Transcription
Glucagon-Like Peptide (GLP-1)Receptor Agonists Clinical EditCriteriaDrug/Drug Class:Glucagon-Like Peptide-1 (GLP-1) Receptor AgonistsSuperior HealthPlan follows the guidance of the Texas Vendor Drug Program (VDP)for all clinical edit criteria. Superior has adjusted the clinical criteria to ease the priorauthorization process regarding this clinical edit. The criteria logic step 7 (CPTcodes for ESRD) and 8 (requirement for documentation of HgbA1c from previous180 days) have been removed. Any changes to VDP criteria are noted in yellowhighlight within the criteria and diagram.The original clinical edit can be referenced at the Texas Vendor Drug Program websitelocated at rization/mco-clinical-pa.Clinical Edit Information Included in this Document:Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Drugs requiring prior authorization: the list of drugs requiring prior authorization for this clinicalcriteria.Prior authorization criteria logic: a description of how the prior authorization request will beevaluated against the clinical criteria rules.Logic diagram: a visual depiction of the clinical edit criteria logic.Diagnosis codes or drugs in step logic: a list of diagnosis codes or drug information and additionalstep logic, claims and lookback period information.Supporting tables: a collection of information associated with the steps within the criteria(diagnosis codes, procedure codes, and therapy codes); provided when applicableClinical Edit References: clinical edit references as provided by the Texas Vendor Drug Program.Publication history: to track when the eased criteria was put into production and any updatessince this time.Please note: All tables are provided by original Texas Vendor Drug Program Edit.
Drugs Requiring Prior Authorization GLP-1 Receptor Agonists:Label NameDrugs Requiring Prior AuthorizationGCNADLYXIN 10-20 MCG STARTER PACKADLYXIN 20 MCG MAINTENANCE PKBYDUREON 2 MG VIALBYDUREON 2 MG PEN INJECTBYDUREON BCISE 2 MGAUTOINJECTBYETTA 5 MCG DOSE PEN INJBYETTA 10 MCG DOSE PEN INJOZEMPIC 0.25-0.5 MG DOSE PENOZEMPIC 1 MG DOSE PENSOLIQUA 100 UNIT-33 MCG/ML PENTRULICITY 0.75 MG/0.5 ML PENTRULICITY 1.5 MG/0.5 ML PENVICTOZA 18 MG/3 ML PENXULTOPHY 100 UNIT-3.6 MG/ML 67637169371712618938348The listed GCNS may not be an indication of Texas Medicaid Formulary coverage. To review thecurrent formulary coverage, please visit orHealthPlan.comSHP 20194847Page 2 of 16
Superior HealthPlan Clinical Criteria Logic GLP-1 Receptor Agonists:1. Is the client greater than or equal to ( ) 18 years of age?[ ] Yes (Go to #3)[ ] No (And request is for Victoza, go to #2)[ ] No (And request is for any agent other than Victoza, Deny)2. Is the client greater than or equal to ( ) 10 years of age?[ ] Yes (Go to #3)[ ] No (Deny)3. Does the client have a diagnosis of type 2 diabetes in the last 365 days?[ ] Yes (Go to #4)[ ] No (Deny)4. Does the client have a history of an oral antidiabetic agent for 14 days in the last 365 days?[ ] Yes (Go to #6)[ ] No (Go to #5)5. Does the client have a history of the requested medication for 14 days in the last 365 days?[ ] Yes (Go to #6)[ ] No (Deny)6. Does the client have a history of ESRD, chronic kidney disease (stage IV and V), pancreatitis, orgastroparesis in the last 730 days?[ ] Yes (Deny)[ ] No (Approve – 365 days)7. Does the client have a history of ESRD services (CPT codes) in the last 730 days?[ ] Yes (Deny)[ ] No (Go to #7)8. Does the client have a history of an HbA1c test in the last 180 days?[ ] Yes (Approve – 365 days)[ ] No (Deny)SuperiorHealthPlan.comSHP 20194847Page 3 of 16
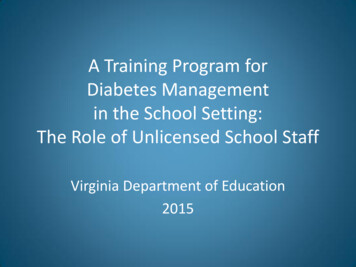
Superior HealthPlan Clinical Edit Logic Diagram GLP-1 ReceptorAgonists:No, and request is forany agent other thanVictozaStep 1Is the client greater than orequal to 18 years of age?Deny requestNo, and request isfor VictozaYesStep 2Is the client greater than orequal to 10 years of age?NoYesNoStep 3Does the client have a diagnosisof type 2 diabetes in the last 365Yesdays?Deny requestYesStep 4Does the client have a history ofan oral antidiabetic agent for 14days in the last 365 days?NoStep 5YesDoes the client have a historyof the requested medication for14 days in the last 365 days?NoDeny requestDenyYesYesStep 6Does the client have a history of ESRD,chronic kidney disease (stage IV and V),pancreatitis, or gastroparesis in the last730 days?NoApprove – 365 daysYesDeny requestPlease Note: Step 7 (regarding CPT codes for ESRD) andstep 8 (requirement for documentation of Hgb A1c fromprevious 180 days) have been removed.SuperiorHealthPlan.comSHP 20194847Page 4 of 16Deny request
Clinical Criteria Supporting Tables GLP-1 Receptor Agonists:ICD-10 1140E1141E1142Step 2 (diagnosis of type II diabetes)Required diagnosis: 1Look back timeframe: 365 daysDescriptionTYPE 2 DIABETES MELLITUS WITH HYPEROSMOLARITY WITHOUTNONKETOTIC HYPERGLYCEMIC-HYPEROSMOLAR COMA (NKHHC)TYPE 2 DIABETES MELLITUS WITH HYPEROSMOLARITY WITHCOMATYPE 2 DIABETES MELLITUS WITH DIABETIC NEPHROPATHYTYPE 2 DIABETES MELLITUS WITH DIABETIC CHRONIC KIDNEYDISEASETYPE 2 DIABETES MELLITUS WITH OTHER DIABETIC KIDNEYCOMPLICATIONTYPE 2 DIABETES MELLITUS WITH UNSPECIFIED DIABETICRETINOPATHY WITH MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH UNSPECIFIED DIABETICRETINOPATHY WITHOUT MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH MILD NONPROLIFERATIVEDIABETIC RETINOPATHY WITH MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH MILD NONPROLIFERATIVEDIABETIC RETINOPATHY WITHOUT MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH MODERATENONPROLIFERATIVE DIABETIC RETINOPATHY WITH MACULAREDEMATYPE 2 DIABETES MELLITUS WITH MODERATENONPROLIFERATIVE DIABETIC RETINOPATHY WITHOUTMACULAR EDEMATYPE 2 DIABETES MELLITUS WITH SEVERE NONPROLIFERATIVEDIABETIC RETINOPATHY WITH MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH SEVERE NONPROLIFERATIVEDIABETIC RETINOPATHY WITHOUT MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH PROLIFERATIVE DIABETICRETINOPATHY WITH MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH PROLIFERATIVE DIABETICRETINOPATHY WITHOUT MACULAR EDEMATYPE 2 DIABETES MELLITUS WITH DIABETIC CATARACTTYPE 2 DIABETES MELLITUS WITH OTHER DIABETIC OPHTHALMICCOMPLICATIONTYPE 2 DIABETES MELLITUS WITH DIABETIC NEUROPATHY,UNSPECIFIEDTYPE 2 DIABETES MELLITUS WITH DIABETIC MONONEUROPATHYTYPE 2 DIABETES MELLITUS WITH DIABETIC POLYNEUROPATHYSuperiorHealthPlan.comSHP 20194847Page 5 of 16
E118E119Step 2 (diagnosis of type II diabetes)Required diagnosis: 1Look back timeframe: 365 daysTYPE 2 DIABETES MELLITUS WITH DIABETIC AUTONOMIC(POLY)NEUROPATHYTYPE 2 DIABETES MELLITUS WITH DIABETIC AMYOTROPHYTYPE 2 DIABETES MELLITUS WITH OTHER DIABETICNEUROLOGICAL COMPLICATIONTYPE 2 DIABETES MELLITUS WITH DIABETIC PERIPHERALANGIOPATHY WITHOUT GANGRENETYPE 2 DIABETES MELLITUS WITH DIABETIC PERIPHERALANGIOPATHY WITH GANGRENETYPE 2 DIABETES MELLITUS WITH OTHER CIRCULATORYCOMPLICATIONSTYPE 2 DIABETES MELLITUS WITH DIABETIC NEUROPATHICARTHROPATHYTYPE 2 DIABETES MELLITUS WITH OTHER DIABETICARTHROPATHYTYPE 2 DIABETES MELLITUS WITH DIABETIC DERMATITISTYPE 2 DIABETES MELLITUS WITH FOOT ULCERTYPE 2 DIABETES MELLITUS WITH OTHER SKIN ULCERTYPE 2 DIABETES MELLITUS WITH OTHER SKIN COMPLICATIONSTYPE 2 DIABETES MELLITUS WITH PERIODONTAL DISEASETYPE 2 DIABETES MELLITUS WITH OTHER ORAL COMPLICATIONSTYPE 2 DIABETES MELLITUS WITH HYPOGLYCEMIA WITH COMATYPE 2 DIABETES MELLITUS WITH HYPOGLYCEMIA WITHOUTCOMATYPE 2 DIABETES MELLITUS WITH HYPERGLYCEMIATYPE 2 DIABETES MELLITUS WITH OTHER SPECIFIEDCOMPLICATIONTYPE 2 DIABETES MELLITUS WITH UNSPECIFIEDCOMPLICATIONSTYPE 2 DIABETES MELLITUS WITHOUT COMPLICATIONSStep 3 (history of oral antidiabetic agent)Required quantity: 14 days supplyLook back timeframe: 365 daysLabel NameGCNACTOPLUS MET 15 MG-500 MG TAB25444ACTOPLUS MET 15 MG-850 MG TAB25445ACTOPLUS MET XR 15-1000 MG TB28620ACTOPLUS MET XR 30-1000 MG TB28622ACTOS 15 MG TABLET92991ACTOS 30 MG TABLET93001ACTOS 45 MG TABLET93011SuperiorHealthPlan.comSHP 20194847Page 6 of 16
Step 3 (history of oral antidiabetic agent)Required quantity: 14 days supplyLook back timeframe: 365 daysLabel NameGCNALOGLIPTIN 12.5 MG TABLET34085ALOGLIPTIN 25 MG TABLET34076ALOGLIPTIN 6.25 MG TABLET34086ALOGLIPTIN-METFORMIN 12.5-100034088ALOGLIPTIN-METFORMIN 12.5-50034087ALOGLIPTIN-PIOGLIT 12.5-15 MG34080ALOGLIPTIN-PIOGLIT 12.5-30 MG34083ALOGLIPTIN-PIOGLIT 12.5-45 MG34084ALOGLIPTIN-PIOGLIT 25-15 MG34077ALOGLIPTIN-PIOGLIT 25-30 MG34078ALOGLIPTIN-PIOGLIT 25-45 MG34079AMARYL 1 MG TABLET05830AMARYL 2 MG TABLET05832AMARYL 4 MG TABLET05833AVANDIA 2 MG TABLET93193AVANDIA 4 MG TABLET93203AVANDIA 8 MG TABLET93363CHLORPROPAMIDE 100 MG TABLET05731CHLORPROPAMIDE 250 MG TABLET05732FARXIGA 10 MG TABLET34394FARXIGA 5 MG TABLET35698FORTAMET ER 1,000 MG TABLET21831FORTAMET ER 500 MG TABLET21832GLIMEPIRIDE 1 MG TABLET05830GLIMEPIRIDE 2 MG TABLET05832GLIMEPIRIDE 4 MG TABLET05833GLIPIZIDE 10 MG TABLET10841GLIPIZIDE 5 MG TABLET10840GLIPIZIDE ER 10 MG TABLET10843GLIPIZIDE ER 2.5 MG TABLET50638GLIPIZIDE ER 5 MG TABLET10844GLIPIZIDE XL 10 MG TABLET10843GLIPIZIDE XL 2.5 MG TABLET50638GLIPIZIDE XL 5 MG TABLET10844GLIPIZIDE-METFORMIN 2.5-250 MG18366GLIPIZIDE-METFORMIN 2.5-500 MG18367SuperiorHealthPlan.comSHP 20194847Page 7 of 16
Step 3 (history of oral antidiabetic agent)Required quantity: 14 days supplyLook back timeframe: 365 daysLabel NameGCNGLIPIZIDE-METFORMIN 5-500 MG18368GLUCOPHAGE 1000 MG TABLET10857GLUCOPHAGE 500 MG TABLET10810GLUCOPHAGE 850 MG TABLET10811GLUCOPHAGE XR 500 MG TAB89863GLUCOPHAGE XR 750 MG TAB19578GLUCOTROL 10 MG TABLET10841GLUCOTROL 5 MG TABLET10840GLUCOTROL XL 10 MG TABLET10843GLUCOTROL XL 2.5 MG TABLET50638GLUCOVANCE 2.5-500 MG TABLET92889GLUCOVANCE 5-500 MG TABLET89879GLUMETZA ER 1,000 MG TABLET97067GLUMETZA ER 500 MG TABLET97061GLYBURIDE 1.25 MG TABLET05710GLYBURIDE 2.5 MG TABLET05711GLYBURIDE 5 MG TABLET05712GLYBURIDE MICRO 1.5 MG TAB05713GLYBURIDE MICRO 3 MG TABLET05714GLYBURIDE MICRO 6 MG TABLET05715GLYBURIDE-METFORMIN 1.25-250 MG89878GLYBURIDE-METFORMIN 2.5-500 MG92889GLYBURIDE-METFORMIN 5-500 MG89879GLYNASE 1.5 MG PRESTAB05713GLYNASE 3 MG PRESTAB05714GLYNASE 6 MG PRESTAB05715GLYSET 100 MG TABLET95254GLYSET 25 MG TABLET95252GLYSET 50 MG TABLET95253GLYXAMBI 10-5 MG TABLET37832GLYXAMBI 25-5 MG TABLET37833INVOKAMET 150-1000 MG TABLET36859INVOKAMET 150-500 MG TABLET36953INVOKAMET 50-1000 MG TABLET36857INVOKAMET 50-500 MG TABLET36954INVOKAMET XR 150-1000 MG TABLET42315SuperiorHealthPlan.comSHP 20194847Page 8 of 16
Step 3 (history of oral antidiabetic agent)Required quantity: 14 days supplyLook back timeframe: 365 daysLabel NameGCNINVOKAMET XR 150-500 MG TABLET42314INVOKAMET XR 50-1000 MG TAB42313INVOKAMET XR 50-500 MG TABLET42312INVOKANA 100 MG TABLET34439INVOKANA 300 MG TABLET34441JANUMET 50-1,000 MG TABLET98307JANUMET 50-500 MG TABLET98306JANUMET XR 100-1000 MG TABLET31348JANUMET XR 50-1000 MG TABLET31340JANUMET XR 50-500 MG TABLET31339JANUVIA 100 MG TABLET97400JANUVIA 25 MG TABLET97398JANUVIA 50 MG TABLET97399JARDIANCE 10 MG TABLET36716JARDIANCE 25 MG TABLET36723JENTADUETO 2.5-1000 MG TAB31317JENTADUETO 2.5-500 MG TAB31315JENTADUETO 2.5-850 MG TAB31316JENTADUETO XR 2.5-1000 MG TAB41637JENTADUETO XR 5-1000 MG TAB41639KAZANO 12.5-1000 MG TABLET34088KAZANO 12.5-500 MG TABLET34087KOMBIGLYZE XR 2.5-1,000 MG TAB29225KOMBIGLYZE XR 5-1,000 MG TAB29224KOMBIGLYZE XR 5-500 MG TABLET29118METFORMIN HCL 1000 MG TABLET10857METFORMIN HCL 500 MG TABLET10810METFORMIN HCL 850 MG TABLET10811METFORMIN HCL ER 500 MG TABLET89863METFORMIN HCL ER 750 MG TABLET19578NATEGLINIDE 120 MG TABLET34027NATEGLINIDE 60 MG TABLET12277NESINA 12.5 MG TABLET34085NESINA 25 MG TABLET34086NESINA 6.25 MG TABLET34086ONGLYZA 2.5 MG TABLET27393SuperiorHealthPlan.comSHP 20194847Page 9 of 16
Step 3 (history of oral antidiabetic agent)Required quantity: 14 days supplyLook back timeframe: 365 daysLabel NameGCNONGLYZA 5 MG TABLET27394OSENI 12.5-15 MG TABLET34080OSENI 12.5-30 MG TABLET34083OSENI 12.5-45 MG TABLET34084OSENI 25-15 MG TABLET34077OSENI 25-30 MG TABLET34078OSENI 25-45 MG TABLET34079PIOGLITAZONE HCL 15 MG TABLET92291PIOGLITAZONE HCL 30 MG TABLET93001PIOGLITAZONE HCL 45 MG TABLET93011PIOGLITAZONE-GLIMEPIRIDE 30-2 MG97181PIOGLITAZONE-GLIMEPIRIDE 30-4 MG97180PIOGLITAZONE-METFORMIN 15-500 MG25444PIOGLITAZONE-METFORMIN 15-850 MG25445PRANDIMET 1 MG-500 MG TABLET16084PRANDIMET 2 MG-500 MG TABLET16085PRANDIN 0.5 MG TABLET26311PRANDIN 1 MG TABLET26312PRANDIN 2 MG TABLET26313PRECOSE 100 MG TABLET02318PRECOSE 25 MG TABLET08070PRECOSE 50 MG TABLET02319QTERN 10-5 MG TABLET43126REPAGLINIDE 0.5MG TABLET26311REPAGLINIDE 1 MG TABLET26312REPAGLINIDE 2 MG TABLET26313REPAGLINIDE-METFORMIN 1-500 MG TAB16084REPAGLINIDE-METFORMIN 2-500 MG TAB16085RIOMET 500 MG/5 ML SOLUTION20808STARLIX 120 MG TABLET34027STARLIX 60 MG TABLET12277STEGLUJAN 15-100 MG TABLET44238STEGLUJAN 5-100 MG TABLET44237SYNJARDY 12.5-1000 MG TABLET38932SYNJARDY 12.5-500 MG TABLET39378SYNJARDY 5-1000 MG TABLET38929SuperiorHealthPlan.comSHP 20194847Page 10 of 16
Step 3 (history of oral antidiabetic agent)Required quantity: 14 days supplyLook back timeframe: 365 daysLabel NameGCNSYNJARDY XR 10-1000 MG TABLET42788SYNJARDY XR 12.5-1000 MG TAB42787SYNJARDY XR 25-1000 MG TABLET42789SYNJARDY XR 5-1000 MG TABLET42786TOLAZAMIDE 250 MG TABLET05741TOLAZAMIDE 500 MG TABLET05742TOLBUTAMIDE 500 MG TABLET05724TRADJENTA 5 MG TABLET29890XIGDUO XR 10-1000 MG TABLET37344XIGDUO XR 10-500 MG TABLET37342XIGDUO XR 5-1000 MG TABLET37343XIGDUO XR 5-500 MG TABLET37339Step 4 (history of requested medication)Required quantity: 14 days supplyLook back timeframe: 365 daysLabel NameGCNADLYXIN 10-20 MCG STARTER PACK35688ADLYXIN 20 MCG MAINTENANCE PK35687BYDUREON 2 MG VIAL31304BYDUREON 2 MG PEN INJECT36352BYDUREON BCISE 2 MG AUTOINJECT44039BYETTA 5 MCG DOSE PEN INJ24613BYETTA 10 MCG DOSE PEN INJ24614OZEMPIC 0.25-0.5 MG DOSE PEN44163OZEMPIC 1 MG DOSE PEN44164SOLIQUA 100 UNIT-33 MCG/ML PEN42676TRULICITY 0.75 MG/0.5 ML PEN37169TRULICITY 1.5 MG/0.5 ML PEN37171VICTOZA 18 MG/3 ML PEN26189XULTOPHY 100 UNIT-3.6 MG/ML PEN38348SuperiorHealthPlan.comSHP 20194847Page 11 of 16
ICD-10 Z4931Z4932Step 5 (diagnosis of ESRD, CKD, pancreatitis, or gastroparesis)Required diagnosis: 1Look back timeframe: 730 daysDescriptionENCOUNTER FOR DIALYSIS AND DIALYSISCATHETER CARERENAL DIALYSIS ENCOUNTERFT/ADJ XTRCORP DIAL CATHFIT/ADJ PERIT DIAL CATHENCOUNTER FOR ADEQUACY TESTING FORDIALYSISHEMODIALYSIS TESTINGPERITONEAL DIALYSIS TESTDIALYSIS ENCOUNTER, NECGASTROPARESISCYTOMEGALOVIRAL PANCREATITISIDIOPATHIC ACUTE PANCREATITISBILIARY ACUTE PANCREATITISALCOHOL INDUCED ACUTE PANCREATITISDRUG INDUCED ACUTE PANCREATITISACUTE PANCREATITIS, UNSPECIFIEDOTHER ACUTE PANCREATITISALCOHOL-INDUCED CHRONIC PANCREATITISOTHER CHRONIC PANCREATITISCHRONIC KIDNEY DISEASE, STAGE 4 (SEVERE)CHRONIC KIDNEY DISEASE, STAGE 5END STAGE RENAL DISEASEENCOUNTER FOR FITTING AND ADJUSTMENTOF EXTRACORPOREAL DIALYSIS CATHETERENCOUNTER FOR FITTING AND ADJUSTMENTOF PERITONEAL DIALYSIS CATHETERENCOUNTER FOR ADEQUACY TESTING FORHEMODIALYSISENCOUNTER FOR ADEQUACY TESTING FORPERITONEAL DIALYSISStep 7 (procedure for ESRD services)Required diagnosis: 1Look back timeframe: 730 days (this step is removed)CPT Code90918909199092090921SuperiorHealthPlan.comSHP 20194847Page 12 of 16DescriptionESRD RELATED SERVICES, MONTHESRD RELATED SERVICES, MONTHESRD RELATED SERVICES, MONTHESRD RELATED SERVICES, MONTH
CPT 0967909689096990970Step 7 (procedure for ESRD services)Required diagnosis: 1Look back timeframe: 730 days- This step is removedDescriptionESRD RELATED SERVICES, DAYESRD RELATED SERVICES, DAYESRD RELATED SERVICES, DAYESRD RELATED SERVICES, DAYHEMODIALYSIS, ONE EVALUATIONHEMODIALYSIS, REPEATED EVALHEMODIALYSIS ACCESS STUDYHEMODIALYSIS, INITIAL OR ACUTE (EG, ACUTERENAL FAILURE OR INTOXICAT; PAT OVER 40KGHEMODIALYSIS, INITIAL OR ACUTE (EG, ACUTERENAL FAILURE OR INTOXICAT: PAT 21-40 KGHEMODIAL, INITIAL OR ACUTE (EG, ACUTERENAL FAILURE OR INTOXICAT; PAT OVER 40KGHEMODIAL, INITIAL OR ACUTE (EG, ACUTERENAL FAILURE OR INTOXICAT; PAT UNDER 10KGDIALYSIS, ONE EVALUATIONDIALYSIS, REPEATED EVALESRD SERV, 4 VISITS P MO, 2ESRD SERV, 2-3 VSTS P MO, 2ESRD SERV, 1 VISIT P MO, 2ESRD SERV, 4 VSTS P MO, 2-11ESRD SRV 2-3 VSTS P MO, 2-11ESRD SRV, 1 VISIT P MO, 2-11ESRD SRV, 4 VSTS P MO, 12-19ESRD SRV 2-3 VSTS P MO 12-19ESRD SERV, 1 VST P MO, 12-19ESRD SRV, 4 VISITS P MO, 20 ESRD SRV, 2-3 VSTS P MO, 20 ESRD SERV, 1 VISIT P MO, 20 ESRD HOME PT, SERV P MO, 2ESRD HOME PT SERV P MO, 2-11ESRD HOME PT SERV P MO 12-19ESRD HOME PT, SERV P MO, 20 ESRD HOME PT SERV P DAY, 2ESRD HOME PT SRV P DAY, 2-11ESRD HOME PT SRV P DAY 12-19ESRD HOME PT SERV P DAY, 20 SuperiorHealthPlan.comSHP 20194847Page 13 of 16
CPT 099090991909929099390994CPT Code8303683037Step 7 (procedure for ESRD services)Required diagnosis: 1Look back timeframe: 730 days- This step is removedDescriptionPERITONEAL DIALYSIS FOR CHRONICRENAL FAILURE; PATIENT MORE THAN 40KGPERITONEAL DIALYSIS FOR CHRONICRENAL FAILURE; PATIENT 21-40 KGPERITONEAL DIALYSIS FOR CHRONICRENAL FAILURE; PATIENT 11-20 KGPERITONEAL DIALYSIS FOR CHRONICRENAL FAILURE; PATIENT UNDER 10 KGPERITONEAL DIALYSIS FOR (ESRD), MAINTSTABI COND, HOSP/OTHER FACIL PER SET;MORE 40 KGPERITONEAL DIALYSIS FOR (ESRD),MAINTSTABL COND,HOSP/OTHER FAC PERSET;PATIENT 21-40 KGPERITONEAL DIALYSIS FOR (ESRD),MAINTSTABI COND, HOSP/OTHER FAC PERSET;PATIENT 11-20 KGPERITONEAL DIALYSIS FOR (ESRD),MAINTSTABI COND,HOSP/OTHER FAC PERSET;PATIENT UNDER 10KDIALYSIS TRAINING, COMPLETEHEMODIALYSIS TRAINING AND/ORCOUNSELINGHOME HEMODIALYSIS CARE, OUTPAT,SERV PROVID BY PHYSI RESPONS FORTOTAL CAREPERITONEAL DIALYSIS TRAINING AND/ORCOUNSELING (MEDICARE ONLY)DIALYSIS TRAINING, INCOMPLSUPERVISION OF CHRONICAMBPERITONEAL DIAL (CAPD),HOME/OUTPATIENT,MONTHLYStep 8 (procedure for HbA1c test)Required procedure: 1Look back timeframe: 180 days- This step is removed.DescriptionGLYCOSYLATED HEMOGLOBIN TESTGLYCOSYLATED HB, HOME DEVICESuperiorHealthPlan.comSHP 20194847Page 14 of 16
Clinical Criteria References:1. 2015 ICD-9-CM Diagnosis Codes. 2015. Available at www.icd9data.com. Accessed on April 3,2015.2. 2015 ICD-10-CM Diagnosis Codes. 2015. Available at www.icd10data.com. Accessed on April3, 2015.3. American Medical Association data files. 2015 ICD-9-CM Diagnosis Codes. Available atwww.commerce.ama-assn.org.4. American Medical Association data files. 2015 ICD-10-CM Diagnosis Codes. Available atwww.commerce.ama-assn.org.5. Clinical Pharmacology [online database]. Tampa, FL: Elsevier/Gold Standard, Inc.; 2018.Available at www.clinicalpharmacology.com. Accessed on July 5, 2019.6. Micromedex [online database]. Available at www.micromedexsolutions.com. Accessed on July5, 2019.7. Adlyxin Prescribing Information. Bridgewater, NJ. sanofi-aventis U.S. LLC. January 2019.8. Byetta Prescribing Information. Wilmington, DE. AstraZeneca Pharmaceuticals LP. December2018.9. Bydureon Prescribing Information. Wilmington, DE. AstraZeneca Pharmaceuticals LP. February2019.10. Bydureon BCise Prescribing Information. Wilmington, DE. AstraZeneca Pharmaceuticals LP.March 2019.11. Ozempic Prescribing Information. Plainsboro, NJ. Novo Nordisk Inc. April 2019.12. Soliqua Prescribing Information. Bridgewater, NJ. sanofi-aventis U.S. LLC. February 2019.13. Tanzeum Prescribing Information. Research Triangle Park, NC. GlaxoSmithKline LLC. December2017.14. Trulicity Prescribing Information. Indianapolis, IL. Eli Lilly and Company. January 2019.15. Victoza Prescribing Information. Plainsboro, NJ. Novo Nordisk Inc. June 2019.16. Xultophy Prescribing Information. Plainsboro, NJ. Novo Nordisk Inc. February 2019.17. American Diabetes Association. Standards of Medical Care in Diabetes-2018. Diabetes Care2018;41(Suppl 1).18. Qaseem A, Humphrey LL, Sweet DE, et al, for the Clinical Guidelines Committee of the AmericanCollege of Physicians. Oral pharmacologic treatment of type 2 diabetes mellitus: a clinicalpractice guideline from the American College of Physicians. Ann Intern Med. 2012 Feb7;156(3):218-31.SuperiorHealthPlan.comSHP 20194847Page 15 of 16
19. Rosenzweig JL, Ferrannini E, Grundy SM, et al. Primary Prevention of Cardiovascular Diseaseand Type 2 Diabetes in Patients at Metabolic Risk: An Endocrine Society Clinical PracticeGuideline. J Clin Endocrinol Metab. October 2008, 93(10):3671-3689.Publication History:Publication1/7/20198/16/2019NotesCriteria created and cross referenced to VDP criteria. VDP criteria is dated 46-18. Removed steps 6 and 7 of original VDP criteria per Superior P&TCommittee approval. Removed GCNs for Tanzeum (no longer available), pages 2 and 11Expanded age for Victoza to 10 years (question #2) in criteria logic andlogic diagram, pages 3-4Updated references, pages 15-16Updated to include formulary statement (The listed GCNS may not be anindication of TX Medicaid Formulary coverage. To learn the currentformulary coverage, visit TxVendorDrug.com/formulary/formularysearch.) on each ‘Drug Requiring PA’ tableSuperiorHealthPlan.comSHP 20194847Page 16 of 16
bydureon 2 mg vial 31304 bydureon 2 mg pen inject 36352 bydureon bcise 2 mg autoinject 44039 byetta 5 mcg dose pen inj 24613 byetta 10 mcg dose pen inj 24614 ozempic 0.25-0.5 mg dose pen 44163 ozempic 1 mg dose pen 44164 soliqua 100 unit-33 mcg/ml pen 42676 trulicity 0.75 mg/0.5 ml pen 37169