Transcription
BREASTFEEDING PROTOCOL:Positioning and Latching
The Breastfeeding Protocols are based on the City of Toronto’s Breastfeeding Protocols for HealthCare Providers (2013) and are co-owned by the City of Toronto, Toronto Public Health Division(TPH) and the Toronto East Health Network, Baby-Friendly Initiative (BFI) Strategy for Ontario.Revised Protocols are being released as they are completed, and they are available at breastfeeding-protocols-health-care-providers. Allrevised Protocols, as well as the complete set of 2013 Protocols, are available at 013.pdf.F unding for this project was received from the Government of Ontario. The views expressedin the publication are the views of the Recipient and do not necessarily reflect those ofthe Province. For more details on the revision process and terminology, please see theIntroduction to Breastfeeding Protocols for Health Care Providers.ProcessThe process of revising and updating the Protocol followed a clear methodology based onEvidence-Informed Decision Making in Public Health www.nccmt.ca, developed by the NationalCollaborating Centre for Methods and Tools (NCCMT) and is described in the full Introduction,linked above. Every effort has been made to ensure the highest level of evidence is reflected.ContributorsProject Lead: Sonya Boersma, MScN, RN, IBCLC, BFI Strategy for Ontario.Thanks to the following individuals and organizations for their contributions:Revising Authors: Susan Gallagher, BScN, RN, and Tracy Petrou, BScN, RN, IBCLC,Toronto Public Health.External Reviewers:NAMEROLE AND/ORQUALIFICATIONSLOCATIONORGANIZATIONJennifer Abbass-DickAssistant ProfessorRN, PhD, IBCLCCentralUniversity of Ontario Instituteof TechnologyLina Al-ImariMD, BreastfeedingMedicineCentralDoctors’ Breastfeeding Clinic,Peel RegionJosdalyne AndersonMDEasternMonarch Centre,Independent PracticePamela DrynanPHNNorth EastTimmins & District Hospital,& Independent PracticeLaura DueckRN, PHNSouth WestMiddlesex-London Health UnitDanit FischteinMD, IBCLCCentralWell Medica Medical Centre,BramptonSusan HaywardMD, FCFP, FABMCentralQueen Square FamilyHealth TeamElaine JeffriesRNNorthernMoose Factory Hospital, WAHAHeather KefferMWWestMidwives Grey BruceWithin Ontario
NAMEROLE AND/ORQUALIFICATIONSLOCATIONORGANIZATIONSarah PattersonPaediatric RDTorontoMichael Garron HospitalJanice SullivanRN, IBCLCEasternCarlington Community CHCSue Theriault ValinIBCLCEastern IBCLC Independent Practice,Southeast Ottawa CommunityHealth Centre, La Leche Leaguefor Eastern ON & QCDeb Baumannand colleaguesClinical Coordinator& Educator for VIHABritish ColumbiaVancouver Island HealthAuthorityDonna BrownBFI CoordinatorNew BrunswickHorizon Health NetworkSarah ChapmanClinical Dietitian &Baby-FriendlyNewfoundland andLabradorNewfoundlandJaneway Children’s Healthand Rehabilitation CentreMarusia KachkowskiMPH, PHN, IBCLCManitoba Winnipeg Regional HealthAuthorityLisa RobertsBN, RN, IBCLCNewfoundland Regional Lactation Consultant,Eastern HealthWithin OntarioOut of OntarioBreastfeeding Protocol: Positioning and LatchingAdditional thanks to: L ead BFI Assessor Marg La Salle and Editor Kim Tytler. FI Strategy for Ontario team members who reviewed this Protocol: Doris Balcarras, Hiltrud BDawson, Louise Guthro, Yolande Lawson, Linda Young.Use of this ProtocolThe BFI Strategy for Ontario and TPH encourage individuals and organizations to use thisProtocol to support evidence-informed clinical practice. This Protocol may be copied or printedfor the purpose of educating health care practitioners, provided the authors are acknowledgedand content is not altered, nor used or reproduced for commercial gains.DisclaimerThis Protocol is a guideline. Every breastfeeding dyad and their circumstances must beassessed on an individual basis. In doing so, health care providers use their own professionaljudgement along with the evidence in assessing the care and support that the family needs.At times, consultation with another breastfeeding expert or advice from a medical practitioner,(physician, midwife, or nurse-practitioner), will be required.January 2019
Table of ContentsKey Messages . 1Principles of Positioning . 1 Biological Nurturing (laid-back or semi-reclined position) . 2 Benefits of Biological Nurturing. 3Techniques to Support Effective Latching . 3 Principles of Achieving an Effective Latch . 5 Signs of an Effective Latch . 5 Infant-led Latching . 6 Other Latching Techniques . 7- Nipple tilting . 7- Breast sandwich . 8- Dancer hand-hold, for special circumstances . 9 Practices to Prevent or Troubleshoot Latching Challenges. 10 How to Unlatch an Infant . 11Other Breastfeeding Positions . 11 Cross-cradle . 12 Cradle . 13 Football . 14 Side-lying . 15Breastfeeding Multiples . 16 V-hold . 17 Double football . 17 Combination cradle/football . 18 Criss-cross or double cradle . 18 Parallel . 18Key Resources . 19References . 20Breastfeeding Protocol: Positioning and Latching
Key Messages1. Any position that is comfortable for the motherand infant and allows for effective breastmilk transfer is an acceptable position. Whenpositioning is comfortable, and the infant is wellaligned with the breast, a deep and effectivelatch is more likely.2. Effective positioning and latching are essential forsuccessful breastfeeding and can: Help the infant to suck effectively. Ensure effective breast milk transfer to assistwith optimal growth of the infant. Stimulate, build, and maintain a mother’sbreast milk production. Help prevent many breastfeeding problemssuch as sore nipples, mastitis, low breast milksupply, and poor infant weight gain.3. Baby-led latching is a natural and intuitive approach for an infant to find the breast and latchor self-attach.4. Breastfeeding positions can vary and change depending on an infant’s size, gestational ageand abilities, maternal body shape, breast size and shape, recent procedures, and mother’spreference.Principles of Positioning Mother is in a relaxed and comfortable position that does not cause pain (e.g., from anepisiotomy or caesarean birth). Mother and infant are well supported. Supports may be used to help a mother find acomfortable position while breastfeeding. A pillow, rolled blanket, or rolled towel may help tosupport a mother’s arm. Mother holds the infant unswaddled, tucked in close “tummy-to-mommy” with shoulders andhips aligned and well supported. Some practitioners suggest an infant is well aligned if animaginary line can be drawn from the infant’s ear, to shoulder, to hip. The infant’s head and neck are slightly extended which means slightly tilted back, sometimescalled a sniffing position. During latching, the infant’s head is slightly extended with the lower lip or chin touching thebreast. This will allow for a deep latch. Teach the mother to pay attention to the amount of areola in the infant’s mouth. Sometimesthe natural relaxation that happens with feeding leads to the areola slipping out. Encourage the mother to notice any tension in her shoulders and then relax them. There is a strong interaction between head and neck position and feeding function. A slightlyextended position positively affects respiratory mechanisms, oral motor control, and swallowing.Head and body alignment work together to achieve a position that enables breast milk transfer(Walker, 2014).1Breastfeeding Protocol: Positioning and Latching
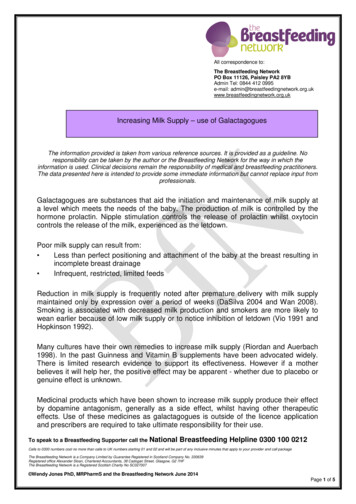
Biological Nurturing (laid-back or semi-reclined position)Biological Nurturing is a mother-centred approach to breastfeeding initiation. It promotesmaternal postures that help an infant’s instinctive behaviours and primitive neonatal reflexes.Primitive neonatal reflexes refers to more than 50 unconditioned reflex responses, as well asspontaneous behaviours to environmental stimuli. Spontaneous behaviors or reflexes includestepping, crawling, rooting, sucking, swallowing, hand-to-mouth movements, and movementsof the head, cheek, tongue, and lips (Colson et al., 2008).Biological Nurturing supports positive baby-led breastfeeding behaviours in infants whichallows them to actively participate in latching. This position can be used at any time duringbreastfeeding and works well with baby-led latching (Colson, 2010).This approach suggests that the mother: L ean back, somewhatsemi-reclined, finding anangle that feels right for her. I s relaxed and supported. D ress the infant lightly orpractice safe skin-to-skinwith both infant shoulderstouching the mother andthe infant chest expanded. P lace infant tummy downand in full contact with themother’s semi-reclined body.Across breastsSupported at mother’s sideOver the shoulderBelow breasts C uddle or nest the infantwith her arms. L et gravity support theinfant; there is no need toapply pressure along theinfant’s back or neck tokeep the infant in place(Colson, 2015). L atch the infant anywherealong the 360 circle of thebreast. See the illustrationsfor ideas.Illustrations adapted with permission from NancyMohrbacher.comSee a video at www.biologicalnurturing.com/video/bn3clip.html. In the video, notice: H ow comfortable the mother is. T he infant is in a light stage of sleep. H ow the mother follows the infant’s cues.2Breastfeeding Protocol: Positioning and Latching
Benefits of Biological Nurturing Allows for self-attachment (baby-ledlatching). Infants may latch on more quickly andwith ease (Colson, 2010).Considerations May or may not work for some womenwith extremely large breasts (Riordan,2016). Provides good support for the infant andrelaxation for the mother (Riordan, 2016). Works well for term and late preterminfants (Walker, 2014). May be an effective position for infantswith tongue tie, since gravity assists inmoving the tongue down and forward(Walker, 2014).Techniques to Support Effective Latching Affirm what works for the mother and infant. When something is not working, offer alternativesuggestions. Assess positioning and latching multiple times before hospital discharge and when any breastfeeding challenges occur. The Breastfeeding Committee for Canada (BCC) recommends that most teaching andbreastfeeding support be done in a hands-off manner. This allows a mother to latch the infantindependently, which can improve maternal self-confidence (BCC, 2017).Principles of Achievingan Effective Latch3Rationale Mother is relaxed and infant is in aquiet alert state. Both are positionedcomfortably. Promotes and optimizes infant feedingbehaviours. Mother holds infant tucked in closetummy-to-mommy, and preferablyskin-to-skin. Safe skin-to-skin contact has manybenefits for both mothers and newbornswhich include the promotion ofmother-infant attachment and initiationof early breastfeeding (Lau et al., 2017).See Initiation of Breastfeeding Protocol.Breastfeeding Protocol: Positioning and Latching
Principles of Achievingan Effective Latch Infant is well supported with mother’shand behind the shoulders, supportingthe neck, not the head. The infant’s handscan remain free to explore the mother’sbreasts and assist with latching.Rationale Provides positional and core stability neededto facilitate the infant’s instinctive behavioursand ability to self-attach. Allows the infant’s head to extend freely intoa sniffing position. Pushing on the back of the infant’s head mayblock the infant nose and make it difficult tobreathe. Pushing on the head may result inthe infant arching away from the breast, bitingthe nipple, or coming off the breast. Pushingthe head can also disturb the placement ofthe tongue when latching, encouraging it toelevate rather than cupping and moving downand forward (Walker, 2014). Infant’s nose approaches the nipple(nose-to-nipple as a landmark). Infantcan lick, search, and peck for the nipple. Stabilized on mother’s body, healthyinfants will lift their head, and use their mouthto search for the nipple. Aligning the infant’s nose to the mother’snipple allows for a deeper asymmetrical latch. With head in a slightly extended position,infants may touch the breast with theirchin, tongue, and cheek. This triggers awide open mouth. The touch of the infant’s face (cheeks, lips,or chin) on the breast, will, encourage theinfant to search, move, and centre theirmouth on the nipple. The infant will openthe lower jaw wide. Place the bottom lip andchin well below the nipple. This will appearasymmetrical, meaning it appears that morebreast is in the infant’s lower jaw than theupper jaw. Latching like this helps the infantto draw in a large mouthful of breast andnipple (Glover, 2018). This allows the nippleto be drawn further back in the infant’smouth where it will be more comfortable forthe mother. Mother may need to shape the breastwhile latching. May make it easier for the infant’s lower jawto take in more breast tissue and allow for adeeper latch. See Other Latching Techniques,page 7.See an animated latching video on many of these principles atwww.youtube.com/watch?v Rydwlle7jx4.4Breastfeeding Protocol: Positioning and Latching
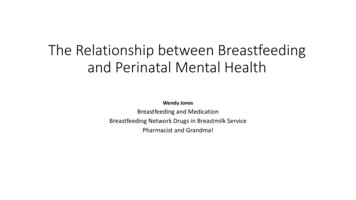
Signs of an Effective Latch I nfant’s mouth is opened wide. I nfant’s lips are curled out. M ore areola may be visible above theinfant’s upper lip than below. I nfant’s head is slightly extended. Whenthe head is back, the nose is free (notburied into the breast). The infant’s chinis pressed into the breast. During suckling:–T he infant’s cheeks remain full and rounded,not dimpling or indrawn.–M other feels a tugging sensation when infantsuckles, with no pain. There may be someinitial discomfort from suckling but not aftera letdown. If pain persists, reassess the latch.–A ctive sucking and swallowing of breastmilk may be heard (audible swallowing or“kah” sounds). Seeing a suck-pause-swallowpattern generally indicates breast milk transfer. Breast softening and increasedinfant contentment following a feed, along with adequate diaper output, are signs ofeffective breast milk transfer. See Protocol called Signs of Effective Breastfeeding.– I nfant is comfortable, managing the flow of breast milk, and maintains the latch.– I nfant relaxes during the breastfeed and does not get tense or agitated. W hen the infant comes off the breast, the colour and shape of mother’s nipple remainsunchanged. Sometimes the nipple may be elongated, but not pinched or compressed. After a feed, the mother’s breast is softer than before the feed.See these helpful videos: w ng-your-baby h ttps://globalhealthmedia.org/videos/breastfeeding/ See: Attaching Your Baby at the Breast.This LATCH acronym helps to highlight what to look for in an effective latch.LATCHLIPSFLANGED OUT(Wide, gaping mouthto accommodateareola and nipple)ASYMMETRICLATCH(More areola visibleabove the baby’stop lip)TUMMY-TOMOMMY(Baby’s ears,shoulders, and hipsin alignment)CHIN TOUCHINGBREAST(Nose freein thesniffing position)HAVE A LISTEN& WATCH(Active suckling andswallowing indicatingmilk transfer)Adapted with permission from Baby-Friendly Council of Newfoundland and Labrador.Adapted with permission from Baby-Friendly Council of Newfoundland and Labrador.5Breastfeeding Protocol: Positioning and Latching
Infant-led LatchingAchieving an optimal latch is best when led by the infant. Baby-led latching is a naturaland intuitive way for the infant to find the breast. It can be used anytime in a laid-back orsemi-reclined position and is helpful when the infant is learning to breastfeed, is notbreastfeeding well, or when the mother’s nipples are sore. M other sits comfortably and leans back. I nfant is held safely, skin-to-skin onmother’s upper chest. A commonmethod is to put the infant betweenthe mother’s breasts, so that the infant’sshoulders and hips are stable, andthe infant’s head can tilt back slightlyinto a sniffing position.12 Infant will start moving their head up and down looking formother’s breast. This may look like bobbing or pecking. Infant will seek the breast and try moving towards the breast,sometimes making crawling motions. Mother supports the infant’s shoulders, neck and buttocks,assisting the infant while they moves towards the breast.3 I nfant will find mother’s nipple. I nfant will push their chin into mother’s breast, reach upwith a wide open mouth and latch onto the breast. O nce infant is attached, mother and infant can adjustto each other to find a comfortable position. M other can bring the infant’s bottom close to mother’sbody and support the infant’s back and shoulders.6Breastfeeding Protocol: Positioning and Latching
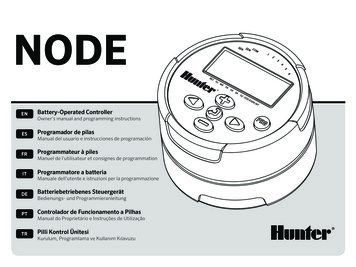
1Other Latching TechniquesBreast-shaping techniques may be used to assist the infant in getting a bigger mouthful of thebreast, so the nipple can extend farther back into the infant’s mouth. Nipple tilting and breastsandwich are two breast-shaping techniques that some practitioners use to help mothers andinfants (Mohrbacher, 2010).1Nipple tiltingThis technique was originally described byRebecca Glover. Some call it the flipple.Using nipple tilting can make it easier for theinfant’s lower jaw to create a deeper latch.12To do nipple tilting: I nfant is aligned and well supported. M other presses on the breast near thenipple with a thumb or finger. The mother’sthumb (or finger), the nipple, and theinfant’s upper lip are in alignment. T he thumb or finger causes the nippleto point up and away from the infant.This rounds out the areola providingmore surface area for the infant to latch. T he mother brings the infant’s lowerjaw or chin into contact with the skin.Once in skin contact, the infant’s mouthreflexively opens wide. The mother thenrolls the rounded side of the areola intothe infant’s open mouth to create adeep latch. The mother then watchesfor swallowing (Mohrbacher, 2010).223337Breastfeeding Protocol: Positioning and Latching
Breast sandwich M other may support and shape thebreast to get more breast tissue intothe infant’s mouth by gently squeezingor compressing the breast from topto bottom or side-to-side.1 W ith the mother’s fingers on one side,thumb on the other, away from the areola,the mother can shape the breast. Thefingers will be parallel to the infant’s lowerlips, forming a “breast sandwich” (Wiessinger, 1998). I nfant is aligned and well supported ina tummy-to-mommy position.2 I nfant’s head is slightly extended. M other is encouraged to touch the breastto the infant’s mouth, and then wait forthe mouth to open wide. Or, a mothermay support the infant until the chintouches the breast and the infant’s mouthopens wide (like a yawn). T o latch, the mother brings the infantclose to the breast by gently pulling theinfant’s shoulders, upper back andbuttocks closer. Encourage the motherto avoid leaning over or pushing theinfant’s head. S upporting the infant’s upper back andneck can help keep the infant’s neck inslight extension. O nce the infant is latched, mother andinfant can reposition themselves sothey are both comfortable. Ensure themother’s shoulders are relaxed.8Breastfeeding Protocol: Positioning and Latching3
Dancer hand-hold, for special circumstancesThis position may be used if the infant is able to achieve butnot maintain a latch, for example, for infants with low muscletone or weak muscle development. T he infant is held in an upright sitting position facing themother’s breast. T he mother first supports the breast in a variation ofa “U” hold. The mother cups the breast with her palmand three fingers. T he mother supports the infant’s chin in the area ofher hand between the thumb and index finger. T he mother gently supports the infant’scheek on one side with the indexfinger and the thumb on theother cheek. T o avoid triggering a rootingreflex, the mother usesgentle, steady, and equalpressure in the infant’s cheeks.This provides steady supportto the infant’s jaws and chinto help maintain the latch(Lauwers & Swisher, 2011).9Breastfeeding Protocol: Positioning and Latching
Practices That May CreateChallengesMother lifts the breast when latching. W hen the breast is released, thereis a risk that the weight of the breastwill pull some of the breast out of theinfant’s mouth. C an cause a shallow latch, resulting inpoor breast milk transfer and nipplepain.Mother holds the breast firmly or indentsit with her thumb or fingers throughouta feed. This is commonly seen with theintention to help an infant breathe better. M ay contribute to blocked ducts.Infant slips off the breast or makes clickingnoises.Practices to Prevent orTroubleshoot Latching Challenges K eep infant and mother’s breast at thesame level. B ring infant to where mother’s breastnaturally falls. “Breastfeed at the anglethat you dangle” (K. Venter, personalcommunication). F or larger breasts, a rolled up towel maybe placed under the breast for support(Walker, 2014), or mothers may use theirhand to support the weight of the breast.Different positions may also be tried. R eposition infant to ensure head is slightlyextended back, with the nose free, and chinpressed into the breast. H old and shape breast gently. H old breast less firmly after latching toensure mother is not compressing ductsor blocking breast milk flow. E nsure a deep latch, use a breast-shapingtechnique (see Biological Nurturing, page2, Nipple tilting, page 7, or Breast sandwich,page 8). A ssess breast milk transfer and mother’sbreast milk supply. O ral assessment may be required to ruleout any concerns regarding infant’s oralanatomy e.g., tongue tie.10Breastfeeding Protocol: Positioning and Latching
How to Unlatch an InfantOften infants will come off the breast on theirown and do not need to be unlatched.If the mother wishes to remove the latched-oninfant, the mother can break the suctionas follows: G ently insert a clean finger into thecorner of the infant’s mouth andbetween the gums (see illustration). M other’s may optionally gently pulldown on the infant’s chin to unlatch. E ither way, allow the nipple to gentlycome out of the infant’s mouth.Simply pulling the nipple out ofthe infant’s mouth while latchedcan cause nipple damage and isbest to avoid.Other BreastfeedingPositionsThere are many breastfeeding positions a mothermay use. Whatever position a mother prefers(e.g., laid-back, sitting up or lying down), the infantshould be well-supported allowing for a deep latchand ease of swallowing. Along with BiologicalNurturing or laid-back position (see page 2), themost commonly taught positions are: C ross-cradle. C radle. F ootball. S ide-lying.11Breastfeeding Protocol: Positioning and Latching
Cross-cradle Position(May be used for either breast. This description is for the left breast.)Refer to Principles of Positioning on page 1. M other’s right arm holds infant along theirspine. M other’s right hand supports infant’s shouldersand neck. The mother’s forearm supports theinfant’s back and bottom. M other can hold the breast with her left hand.See Other Latching Techniques, page 7. Mother observes signs of an effective latch.See page 5. O nce infant is latched, mother may shift to adifferent position (e.g., cradle position).Benefits I nfant is tucked close to the mother. Thishelps the infant to achieve a large mouthon the breast and a comfortable latch. M other’s arms may tire from infant’sweight. P rovides good head and neck control.This makes it easier to bring the infant tothe breast (Riordan, 2016). M other can hold the infant using a pillowor blanket to support the mother’s arms;paying attention to her wrist and elbowsupport. W orks well for mothers and infantslearning to breastfeed. S ome mothers may be less familiar withthis hold. W orks for infants who are term, preterm,and small or have low muscle tone. W orks well for infants who have a weakrooting reflex or suck.12ConsiderationsBreastfeeding Protocol: Positioning and Latching
Cradle Position(May be used for either breast. This description is for the left breast.)Refer to Principles of Positioning on page 2. Mother holds infant in the left arm, with theinfant’s head near her elbow. Mother’s lefthand holds the infant’s bottom. M other may support the left breast with theright hand. M other observes signs of an effective latch.See page 5.Benefits13Considerations W orks when mother is comfortablebreastfeeding and infant is latching well. W hen learning to breastfeed, this positionmay be more challenging. M other may feel comfortable andconfident holding the infant in this way.This is a common position and mayseem familiar. M other may feel she has minimal controlover the infant’s head.Breastfeeding Protocol: Positioning and Latching M ay have difficulty achieving a deep latch. G enerally avoid this position with earlyor late preterm infants as these infantsoften have low muscle tone. In addition,positions that place the late preterminfant’s neck and body in excessive flexionmakes them prone to positional apneadue to airway obstruction. This increasesthe risk of bradycardia and oxygendesaturation (Walker, 2014).
Football PositionMother places infant at her side and scoops theinfant up with the forearm, tucking the infantat her side. I nfant is lying on their back, looking up at theirmother, or turned to varying degrees, lookingat the mother’s side. I nfant’s legs and feet are facing towards theback of the chair. P osition infant back far enough so the infant’shead can extend into a sniffing position.This allows room between the infant’s chinand chest and helps achieve a deeper latch(Riordan, 2016). M other’s hand will be behind infant’sshoulder and neck, supporting theinfant’s upper back. M other’s other hand can support thebreast. L atch infant.Benefits M ay be comfortable for mothers after acaesarean birth. W orks well when learning to breastfeedand if the infant has difficulty maintaininga latch. W orks well if infant is preterm or small,has low muscle tone, weak rooting reflexor suck. M ay help mothers with larger breasts. M ay help mothers with sore nipples. I s an option for feeding twins at the sametime. Breastfeeding Multiples, page 16.14Breastfeeding Protocol: Positioning and LatchingConsiderations P illows can be used behind the mothersback and beside her to support her armand infant. M any mothers place the infant’s headtoo far forward for the infant to latch in asniffing position. M ay be more challenging as infant grows. M ay be difficult for some mothers to seethe infant’s mouth to latch. W atch if the weight of a large breas
Josdalyne Anderson MD Eastern Monarch Centre, Independent Practice Pamela Drynan PHN North East Timmins & District Hospital, & Independent Practice Laura Dueck RN, PHN South West Middlesex-London Health Unit Danit Fischtein MD, IBCLC Central Well Medica Medical Centre, Brampton Susan Hayward MD, FCFP, FABM Central Queen Square Family