Transcription
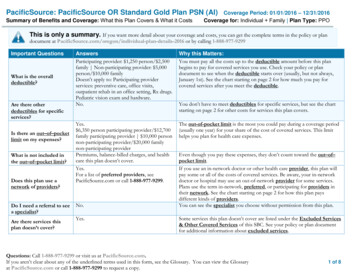
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Summary of Benefits and Coverage: What this Plan Covers & What it CostsCoverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPOThis is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plandocument at 016 or by calling 1-888-977-9299Important QuestionsWhat is the overalldeductible?Are there otherdeductibles for specificservices?Is there an out–of–pocketlimit on my expenses?What is not included inthe out–of–pocket limit?Does this plan use anetwork of providers?Do I need a referral to seea specialist?Are there services thisplan doesn’t cover?AnswersParticipating provider: 1,250 person/ 2,500family Non-participating provider: 5,000person/ 10,000 familyDoesn’t apply to: Participating providerservices: preventive care, office visits,outpatient rehab in an office setting, Rx drugs.Pediatric vision exam and hardware.No.Why this Matters:You must pay all the costs up to the deductible amount before this planbegins to pay for covered services you use. Check your policy or plandocument to see when the deductible starts over (usually, but not always,January 1st). See the chart starting on page 2 for how much you pay forcovered services after you meet the deductible.Yes. 6,350 person participating provider/ 12,700family participating provider 10,000 personnon-participating provider/ 20,000 familynon-participating providerPremiums, balance-billed charges, and healthcare this plan doesn’t cover.Yes.For a list of preferred providers, seePacificSource.com or call 1-888-977-9299.The out-of-pocket limit is the most you could pay during a coverage period(usually one year) for your share of the cost of covered services. This limithelps you plan for health care expenses.No.Yes.You don’t have to meet deductibles for specific services, but see the chartstarting on page 2 for other costs for services this plan covers.Even though you pay these expenses, they don’t count toward the out–of–pocket limit.If you use an in-network doctor or other health care provider, this plan willpay some or all of the costs of covered services. Be aware, your in-networkdoctor or hospital may use an out-of-network provider for some services.Plans use the term in-network, preferred, or participating for providers intheir network. See the chart starting on page 2 for how this plan paysdifferent kinds of providers.You can see the specialist you choose without permission from this plan.Some services this plan doesn’t cover are listed under the Excluded Services& Other Covered Services of this SBC. See your policy or plan documentfor additional information about excluded services.Questions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.1 of 8
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPOCo-payments are fixed dollar amounts (for example, 15) you pay for covered health care, usually when you receive the service.Co-insurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, ifthe plan’s allowed amount for an overnight hospital stay is 1,000, your co-insurance payment of 20% would be 200. This may change ifyou haven’t met your deductible.The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than theallowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges 1,500 for an overnight stay andthe allowed amount is 1,000, you may have to pay the 500 difference. (This is called balance billing.)This plan may encourage you to use participating providers by charging you lower deductibles, co-payments and co-insurance amounts.CommonMedical EventIf you visit ahealth careprovider’s officeor clinicServices You May NeedYour cost if you usea ParticipatingProviderPrimary care visit to treat an injury orillness 20 co-pay/visitSpecialist visit 40 co-pay/visitOther practitioner office visitPreventivecare/screening/immunizationNot coveredYour cost if youuse a NonparticipatingProviderDeductible then 55%co-insuranceDeductible then 55%co-insuranceNot coveredDeductible then 55%co-insuranceNo chargeTobacco Cessation: NotcoveredDiagnostic test (x-ray, blood work)If you have a testImaging (CT/PET scans, MRIs)If you need drugsto treat yourillness orDeductible then 10% coinsuranceDeductible then 10% coinsuranceRetail: 10 co-payMail:Deductible then 55%co-insuranceDeductible then 55%co-insuranceLimitations & Exceptions---none-----none--Not covered.Limited to: Routine Physicals: 13 visitsages 0-36 months, annually ages 3 andolder. Well Woman Visits: annually.Immunizations: CDC and USPSTFPreventive Care Grade A and BRecommended. PreventiveColonoscopy: Ages 50-75. High RiskColonoscopy: Under age 50.---none--Pre-authorization required.Deductible then 90%co-insuranceRetail limited to 30 day supply. Maillimited to 90 day supply. Preauthorization required for certain drugs.Questions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.2 of 8Generic drugs
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Summary of Benefits and Coverage: What this Plan Covers & What it CostsconditionMore informationabout prescriptiondrug coverage isavailable atPacificSource.com.Preferred brand drugsNon-preferred brand drugsSpecialty drugsIf you haveoutpatient surgeryFacility fee (e.g., ambulatory surgerycenter)Physician/surgeon feesEmergency room servicesIf you needimmediatemedical attention 20 co-payRetail: 30 co-payMail: 90 co-payRetail:50% co-insuranceMail:50% co-insuranceCoverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPODeductible then 90%co-insuranceSee Generic drugs above.Deductible then 90%co-insuranceSee Generic drugs above.50% co-insuranceDeductible then 90%co-insuranceParticipating provider benefit availableonly through our specialty pharmacyservices provider. Limited to 30 daysupply. Pre-authorization required forcertain drugs.Deductible then 10% coinsuranceDeductible then 10% coinsuranceMedical Emergency:Deductible then 10% coinsuranceNon-Emergency:Deductible then 10% coinsuranceDeductible then 55%co-insuranceDeductible then 55%co-insuranceMedical Emergency:Deductible then 10%co-insuranceNon-Emergency:Deductible then ible then 10% coinsuranceDeductible then 10%co-insuranceLimited to nearest facility able to treatcondition. Air covered if groundmedically or physically inappropriate.Non-participating air covered up to200% of Medicare allowance. 60 co-pay/visitDeductible then 55%co-insurance---none---Deductible then 10% coinsuranceDeductible then 55%co-insuranceLimited to semi-private room unlessintensive or coronary care units,medically necessary isolation, or hospitalQuestions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.3 of 8Emergency medical transportationUrgent careIf you have ahospital stayFacility fee (e.g., hospital room)
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Summary of Benefits and Coverage: What this Plan Covers & What it CostsCoverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPOonly has private rooms. Preauthorization required for someinpatient services.Physician/surgeon feeIf you havemental health,behavioral health,or substanceabuse needsMental/Behavioral health outpatientservicesMental/Behavioral health inpatientservicesSubstance use disorder outpatientservicesSubstance use disorder inpatientservicesPrenatal and postnatal careIf you arepregnantIf you need helprecovering orhave other specialhealth needsDeductible then 10% coinsurance 20 co-pay/visitDeductible then 10% coinsurance 20 co-pay/visitDeductible then 10% coinsuranceDeductible then 10% coinsuranceDeductible then 55%co-insuranceDeductible then 55%co-insuranceDeductible then 55%co-insuranceDeductible then 55%co-insuranceDeductible then 55%co-insuranceDeductible then 55%co-insuranceDelivery and all inpatient servicesDeductible then 10% coinsuranceDeductible then 55%co-insuranceHome health careDeductible then 10% coinsuranceDeductible then 55%co-insuranceInpatient:Deductible then 10% coinsuranceRehabilitation servicesHabilitation servicesOutpatient: 20 copay/visit if provided inan office setting, all othersettings Deductible then10% co-insuranceInpatient:Deductible then 10% co-Inpatient: Deductiblethen 55% co-insuranceOutpatient: Deductiblethen 55% co-insuranceInpatient:Deductible then 55%Questions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.---none-----none--Pre-authorization required.---none--Pre-authorization required.Preventive prenatal: No co-insurance.Practitioner delivery and hospital visitsare covered under prenatal and postnatalcare. Facility is covered the same as anyother hospital services. Coverageincludes termination of pregnancy.No coverage for private duty nursing orcustodial care. Pre-authorizationrequired.Inpatient: Covered up to a combined 30days/year, unless medically necessary totreat a mental health diagnosis. Preauthorization required.Outpatient: Covered up to 30visits/year, unless medically necessary totreat a mental health diagnosis.Preauthorization required. No coveragefor recreation therapy.Inpatient: Covered up to a combined 30days/year, unless medically necessary to4 of 8
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Summary of Benefits and Coverage: What this Plan Covers & What it CostsIf your childneeds dental oreye careCoverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPOinsuranceco-insuranceOutpatient: 20 copay/visit if provided inan office setting, all othersettings Deductible then10% co-insuranceOutpatient:Deductible then 55%co-insuranceSkilled nursing careDeductible then 10% coinsuranceDeductible then 55%co-insuranceDurable medical equipmentDeductible then 10% coinsuranceDeductible then 55%co-insuranceHospice serviceDeductible then 10% coinsuranceDeductible then 55%co-insuranceEye examNo charge50% co-insuranceGlassesNo charge50% co-insuranceNot coveredNot coveredDental check-upQuestions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.treat a mental health diagnosis. Preauthorization required.Outpatient: Covered up to 30visits/year, unless medically necessary totreat a mental health diagnosis.Preauthorization required. No coveragefor recreation therapy.Limited to 60 days/year. No coveragefor custodial care. Pre-authorizationrequired.Limited to: 5,000/year overall; preauthorization required for powerassisted wheelchairs; one pair/year forglasses or contact lenses to correct aspecific vision defect from a severemedical or surgical problem; one per earevery 48 months for hearing aid age 0-18(or age 0-25 if student); no coverage foradult hearing aids; and one breastpump/pregnancy. Pre-authorizationrequired if over 800.Pre-authorization required. No coveragefor private duty nursing.One routine eye exam per year forchildren 18 or younger when providedby a licensed provider.One pair of lenses and frames from thePediatric Exchange Collection per yearfor children 18 or younger. Additionalcoatings not covered.Not covered.5 of 8
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Summary of Benefits and Coverage: What this Plan Covers & What it CostsCoverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPOExcluded Services & Other Covered Services:Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.) Acupuncture Dental Care (Adult) Non-emergency care when traveling outside the U.S. Bariatric Surgery Dental Check-up(Child) Outpatient Recreational Therapy Chiropractic Care Hearing Aids (Adult) Private Duty Nursing Cosmetic Surgery (except in certain Infertility Treatment Routine Eye Care (Adult)situations) Long-term Care Routine foot care, other than with diabetes mellitus Custodial Care Massage TherapyOther Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for theseservices.) Hearing Aids (Child) Weight Loss ProgramsYour Rights to Continue Coverage:Federal and State laws may provide protections that allow you to keep this health insurance coverage as long as you pay your premium. There are exceptions,however, such as if: You commit fraud The insurer stops offering services in the State You move outside the coverage areaFor more information on your rights to continue coverage, contact the insurer at (888) 977-9299. You may also contact your state insurance department at (503)947-7984 or the toll free message line at (888) 877-4894; by writing to the Oregon Insurance Division, Consumer Protection Unit, 350 Winter Street NE, Salem,OR 97301-3883; through the Internet at /fileacomplaint.aspx; or by e-mail at: cp.ins@state.or.us.Your Grievance and Appeals Rights:If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions aboutyour rights, this notice, or assistance, you can contact: your state insurance department at (503) 947-7984 or the toll free message line at (888) 877-4894; by writingto the Oregon Insurance Division, Consumer Protection Unit, 350 Winter Street NE, Salem, OR 97301-3883; through the Internet es/fileacomplaint.aspx; or by e-mail at: cp.ins@state.or.us.Does this Coverage Provide Minimum Essential Coverage?The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage”. This plan or policy does provideminimum essential coverage.Does this Coverage Meet the Minimum Value Standard?The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This healthcoverage does meet the minimum value standard for the benefits it provides.Language Access Services:Spanish (Español): Para obtener asistencia en Español, llame al �––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next –––––––Questions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.6 of 8
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Coverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPOCoverage ExamplesAbout these CoverageExamples:These examples show how this plan might covermedical care in given situations. Use theseexamples to see, in general, how much financialprotection a sample patient might get if they arecovered under different plans.This isnot a costestimator.Don’t use these examples toestimate your actual costsunder this plan. The actualcare you receive will bedifferent from theseexamples, and the cost ofthat care will also bedifferent.See the next page forimportant information aboutthese examples.Having a babyManaging type 2 diabetes(normal delivery)(routine maintenance ofa well-controlled condition) Amount owed to providers: Plan pays Patient pays 7,540 5,520 2,020Sample care costs:Hospital charges (mother)Routine obstetric careHospital charges (baby)AnesthesiaLaboratory testsPrescriptionsRadiologyVaccines, other preventiveTotal 2,700 2,100 900 900 500 200 200 40 7,540Patient pays:DeductiblesCo-paysCo-insuranceLimits or exclusionsTotal 1,250 20 600 150 2,020American Indian and Native American Benefits: If you are a Native American enrolled onthis plan and receive services directly from the Indian Health Service, Indian Tribe, TribalOrganizations, or Urban Indian Organization, or through referral under the contract healthservices, the services will not be subject to any Deductible, Copayments, or Coinsurance. Amount owed to providers: Plan pays Patient pays 5,400 3,500 1,900Sample care costs:PrescriptionsMedical Equipment and SuppliesOffice Visits and ProceduresEducationLaboratory testsVaccines, other preventiveTotal 2,900 1,300 700 300 100 100 5,400Patient pays:DeductiblesCo-paysCo-insuranceLimits or exclusionsTotal 1,250 460 110 80 1,900Note: These numbers assume the patient isparticipating in our diabetes wellness program. Ifyou have diabetes and do not participate in thewellness program, your costs may be higher. Formore information about the diabetes wellnessprogram, please contact: 1-888-977-9299.Questions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.7 of 8
PacificSource: PacificSource OR Standard Gold Plan PSN (AI)Coverage ExamplesCoverage Period: 01/01/2016 – 12/31/2016Coverage for: Individual Family Plan Type: PPOQuestions and answers about the Coverage Examples:What are some of theassumptions behind theCoverage Examples? Costs don’t include premiums.Sample care costs are based on nationalaverages supplied by the U.S.Department of Health and HumanServices, and aren’t specific to aparticular geographic area or health plan.The patient’s condition was not anexcluded or preexisting condition.All services and treatments started andended in the same coverage period.There are no other medical expenses forany member covered under this plan.Out-of-pocket expenses are based onlyon treating the condition in the example.The patient received all care from innetwork providers. If the patient hadreceived care from out-of-networkproviders, costs would have been higher.What does a Coverage Exampleshow?Can I use Coverage Examplesto compare plans?For each treatment situation, the CoverageExample helps you see how deductibles, copayments, and co-insurance can add up. Italso helps you see what expenses might be leftup to you to pay because the service ortreatment isn’t covered or payment is limited. Yes. When you look at the Summary ofDoes the Coverage Examplepredict my own care needs? No. Treatments shown are just examples.The care you would receive for thiscondition could be different based on yourdoctor’s advice, your age, how serious yourcondition is, and many other factors.Does the Coverage Examplepredict my future expenses? No. Coverage Examples are not costestimators. You can’t use the examples toestimate costs for an actual condition. Theyare for comparative purposes only. Yourown costs will be different depending onthe care you receive, the prices yourproviders charge, and the reimbursementyour health plan allows.Benefits and Coverage for other plans,you’ll find the same Coverage Examples.When you compare plans, check the“Patient Pays” box in each example. Thesmaller that number, the more coveragethe plan provides.Are there other costs I shouldconsider when comparingplans? Yes. An important cost is the premiumyou pay. Generally, the lower yourpremium, the more you’ll pay in out-ofpocket costs, such as co-payments,deductibles, and co-insurance. Youshould also consider contributions toaccounts such as health savings accounts(HSAs), flexible spending arrangements(FSAs) or health reimbursement accounts(HRAs) that help you pay out-of-pocketexpenses.Questions: Call 1-888-977-9299 or visit us at PacificSource.com.If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossaryat PacificSource.com or call 1-888-977-9299 to request a copy.8 of 8
PacificSource OR Standard Plan PSN Individual Medical PolicymPacificSource Health PlansplePolicyPacificSource Health Plans, herein called PacificSource, will pay the benefits of this IndividualMedical Policy (‘policy’ herein) for covered losses in accordance with the policy provisions.The term of this policy is from month to month and is guaranteed renewable as long as requiredpremiums are paid. We will renew this policy annually on January 1st of each year, subject totermination for any of the reasons stated under General Policy Provisions.PacificSource may change the premiums or other provisions of this policy as allowed by state law. Ifpremiums or other policy provisions are changed, PacificSource will give the policyholder at least 60days written notice before the change becomes effective. Failure on the part of the policyholder topay premium after notice of a change will mean the policyholder terminates this policy as of theeffective date of the change. The policyholder may deposit premium in advance, but doing so will notextend the policy term or limit the right of PacificSource to change the premium. PacificSource willmake no change in premium or policy provisions unless the same change is made to all policies ofthe same form and class.This policy you are applying for does not include coverage for pediatric dental care, which isconsidered an essential health benefit under the Affordable Care Act. Pediatric dental care isavailable in the market and can be purchased as a stand-alone product. Please contact yourinsurance agent, your health insurance company, or your state’s insurance exchange if you wish topurchase a stand-alone dental care product.This policy is issued in consideration of payment of the initial premium and of the application, a copyof which is attached to and made part of this policy.IN WITNESS WHEREOF, PacificSource has caused this policy to be executed as of 12:00:01 a.m.local time on the policy effective date.SaBy:Kenneth P. ProvencherPresident, CEOPlease read the policy carefully. If you are not satisfied with the policy for any reason, it may bereturned to PacificSource within ten days after receipt and any premium paid will be refunded.POLICY INFORMATIONPolicyholder: Sample PolicyholderAdditional Insured Persons:Policy Number:Policy Effective Date:Monthly Premium:Date of Issue:PacificSource Health Plans HeadquartersPacificSource Customer Service DepartmentPO Box 7068, Springfield, OR 97475-0068Phone (541) 684-5582 or (888) 977-9299Website: PacificSource.comEmail cs@pacificsource.comPara asistirle en español, por favor llame al numero (800) 624-6052, extensión 5456PSIP.OR.0116
CONTENTSSCHEDULE OF BENEFITS .AADMINISTRATIVE PROVISIONS . 1ELIGIBILITY . 1OPEN ENROLLMENT . 3EFFECTIVE DATE OF COVERAGE . 3PREMIUM . 3GENERAL POLICY PROVISIONS . 4USING THE PROVIDER NETWORK . 6yPARTICIPATING PROVIDERS. 6NON-PARTICIPATING PROVIDERS . 7FINDING PARTICIPATING PROVIDER INFORMATION . 9licCOVERED EXPENSES . 10mplePoPLAN BENEFITS . 11PREVENTIVE CARE SERVICES . 12PEDIATRIC SERVICES . 15PROFESSIONAL SERVICES . 16HOSPITAL AND SKILLED NURSING FACILITY SERVICES . 17OUTPATIENT SERVICES . 18EMERGENCY SERVICES . 19MATERNITY SERVICES. 20MENTAL HEALTH AND CHEMICAL DEPENDENCY SERVICES . 21HOME HEALTH AND HOSPICE SERVICES . 22DURABLE MEDICAL EQUIPMENT . 24TRANSPLANT SERVICES . 25PRESCRIPTION DRUGS . 27OTHER COVERED SERVICES, SUPPLIES, AND TREATMENTS. 30SaBENEFIT LIMITATIONS AND EXCLUSIONS . 34EXCLUDED SERVICES . 34PREAUTHORIZATION . 43CASE MANAGEMENT . 44INDIVIDUAL BENEFITS MANAGEMENT . 44UTILIZATION REVIEW . 45CLAIMS PAYMENT . 46COORDINATION OF BENEFITS . 48THIRD PARTY LIABILITY . 50COMPLAINTS, GRIEVANCES, AND APPEALS . 52GRIEVANCE PROCEDURES . 52APPEAL PROCEDURES . 52HOW TO SUBMIT GRIEVANCES OR APPEALS . 54RESOURCES FOR INFORMATION AND ASSISTANCE . 55FEEDBACK AND SUGGESTIONS . 56PSIP.OR.0116
RIGHTS AND RESPONSIBILITIES . 56PRIVACY AND CONFIDENTIALITY . 58PLAN ADMINISTRATION . 58SamplePolicyDEFINITIONS . 58PSIP.OR.0116
SCHEDULE OF BENEFITSSamplePolicySchedule of Benefits for Medical, Pharmacy, and Vision would be inserted here. See websitefor plan specific schedules.PSIP.OR.0116A
ADMINISTRATIVE PROVISIONSThis policy, including endorsements, addendums, and any other attached papers, if any,constitutes the entire contract of insurance. No change in this policy is valid unless approvedby an executive officer of PacificSource and unless such approval is endorsed hereon orattached hereto. No agent has the author
1 of 8 PacificSource: PacificSource OR Standard Gold Plan PSN (AI) Coverage Period: 01/01/2016 - 12/31/2016 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual Family Plan Type: PPO Questions: Call 1-888-977-9299 or visit us at PacificSource.com. If you aren't clear about any of the underlined terms used in this form, see the Glossary.