding where 69% reportedthat their EHR system was fully functional.14 2016. All Rights Reserved.
Core EHR Functionality Not Fully ImplementedScheduling and billingfunctionality have beenprioritized or moresuccessfully implemented byproviders Scheduling Billing15 ManagementReporting 2016. All Rights Reserved.While the criticalfunctionality of managementreporting is only reported asfully functional in just overone out of five providers.More than a quarter ofproviders reported that oneor more of these corefunctional areas is plannedfor implementation, but notcompleted yet.
Core Functionality Implementation16Core lyImplementedPlanned, butnotimplementedNot planned,but ing34%29%31%6%Reporting21%48%26%5% 2016. All Rights Reserved.
Key Elements Of AnEHR Implementation
EHR Implementation18I. RoutineElementsII. Complex #1 Vendortraining andimplementation #2 Hardware #3 Dataconversion #4 Mobilesystem use #5 Workflows #6 Clinicalcontent #7 System setup #8 Billing testing #9 Reports #10 Interfaces #11 Meaningfuluse 2016. All Rights Reserved.ElementsIII. SystemFreeze &FinalPreparationIV. Expanding &Leveraging TheEHRImplementation #12 Finalworkflow testing #13 Trainingmaterials andexecution #14 Final go-livepreparation #15 Implementingmore features #16 Leveraging datathrough businessintelligence #17 Additional clinicaland analytic use
EHR ImplementationI. Routine Elements #1 Vendor trainingand implementation #2 Hardware #3 Data conversion #4 Mobile system use19 2016. All Rights Reserved.
#1 Vendor Training & Implementation DaysThis includes all of the training and support from you vendor partner - these itemsare often included in the vendor’s standard project management templateThe number of training andimplementation support days andthe vendor’s approach varysignificantly from vendor to vendor20 2016. All Rights Reserved.
#2 Hardware & Infrastructure ChangesThis is for all tasks related tomaking sure that ourhardware and infrastructureis configured correctly andworks for implementing thenew system21 2016. All Rights Reserved.Also includes making allrequired hardware andsoftware purchases
#2 Hardware & Infrastructure Changes Checklist File servers and related infrastructure Connectivity and internet access Wireless cards or mobile hotspots Laptops and other portable devices Signature pads High-speed scanners Portable printers Kiosks Other?22 2016. All Rights Reserved.
#3 Data ConversionThis is for all tasks related to planning and executing a conversion of data fromthe old software package to the new oneKey decisions: What data elements to convert from theold system to the new one Which consumers to include in the dataconversion23 2016. All Rights Reserved.
#4 Mobile System Use PlanningThis is for testing and planning the use of the EHR in community or home-basedsettingsVendors may offer connected and/ordisconnected mobile EHR solutions, each ofwhich should be tested thoroughly, using allrelated equipment (such as signature pads,portable printers and scanners, etc.)24 2016. All Rights Reserved.
EHR ImplementationII. ComplexElements 25 2016. All Rights Reserved.#5 Workflows#6 Clinical content#7 System set-up#8 Billing testing#9 Reports#10 Interfaces#11 Meaningful use
#5 Workflow Process MappingThis is for all tasks related todoing the workflow reviewsand documentation (typicallywith VISEO software),identifying opportunities forimprovement, and modifyingthem to represent how thingswill work in the new system26 2016. All Rights Reserved.
Purpose Of Mapping Clinical & AdministrativeWorkflow ProcessesTo record all key tasks, steps, and decision points in current workflow processesTo understand what staff positions are used for each task or stepTo understand the consumer’s experience in the clinical workflow processes– the interfaces with staff and ease in moving through the system of careTo identify differences in workflows for similar clinical programs or administrativeprocesses27 2016. All Rights Reserved.
Purpose Of Workflow MappingTo identify opportunities to enhance and standardizeworkflows – to improve the experience of consumers, toincrease efficiencies, and to adopt both clinical andadministrative best practicesTo identify all health record data (paper or electronicforms) for decision-making about content,standardization, and other changes before setting up thenew EHRTo eventually modify the workflows and data and healthrecord collection and map the “new” workflows as theywill exist when the new EHR is fully implemented,including all changes in processes and EHR content28 2016. All Rights Reserved.
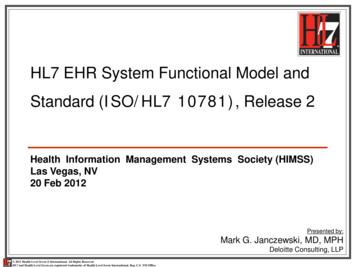
#5 Workflow Process MappingTrack clinical workflows inthree phases:Create a list of key clinicalprograms as the startingpoint to identify thenumber of workflows thatneed to be documentedand analyzed29 2016. All Rights Reserved. Phase One: Referral & Access ToCare Phase Two: Routine Care Phase Three: Discharge & TransferCreate a task for additionalworkflows (this mayinclude administrativeareas like reporting criticalincidents or specific areasof program workflows,such as prescribers seeingpatients in an outpatientmental health clinic)
30 2016. All Rights Reserved.
31 2016. All Rights Reserved.
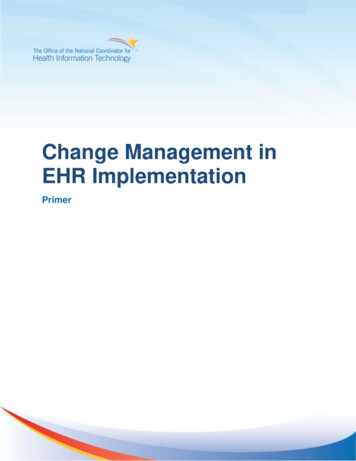
Medicaid eligibility hasbeen verified andreferral packet iscomplete.Refer back toreferralsourceSchedule a BMSadmission teaming(all team memberspresent)NOCall parents/referral source/school,etc to inform them that a referralwas received and ask if they arestill interested in services.Every 90 days(after 3 monthlyreviews) updatethe service plan.This must be sentto the directorand clinicalsupervisor forapproval.Every 90 daysupdate CAFAS andPCP notification.PCP notificationssent to PCP viafax/mail/handdeliver.32YESMonthly reviewsneed to take placeevery monthwithin 30 days ofthe prior review.These must besent to thedirector andclinical supervisorfor approval.Update Releases ofinformation every 6months (180 days). Mail orfax to collaboratingentities related to thereleases. 2016. All Rights Reserved.Identify a provider match.The provider match consistsof personalities, interventiontechniques, schedules, etc based on the client’s need.Within 30 days ofthe comprehensiveservice planschedule andconduct monthlyreview with allteam members atthe location ofservice.Updated everyyear are the FBA,EPSDT, SEDdocumentation.Give a copy of theapproved serviceplan to the BMSprovider andapplicable parties.Have team signcomprehensivesign in sheet.Discharges shouldall be planned anda team decision.Discharge CAFAS;Discharge PCPnotification,Discharge teammtg, dischargesummary,dischargenotification.At the BMS admissionmeeting complete theBMS admission teammeeting, BMS Ctorientation, and getinformation for functionalbehavioral assessment.Send to Director andClinical Supervisor forapprovalWithin 14 days ofadmissioncomplete the FBAandComprehensiveService plan. Sendboth to directorand clinicalsupervisor forapproval.Within 10 days ofadmissioncomplete CAFAS.Immediatelycomplete BMSassignment sheetand give a copy tothe BMS provider.The assignment sheet isupdated anytime there isa change in provider,scheduled hours, location,emergency info, etc.Immediatelycompleteadmissionnotification formand send toenrollment.BMS providers write progress notes every day thatthey are with a client. These notes are to besubmitted no later thanMonday at 9:00am.Other BMS documents due by the provider:Behavioral maps (due by the 20th of every month)Behavioral Observations (one weekly)Skillstreaming Sheets (one weekly)School cards (one weekly if school based)Time sheets (one weekly)
33 2016. All Rights Reserved.
#6 Clinical Form Content DecisionsThis includes all tasks that revolve around reviewing clinical forms that willbe part of the EHR, the technical design and review, and system set-upVendors typically haveform libraries and/or allowcustomers to share forms34 2016. All Rights Reserved.
#6 Clinical Form DevelopmentFor each new form Initial form review and approvalof content Technical form design ormodification Form review and feedback forchanges Final form sign-off, completion,and hanging in the system35 2016. All Rights Reserved.
#7 System Table & Structure Set-UpThis is for all system set-up tasks - it is usually very comprehensiveand ultimately affects how the overall system and reporting works Cost center, programs, locations Service codes and payers Other key system table files36 2016. All Rights Reserved.
#8 Billing Set-Up & TestingThis is for all tasks to setup billing in the newsystem as well as forthorough testing toensure it works correctly37 2016. All Rights Reserved.
#8 Billing Set-Up & Testing Tasks1238 Develop a task for all set-up items for the billing system Develop a full testing plan to confirm that the system creates a correct bill for all services and allpayers3 Conduct the testing plan4 Correct any errors and re-test necessary items5 Do an electronic billing test for all payers that accept electronic claims (set these up as separatetasks)6 If possible, do an electronic remittance test - in order to do this, you may need to duplicate aREAL billing run from the old system in the new system so that you can load the electronicremittance for testing in the new system7 Develop detailed instructions for billing and accounts receivable staff on using the new system,including a schedule of daily, weekly, and monthly activities 2016. All Rights Reserved.
#9 Report Needs Assessment & DevelopmentThis is for all tasks for report development for the programs being implementedKey tasks for each new report or report modification: 39Initial report specifications for the programmerReport developmentReview, feedback, and revisionsQueries, sorts, defaults definedReports hung in system 2016. All Rights Reserved.
State Reporting & Other Required OrCompliance ReportingMost often, this is monthlyreporting of consumerdemographic, service delivery, andoutcome dataIn some instances the data iscumulative (such as fiscal year-todate data which can complicate dataconversion and go-live planning)40 2016. All Rights Reserved.
#10 Software Interface Needs Assessment &DevelopmentThis is for all tasks related to identifying all interfaces that need to be built forthe new software application as well as the detailed plans for developing andtesting the interfacesFor each interface, create fourtasks 41Planning the interfaceDeveloping the interfaceTesting the interfacePlanning the implementation of theinterface 2016. All Rights Reserved.
Typical Interfaces Or Data ExchangesGL / R applicationsCRMapplicationsLaboratoriesand pharmaciesState, county, orother systemsOther payers42 2016. All Rights Reserved.Other providers
#11 Meaningful Use Registration &ImplementationThis is for all tasks related toimplementing meaningfuluse requirements as well asobtaining meaningful usefederal dollars under theincentive program43 2016. All Rights Reserved.
EHR ImplementationIII. System Freeze &Final Preparation #12 Final workflowtesting #13 Training materialsand execution #14 Final go-livepreparation44 2016. All Rights Reserved.
#12 Final Workflow TestingOnce the entire system has been set-up, it must be “frozen” so that the finalworkflow testing can be completedYou can’t finalize the workflowsand develop training materialsuntil the entire system is set-up!45 2016. All Rights Reserved.
#13 End User Training Material Development &PlanThis is for all tasks related to developing best-practice training materials andexecuting the training plan for end users prior to go-live for each programKey tasks include: Define training groups, anticipatednumber of attendees for each group,and list of key things to train each group Develop model for handling all traininglogistics Develop training material developmentplan46 2016. All Rights Reserved.
#14 Go-Live PlanningThis is for all remaining tasks related to preparing for the final go-liveTypically, they include: Final data conversion and possible duplicatenew client entry for a short period of time Identifying all post-data conversion data entrythat needs to occur and developing a plan forexecution (e.g. caseloads, appointments,updated diagnoses, medication information,etc.) Planning the roll-out of treatment plan dataentry into the new EHR On-site staff support for go-live date47 2016. All Rights Reserved.
EHR ImplementationIV. Expanding &Leveraging The EHRImplementation #15 Implementing morefeatures #16 Leveraging datathrough businessintelligence tools #17 Additional clinical andanalytic use48 2016. All Rights Reserved.
EHR Implementation49I. RoutineElementsII. Complex #1 Vendortraining andimplementation #2 Hardware #3 Dataconversion #4 Mobilesystem use #5 Workflows #6 Clinicalcontent #7 System setup #8 Billing testing #9 Reports #10 Interfaces #11 Meaningfuluse 2016. All Rights Reserved.ElementsIII. SystemFreeze &FinalPreparationIV. Expanding &Leveraging TheEHRImplementation #12 Finalworkflow testing #13 Trainingmaterials andexecution #14 Final go-livepreparation #15 Implementingmore features #16 Leveraging datathrough businessintelligence #17 Additional clinicaland analytic use
50Confidential & Proprietary
Drivers of ImplementationSuccess and Failure basedon Study and Practice.Matthew M. Dorman, CEOCredible Behavioral Health, Inc.51Confidential & Proprietary
Matthew M. Dorman, CEO Credible 52300 Partners Agencies280 Implementations LiveBasement to 150 staff in 9 states 3,000,000,000 Annual Billing“Dark Side” (Investment Banking)Fortune 500 AlumniSecond of Three National Bcare EHR companiesBootstrapped 15 years, 30M Goldman investmentFormer Board Member, MD PRPMBA Finance - UMD; BA PoliSci - Univ. of DEFocus, Persistence, “Unreasonableness”Confidential & Proprietary
Matthew M. Dorman, CEO Credible 300 Partners Agencies 285 Implementations Live 53Basement to 150 staff in 9 states 3,000,000,000 Annual Billing“Dark Side” (Investment Banking)Fortune 500 AlumniSecond of Three National Bcare EHR companiesBootstrapped 15 years, 30M Goldman investmentFormer Board Member, MD PRPMBA Finance - UMD; BA PoliSci - Univ. of DEFocus, Persistence, “Unreasonableness”Confidential & Proprietary
Implementation: Experience Matters54Confidential & Proprietary
Implementation Success & Failure55Confidential & Proprietary
Agenda1. Implementation Terms2. Basic Implementation Strategies3. Experience aka Track Record:Yours and Vendor4. What your vendor doesn’t wantyou to know aboutImplementation.56Confidential & Proprietary
Implementation Terms1.2.3.4.5.6.7.8.9.10.57“Going Live”Data ConversionProject TeamWork Flow AnalysisSaaS/Client Server/HostedBandwidthService/SurveysMilestonesIT v Clinical v Financial Driven ProjectManagement InvolvementConfidential & Proprietary
Implementation Strategies58Confidential & Proprietary
Implementation Strategies1.Most Prevalent 2.Most Scalable 59Custom – “Agency is Always Right”Professional ServicesTime & MaterialsPre-setUniformOnline trackingTransparencyClear road mapConfidential & Proprietary
Track Record & Experience60Confidential & Proprietary
Experienced Gardener?61Confidential & Proprietary
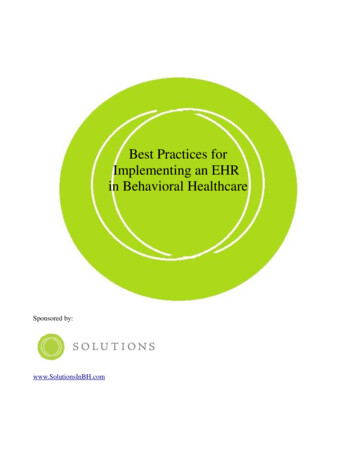
Partner (Agency) BandwidthHiLoRole & Agency KnowledgeHi
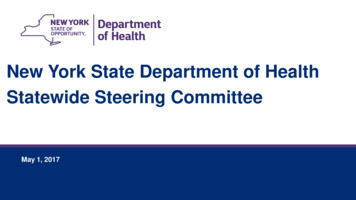
Track Record & ExperienceAgency Strengths1. Clinical Knowledge2. Key Drivers3. Billing4. More staff (?)5. Agency Knowledge6. InfluenceManagement63Vendor Strengths1. Software Knowledge2. Industry Key Drivers3. Billing (?)4. Focused staff (?)5. Clinical Knowledge6. ImplementationExperienceConfidential & Proprietary
Track Record & ExperienceAgency Strengths1. Clinical Knowledge2. Key Drivers3. Billing4. More staff (?)5. Agency Knowledge6. InfluenceManagementVendor Strengths1.Software Knowledge2.3.Industry Key DriversBilling (?)Focused staff (?)Clinical Knowledge4.5.6.ImplementationExperienceFailed and Successful GoLives64Confidential & Proprietary
65Confidential & Proprietary
What YourVendor MayNot Want YouTo Know.66Confidential & Proprietary
Keys to the Castle1.2.3.4.5.6.67Annual GoLives last 24 monthsImplementation Staff v TotalStaff Bandwidth/CapacityLast 12-18 months SalesImplementation DurationsBilling Capacity US Your StateConfidential & Proprietary
Keys to the Castle7.8. 9.10. 11.12.68State & Custom ReportingState PresenceBrandExpertiseExperienceEconomies of scaleFinancial Stability v SizeRevenue modelReRev v big hitFailures and EffectConfidential & Proprietary
69Confidential & Proprietary
Keys to the Castle1.2. 3.4. 5.State & Custom ReportingState PresenceBrandExpertiseExperienceEconomies of scaleFinancial Stability v SizeRevenue modelReRev v big hitFailures and Effect6. Vendor Plan & Strategy70Confidential & Proprietary
Plans Matter71Confidential & Proprietary
72January 2015 Off-Site – St. Petersburg, FL
Questions?732/1/2017Confidential & Proprietary
Seven Steps To EffectiveEHR Implementation
Seven Steps To Effective EHR Implementation1.2.3.4.5.6.7.75 Identify the objectives of implementing an EHR & selecting the right vendor Establish a steering committee and well-rounded implementation team Assess the organization’s current operations, workflow, and clinical documentation Complete system installation, configuration, and thorough testing Develop training materials and conduct staff training System go-live Evaluate system performance and leverage the EHR’s capabilities over time 2016. All Rights Reserved.
Lessons LearnedWhen implementing an EHR, keep in mind you don’t justneed a good software product. You need a vendorrelationship that support you in being successful.It is critical to define what a full implementation of theEHR will mean for your organization so that you canensure the functionality and benefits are achieved.EHR implementations require heavy duty projectmanagement skills – to keep all aspects of the project ontime and on budget.Staff engagement, from leadership to line staff, is criticalfor success.76 2016. All Rights Reserved.
Questions & Discussion
Turning market intelligenceinto business advantageOPEN MINDS helps over 180,000 industry executives tackle business challenges,improve decision-making, and maximize organizational performance every day.See how our market intelligence can help your organization at www.openminds.com.Mental Health Services Chronic Care Management Disability Supports & Long-Term CareAddiction Treatment Social Services Intellectual & Developmental Disability SupportsChild & Family Services Juvenile Justice Adult Corrections Health Care@openmindscirclewww.openminds.comnOPEN MINDS Circle163 York Street, Gettysburg, Pennsylvania 17325OPEN MINDS Circlen717-334-1329ninfo@openminds.com
EHR Implementations The Good There is consensus among behavioral health providers that implementation of an electronic health record (EHR) system brings value when things go right The majority of providers report implementing an EHR in 6-12 months The Bad Challenges include lack of involvement from executive leadership, staff engagement,