Transcription
2019 External Quality HENSIVETECHNICAL REPORTFOR CONTRACT YEARJUNE 2019 – MAY 2020Submitted: May 11, 2020Prepared on behalf of theMississippi Division of Medicaid
2019 External Quality ReviewEXECUTIVE SUMMARY . 4A. Overall Findings . 4Administration . 4Provider Services . 5Member Services . 6Quality Improvement . 7Utilization Management. 13Delegation. 13B. Overall Scoring .13BACKGROUND . 15METHODOLOGY . 15FINDINGS .16A. Administration .16Information Systems Capabilities Assessment . 17Strengths . 20Weaknesses . 20Recommendations . 20B. Provider Services . 20Provider Access and Availability Study . 22Provider Satisfaction Survey . 25Strengths . 34Weaknesses . 35Recommendations . 35C. Member Services . 36Member Satisfaction Survey . 38Strengths . 42Weaknesses . 42Recommendations . 43D. Quality Improvement . 43Performance Measure Validation . 44Performance Improvement Project Validation . 60Strengths . 64Weaknesses . 64Recommendations . 64E. Utilization Management . 65Strengths . 71Weaknesses . 71Recommendations . 71F. Delegation. 72Strengths . 74Weaknesses . 74Recommendations . 74
2019 External Quality ReviewEXECUTIVE SUMMARYThe Balanced Budget Act of 1997 (BBA) requires each State Medicaid Agency that contractswith Managed Care Organizations (MCO) evaluate their compliance with the state andfederal regulations in accordance with 42 Code of Federal Regulations (CFR) 438.358. Tomeet this requirement, the Mississippi Division of Medicaid (DOM) contracted with TheCarolinas Center for Medical Excellence (CCME), an external quality review organization(EQRO), to conduct External Quality Review (EQR) for all Coordinated Care Organizations(CCO) participating in the MississippiCAN (CAN) and Mississippi CHIP (CHIP) MedicaidManaged Care Programs. The CCOs include UnitedHealthcare Community Plan – Mississippi(United) and Magnolia Health (Magnolia).The purpose of the external quality reviews was to ensure that Medicaid enrollees receivequality health care through a system that promotes timeliness, accessibility, andcoordination of all services. This was accomplished by conducting the following activitiesfor the CAN and CHIP programs: validation of performance improvement projects,performance measures, and surveys, compliance with state and federal regulations, andaccess studies for each health plan. This report is a compilation of the annual reviewfindings of the CAN and CHIP programs for each CCO conducted in 2019.A. Overall FindingsAn overview of the findings for each section follows. Additional information regarding thereviews for United and Magnolia, including strengths, weaknesses, and recommendationscan be found further in the narrative of this report.AdministrationUnited and Magnolia have established policy management processes and require atleast annual review of policies; however, some of United’s policies did not reflect anannual review and did not reveal the line(s) of business to which they apply.Although overall health plan staffing appears adequate, United was not in compliancewith DOM’s requirement for a minimum of eight representatives to provide face-toface provider services and two additional representatives designated for out-of-stateproviders.Both Magnolia and United have thorough, documented processes to guard againstfraud, waste, and abuse (FWA) and codes of conduct defining standards of ethicalbehavior for staff. The health plans provide mandatory Compliance training to staffand have suitable processes for training and educating providers about compliance andFWA requirements, laws, and regulations. CCME encouraged United to revise its CANand CHIP Member Handbooks to provide a more comprehensive explanation of FWA toenhance member understanding of these concepts. The plans provide appropriateavenues for reporting potential compliance, FWA, and ethics concerns or violations,4Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality Reviewensure anonymous reporting capabilities are available, and have no-retaliation policiesin place.United’s reported claims payment rate of 85% to 90% completion after three monthsfalls below the contractual requirement that 99% of clean claim payments becompleted within 90 days and shows a need for United to improve its clean claimpayment rate. Magnolia did not provide exact claims statistics but indicated internalclaims audits ensure 100% of clean claims are finalized within 30 calendar days and100% of all claims are processed and paid within 90 calendar days of receipt.United’s business continuity plans summarize approaches to keeping systems availableduring events that could cause interruptions and restoring operations if a disasteroccurs. However, United conducted only limited testing on those processes. Magnolia’smulti-tiered IT infrastructure is regularly maintained, frequently audited, and capableof being recovered after a disaster. Recent disaster recovery test results indicateMagnolia’s ability to successfully recover systems and meet recovery time objectives.Provider ServicesThe health plans define processes and requirements for provider credentialing andrecredentialing in policies with state-specific credentialing addressed in attachmentsor in credentialing plans with addenda defining additional state-specific requirements.CCME noted policies do not address all credentialing/recredentialing requirements,contain incorrect information, and/or do not clearly reflect the processes followed bythe health plan. Both United and Magnolia have committees with appropriatemembership to make credentialing and recredentialing decisions. The committees arechaired by the health plan’s Chief Medical Director/Officer, meet at the establishedfrequency, and have defined quorums. CCME’s review of credentialing andrecredentialing files revealed several issues: lack of proof of query of the MS DOMSanctioned Provider List (Magnolia and United), outdated, incomplete, or missingOwnership Disclosure forms (Magnolia and United) and primary source verification of aClinical Laboratory Improvement Amendment (CLIA) certificate (Magnolia), and failureto conduct office site visits for nurse practitioners acting as PCPs (United).During the previous EQR, United’s credentialing and recredentialing files were notedwith Ownership Disclosure forms signed by unauthorized persons. United respondedduring the corrective action process with an updated Provider Entity Disclosure ofOwnership form containing a statement ensuring the signer had authority to legallybind the entity; however, findings of the current review indicated the updatedOwnership Disclosure form was not implemented.United and Magnolia regularly measure and monitor the adequacy of their providernetworks using measurement standards that are compliant with contractualrequirements. However, Magnolia’s documentation revealed the standards documented5Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality Reviewin policy were not the same as those used for the actual geographic distributionmeasurements.Provider orientation processes are in place and ongoing provider education is providedthrough newsletters, webinars, and resource information available on the website’sprovider portal (United), and through newsletters, informational postcards and letters,resource information on the provider portal, and regularly scheduled meetings with innetwork providers (Magnolia). When comparing documentation of member benefits inthe health plans’ Member Handbooks and Provider Manuals, CCME noted numerousdiscrepancies in the information provided.The health plans conduct annual medical record audits to evaluate network medicalrecord-keeping practices. Although Magnolia’s Medical Record Review policy states anaggregate summary of medical record reviews completed are presented quarterly toMagnolia’s Quality Committee, CCME could not find evidence that this information isreported to the Quality Committee.Both health plans had noted improvements in rate of successfully answered calls forthe 2019 Telephonic Provider Access Study when compared to the 2018 study. Also, aspart of the EQR, CCME validated the health plans’ Provider Satisfaction Surveys andidentified survey response rate as an area needing improvement for both health plans.Member ServicesMagnolia and United have policies and procedures for CAN and CHIP that define anddescribe member rights and responsibilities, as well as methods for notifying membersof their rights and responsibilities. Information is included in Member Handbooks,Provider Manuals, on websites, and in member newsletters. However, CCME identifiedincomplete or omitted requirements with documentation of member’s rights andresponsibilities.The health plans provide toll-free telephone numbers and descriptions for MemberServices and for the 24-hour nurse lines in Member Handbooks and websites. CAN andCHIP members are also encouraged to obtain recommended preventive services(including well-child services) via the website, at community events, and throughreminder phone calls, Member Handbooks, and mailings.Review of the grievance policies and related information in Member Handbooks,Provider Manuals, and on Magnolia’s and United’s CAN and CHIP websites revealedissues such as incomplete definitions of grievance terminology, use of outdatedterminology, and incomplete and incorrect information about requirements forgrievance acknowledgement and resolution timeframes.Issues identified in the review of grievance files included untimely acknowledgmentletters, incorrectly stating the grievance in the resolution letter, and resolution lettersthat contained outdated information, typographical errors, or improper resolutions.6Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewThe health plans appropriately retain grievance and complaint data for thecontractually-required timeframe and use the data for quality improvement activities.Magnolia and United continue to conduct the Consumer Assessment of HealthcareProviders and Systems (CAHPS ) surveys annually via a third-party vendor. Membersatisfaction validation for the health plans was performed based on the CMS SurveyValidation Protocol. Generalizability of the survey results is difficult to discern due tolow response rates and recommendations were provided to address this issue.Quality ImprovementQuality Improvement (QI) program descriptions adequately described the programsMagnolia and United have implemented to monitor, evaluate, and improve the qualityof clinical care and services provided to their members. Both plans provided their 2018and 2019 work plans. The activities or scope of work in Magnolia’s Behavioral Healthwork plans were identical to the CAN and CHIP work plans and not specific toBehavioral Health.Committees responsible for implementing, monitoring, and directing QI activities wereestablished for both health plans. Membership includes a variety of network providers,senior executives, directors, and other health plan staff.Magnolia and United conducted an evaluation of the effectiveness of the QI programs.Program evaluations included the QI activities conducted in 2018, results of thoseactivities, any barriers identified, interventions, and recommendations for 2019.Health plans are required to have an ongoing program of Performance ImprovementProjects (PIPs) and to report plan performance using Healthcare Effectiveness Data andInformation Set (HEDIS ) measures applicable to the Medicaid population.CAN Performance MeasuresWhen evaluating specific measures for each CAN program, the timing of the reviewscreated a one-year gap in performance measure reporting. Thus, the year over yeartrending for each plan included MY 2016 (HEDIS 2017) and MY 2018 (HEDIS 2019). Asshown in Table 1: Magnolia CAN HEDIS Measures with Substantial Changes in Rates, forMagnolia, there were several measures that had substantial improvement of greaterthan 10%: BMI Percentile for Children/Adolescents, Counseling for Physical Activity,HPV vaccines, and Well Child Visits in the First 15 Months of Life. The only measurewith a substantial decrease in rate was the Cardiovascular Monitoring for People withCardiovascular Disease and Schizophrenia.7Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewTable 1: Magnolia CAN HEDIS Measures with Substantial Changes in RatesMeasureYear2016Measure/Data ElementMeasureYear2018Changefrom 2016to 2018Substantial Increase in Rate ( 10% improvement)Weight Assessment and Counseling for Nutrition and Physical Activity for Children/Adolescents(wcc)BMI Percentile45.91%57.42%11.51%Counseling for Physical Activity34.38%47.45%13.07%5.29%20.19%14.90%12-18 0%70.19%10.19%37.43%52.45%15.02%64.15%-15.44%Human Papillomavirus Vaccine for Female Adolescents(hpv)Asthma Medication Ratio (amr)Statin Therapy for Patients with Cardiovascular Disease (spc)Received Statin Therapy - 40-75 years (Female)Well-Child Visits in the First 15 Months of Life (w15)6 VisitsSubstantial Decrease in Rate ( 10% decrease)Cardiovascular Monitoring for People with CardiovascularDisease and Schizophrenia (smc)79.59%For United, there were several measures that had substantial improvement of greaterthan 10% in that time frame, including HPV and Combination #2 Immunizations forAdolescents, and A1C Control. The measures with a substantial decrease in rate wereMetabolic Monitoring for Children and Adolescents on Antipsychotics for 1-5 year-oldsand Alcohol Abuse or Dependence: Initiation of AOD Treatment: Total. Table 2: UnitedCAN HEDIS Measures with Substantial Changes in Rates.Table 2: United CAN HEDIS Measures with Substantial Changes in RatesMeasureYear2016Measure/Data ElementMeasureYear2018Change from2016 to2018Substantial Increase in Rate ( 10% improvement)Immunizations for Adolescents (ima)HPV6.81%18.98%12.17%Combination #26.08%17.27%11.19%Comprehensive Diabetes Care (cdc)8Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewMeasure/Data ElementHbA1c Control ( 8.0%)MeasureYear2016MeasureYear2018Change from2016 34.37%-11.52%Substantial Decrease in Rate ( 10% decrease)Comprehensive Diabetes Care (cdc)HbA1c Poor Control ( 9.0%)56.93%Metabolic Monitoring for Children and Adolescents on Antipsychotics (apm)1-5 Years35.42%Initiation and Engagement of AOD Abuse or Dependence Treatment (iet)Alcohol abuse or dependence: Initiation of AOD Treatment:Total45.89%Non-HEDIS performance measures were uploaded to the desk materials and reviewed incomparison to target rates. Table 3: CAN Non-HEDIS Performance Measure Ratesdisplays the CY 2018 rate and the State target rate. Magnolia met the target rate fortwo of the five measures, and United met the target rate for one of the five measures.Table 3: CAN Non-HEDIS Performance Measure RatesMagnoliaCAN(CY 2018)UnitedCAN(CY 2018)MS CANTarget RateEPSDT Screening ( 1 Year)313.60%116.74%85%EPSDT Screening ( 1, 21 Years)59.78%54.13%75%Well-Child Visits in the 1st 15 months of life52.45%59.44%59.76%Nephropathy Screening90.51%89.78%90.33%Screening for Clinical Depression21.49%5.87%25%Measure/Data ElementCHIP Performance MeasuresFor Magnolia CHIP, when comparing the MY2016 CHIP rates to the MY2018 CHIP rates,there were several measures that had substantial improvement of greater than 10%:Asthma Medication Compliance, Follow Up Care for Children on ADHD MedicationContinuation Phase, Follow up after Hospitalization for Mental Illness, and Well-ChildVisits. The measure of 5 Well-Child Visits in the First 15 Months of Life did have asubstantial decrease, but the 6 well child visits increased substantially.9Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewTable 4: Magnolia CHIP HEDIS Measures with Substantial Changes in RatesMeasureYear2016Measure/Data ElementMeasureYear2018Change from2016 to2018Substantial Increase in Rate ( 10% improvement)Medication Management for People with Asthma (mma)5-11 Years: Medication Compliance 50%45.45%64.84%19.39%5-11 Years: Medication Compliance 75%15.91%32.81%16.90%12-18 Years: Medication Compliance 75%*16.67%27.03%10.36%Total Medication Compliance 50%44.12%58.51%14.39%Total Medication Compliance y follow-up55.29%66.10%10.81%Total-7-day %-15.84%Follow-up care for children prescribed ADHD Medication (add)Continuation and Maintenance (C&M) PhaseFollow-Up After Hospitalization for Mental Illness (fuh)Well-Child Visits in the First 15 Months of Life (w15)6 VisitsSubstantial Decrease in Rate ( 10% decrease)Well-Child Visits in the First 15 Months of Life (w15)5 Visits29.63%As noted in Table 5: United CHIP HEDIS Measures with Substantial Changes in Rates,United did not have any measures with a substantial improvement of greater than 10%,although many rates improved. The Antidepressant Medication Management andFollow-Up After Hospitalization for Mental Illness measures declined substantially( 10%).Table 5: United CHIP HEDIS Measures with Substantial Changes in RatesMeasure/Data ElementMeasureYear2016MeasureYear2018Change from2016 to201832.35%-15.27%Substantial Decrease in Rate ( 10% decrease)Antidepressant Medication Management (amm)Effective Acute Phase Treatment47.62%10Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewMeasureYear2016MeasureYear2018Change from2016 to201833.33%17.65%-15.68%Total-30-day Follow-Up76.97%61.39%-15.58%Total-7-day Follow-Up53.95%35.15%-18.80%Measure/Data ElementEffective Continuation Phase TreatmentFollow-Up After Hospitalization for Mental Illness (fuh)Table 6: CHIP Non-HEDIS Performance Measure Rates, displays the most recentmeasurement rates for the United and Magnolia CHIP Programs. Magnolia met thetarget rate for two of the three measures, and United met the target rate for one ofthe three measures.Table 6: CHIP Non-HEDIS Performance Measure RatesMagnoliaCHIPCY2018UnitedCHIPCY2018MS CHIPTarget RateEPSDT Screening ( 1 Year)366.67%107.27%85%EPSDT Screening ( 1, 21 Years)38.92%47.92%75%Well-Child Visits in the 1st 15 months of Life70.02%48.18%59.76%MeasurePlan rates for the most recent review year with the statewide averages are reported inSection D: Quality Improvement of this report.Performance Improvement ProjectsEach health plan is required to submit their performance improvement projects (PIPs)to CCME for review annually. CCME validates and scores the submitted projects using aCMS designed protocol that evaluates the validity and confidence in the results of eachproject. The 16 projects reviewed for the CAN and CHIP programs for the two plans aredisplayed in Table 7: Results of the Validation of PIPs.Table 7: Results of the Validation of PIPsProjectValidation ScoreMagnolia CANAsthmaBehavioral Health Readmissions91/91 100%High Confidence in Reported Results67/72 93%High Confidence in Report Results11Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewProjectValidation Score62/62 100%High Confidence in Report Results67/72 93%High Confidence in Report ResultsImproved Pregnancy Outcomes with MakenaSickle Cell Disease OutcomesMagnolia CHIP91/91 100%High Confidence in Report Results102/105 97%High Confidence in Report ResultsEPSDTObesity for ChildrenADHD90/91 99%High Confidence in Report ResultsUse of Appropriate Medications for People withAsthma91/91 100%High Confidence in Report ResultsUnited CANBehavioral Health Readmissions78/78 100%High Confidence in Reported ResultsImproved Pregnancy Outcomes: CareManagement to reduce preterm deliveries62/62 100%High Confidence in Reported ResultsSickle Cell Disease Outcomes: CareCoordination for SCD Patients to Reduce ERUtilization57/62 92%High Confidence in Reported Results62/62 100%High Confidence in Reported ResultsRespiratory Illness: COPD/AsthmaUnited CHIPAdolescent Well Child Visits104/105 99%High Confidence in Reported ResultsWeight Assessment and Counseling forNutrition and Physical Activity forChildren/Adolescents- formerly calledReducing Adolescent and Childhood Obesity111/111 100%High Confidence in Reported ResultsGetting Needed Care CAHPS111/111 100%High Confidence in Reported ResultsFollow Up After Hospitalization for MentalIllness84/85 99%High Confidence in Reported ResultsMagnolia and United CAN and CHIP plans scored in the “High Confidence” range for all16 submitted and validated PIPs. Scores ranged from 92% to 100%. There were no PIPsthat scored in the “Confidence,” Low Confidence,” or “Not Credible” scoringcategories.12Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewUtilization ManagementFor Magnolia and United, assessment of utilization management (UM) included reviewsof CAN and CHIP program descriptions and evaluations, policies, Member Handbooks,Provider Manuals, approval, denial, appeal, and case management files, and planwebsites. Policies and procedures define how UM services are operationalized andprovided to members.The respective UM program descriptions outline the purpose, goals, objectives, andstaff roles for physical and behavioral health. Review of approval and denial files metcriteria and timeframe requirements.The CAN and CHIP Care Management (CM) program description and policiesappropriately document care management processes and services provided. CM filesindicate care gaps are identified and addressed consistently, and services are providedfor various risk levels.The health plans have established policies defining processes for handling both CANand CHIP appeals of adverse benefit determinations. Review of documentation inpolicies, Member Handbooks, Provider Manuals, etc. revealed numerous issues ofincomplete, incorrect, and missing information about appeals processes andrequirements. Several of Magnolia’s issues were identified during the 2018 EQR andhave not been corrected. CCME’s review of appeal files revealed only isolated issuesand, overall, appeals are handled correctly. Both health plans use appeal data toidentify opportunities to improve quality of care and service.DelegationMagnolia and United ensure all delegation arrangements are governed by writtenagreements between the delegate and the health plan that describe the roles andresponsibilities of the health plan and the delegated entity, delegated activities,reporting requirements, processes by which the delegated entity's performance isevaluated, and terms for revoking delegation.For credentialing and recredentialing oversight, United conducted annual audits toassess compliance with defined standards. The audit tool was comprehensive andincluded file review. However, the delegated credentialing and recredentialing toolsomit the requirement for ensuring the entities collect Ownership Disclosure forms andquery the Social Security Death Master File.B. Overall ScoringTo objectively compare the CCOs, CCME applied a numerical score (points) to eachstandard’s rating within a section to derive the overall score (percentage) for each planand each Medicaid program. Using the Centers for Medicare & Medicaid Services (CMS)13Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
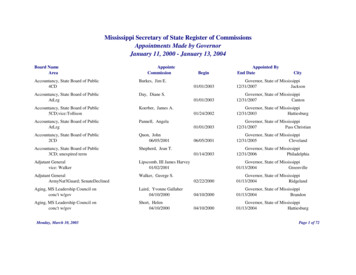
2019 External Quality ReviewProtocol, External Quality Review Protocol for Accessing Compliance with MedicaidManaged Care Regulation, the overall score was calculated based on the following method:Points were assigned to each rating ("Met" 2 points and "Partially Met" 1 point),excluding "Not Evaluated" and "Not Applicable" ratings from the calculation.1. The total points achieved for each section was calculated by adding the earned pointstogether.2. The final section score was derived by dividing the section’s total points (totalnumber achieved) by the total possible points for that section.3. The overall score (percentage) was then calculated by averaging the final sectionscores for the six sections reviewed.Results of the scoring matrix are included in Table 8: Overall Scoring Matrix.Table 8: Overall Scoring gure 1, Overall Results for 2019 EQR, provides an overview of the percentage of “Met,”“Partially Met,” “Not Met,” “Not Evaluated,” or “Not Applicable” scores by health planand Medicaid program.Figure 1: Overall Results for 2019 EQRPercent of Standards Evaluated2019 EQR 0%8.0%1.0%6.0%0.5%8.1%91.0%91.0%93.0%91.4%United CANUnited CHIPMetMagnolia CANPartially MetMagnolia CHIPNot Met14Annual Comprehensive Technical Report for Contract Year June 2019 - May 2020 May 11, 2020
2019 External Quality ReviewBACKGROUNDThe Mississippi Division of Medicaid (DOM) contracted with two coordinated careorganizations (CCOs) to administer the Mississippi Coordinated Access Network(MississippiCAN) and the Mississippi Children’s Health Insurance Program (MississippiCHIP), Medicaid managed care programs. The CCOs include UnitedHealthcareCommunity Plan – Mississippi (United) and Magnolia Health (Magnolia). The BalancedBudget Act of 1997 requires State Medicaid agencies that contract with Medicaidmanaged care organizations evaluate their compliance with state and federalregulations in accordance with 42 Code of Federal Regulations (CFR)
Quality Improvement (QI) program descriptions adequately described the programs Magnolia and United have implemented to monitor, evaluate, and improve the quality of clinical care and services provided to their members. Both plans provided their 2018 and 2019 work plans. The activities or scope of work in Magnolia's Behavioral Health