Transcription
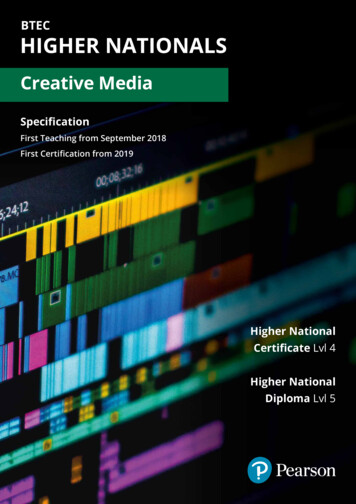
Information & Assistance Unit guide 4How to file an application for adjudication of claimComplete this form if you have a disagreement with your employer or its insurancecompany about your case and you want it resolved by your local Workers’Compensation Appeals Board (WCAB). Filing this form opens a case with theWCAB.You can also complete this form if you think you may need the WCAB to resolve adispute in the future and the time allowed for you to file the application could runout. If you have questions about whether time limits apply in your case, contactyour local Information and Assistance office. You can get information on contactinga local I&A office on the Web at www.dwc.ca.gov.Complete the form and follow the instructions attached. This form can also becompleted at WC1.pdf.Please note that a hearing in your case will not be scheduled until a declaration ofreadiness to proceed is filed (see I&A guide 5).The following papers must be included with your completed application:1. A copy of your claim for workers’ compensation benefits (required only forinjuries that happened between 1-1-90 and 12-31-93). See I&A guide 1.2. Declaration required by law (Labor Code section 4906(h) -- see attached). Aproof of service is recommended. See attached.Send the original to your local WCAB office and copies to all the parties.Submit the following documents with your form filing in the order shown:Document Cover SheetDocument Separator Sheet (for Application for Adjudication of Claim)Application for Adjudication of ClaimDocument Separator Sheet (for Proof Of Service By Mail)Proof Of Service By MailDocument Separator Sheet (for Declaration Pursuant to Labor CodeSection 4906(h)) Declaration Pursuant to Labor Code Section 4906(h) Keep copies of your filings for your records.I&A 4Rev. 06/18
Information & Assistance Unit guide 4All documents filed with the WCAB must include a document cover sheet anddocument separator sheet. Please see I&A guides 17 and 18 to learn how tocomplete these forms. In addition all forms must be typed or handwritten inblock letters to insure legibility. Additional form instructions can be found on theEAMS OCR handbook athttp://www.dir.ca.gov/dwc/eams/SampleFiles/EAMS OCR%20handbook.pdf.If you need help, call an Information and Assistance (I&A) office, or attend aworkshop for injured workers. The local I&A phone numbers are attached to thisguide. You can get information on a local workshop from the I&A office or on theWeb at www.dwc.ca.gov.If you do not have the name and address of your claims administrator tocomplete a form, please link to mins.asp.The information contained in this guide is general in nature and is not intended as a substitute forlegal advice. Changes in the law or the specific facts of your case may result in legalinterpretations different than those present here.When sending documents to a district office, please make sure they are not folded or stapled.Send them in a large manila envelope. Please see the EAMS OCR forms handbook for furtherinstructions.I&A 4Rev. 06/18
WORKERS’ COMPENSATION APPEALS BOARD DISTRICT OFFICESANAHEIM, 92806-21311065 North Link, Suite 170Information & Assistance Unit (714) 414-1801SACRAMENTO, 95834-2962160 Promenade Circle, Suite 300Information & Assistance Unit (916) 928-3158BAKERSFIELD, 93301-1929th1800 30 Street, Suite 100Information & Assistance Unit (661) 395-2514SALINAS, 93906-22041880 N Main Street, Suites 100 & 200Information & Assistance (831) 443-3058EUREKA, 95501-0529 * Virtual office *Information & Assistance Unit(707) 441-5723SAN BERNARDINO, 92401-1411464 W Fourth Street, Suite 239Information & Assistance Unit (909) 383-4522FRESNO, 93721-22192550 Mariposa Street, Suite 4078Information & Assistance Unit (559) 445-5355SAN DIEGO, 92108-44247575 Metropolitan Drive, Suite 202Information & Assistance Unit (619) 767-2082LONG BEACH, 90810-18701500 Hughes Way, Suite C203Information & Assistance Unit (424) 450-2565SAN FRANCISCO, 94102-7014nd455 Golden Gate Avenue, 2 FloorInformation & Assistance Unit (415) 703-5020LOS ANGELES, 90013-1105thth320 W 4 Street, 9 FloorInformation & Assistance Unit (213) 576-7389SAN JOSE, 95113-1402100 Paseo de San Antonio, Suite 241Information & Assistance Unit (408) 277-1292MARINA DEL REY, 90292-6902ndrd4720 Lincoln Boulevard, 2 and 3 FloorsInformation & Assistance Unit (310) 482-3820SAN LUIS OBISPO, 93401-87364740 Allene Way, Suite 100Information & Assistance Unit (805) 596-4159OAKLAND, 94612-1499th1515 Clay Street, 6 FloorInformation & Assistance Unit (510) 622-2861SANTA ANA, 92707-77042 MacArthur Place, Suite 600Information & Assistance Unit (714) 942-7576OXNARD, 93030-79121901 N Rice Avenue, Suite 100Information & Assistance Unit (805) 485-3528SANTA BARBARA, 93101-7538 * Satellite office *130 E Ortega StreetInformation & Assistance Unit (805) 568-1390POMONA, 91768-1653732 Corporate Center DriveInformation & Assistance Unit (909) 623-8568SANTA ROSA, 95404-477150 “D” Street, Suite 420Information & Assistance Unit (707) 576-2452REDDING, 96002-0940nd250 Hemsted Drive, 2 Floor, Suite BInformation & Assistance Unit (530) 225-2047STOCKTON, 95202-231431 E Channel Street, Suite 344Information & Assistance Unit (209) 948-7980RIVERSIDE, 92501-33373737 Main Street, Suite 300Information & Assistance Unit (951) 782-4347VAN NUYS, 91401-33706150 Van Nuys Boulevard, Suite 105Information & Assistance Unit (818) 901-5374Rev. 07/21
STATE OF CALIFORNIADWC DISTRICT OFFICESAMPLEDOCUMENT COVER SHEETIs this a new case?YesDMore than 15 Companion CasesNoDCompanion Cases ExistDWalkthroughDTODAY'S DATEDate:(MM/DD/YYYY)EAMS CASE NUMBERCase Number 1SSN:DSpecific InjuryDCumulative InjuryDNoDYOUR SOCIALSECURITY NUMBERDATE OF INJURY(End Date: MM/DD/YYYY)(Start Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)IF NEW CASELEAVE BLANKBody Part 1:USE CODE FROMBODY PART CODE LIST -Body Part 3:SEE PAGE 8Body Part 2:Body Part 4:Other Body Parts:Yes WHEN MORE THAN 5 BODY PARTS USE BODYPART NUMBER 700 IN THIS FIELDPlease check unit to be filed on ( check only one box )DADJCompanion CasesCase Number 2IDDEUDSIFDUEFDSpecific InjuryDCumulative InjuryDDINTSAU(Start Date: MM/DD/YYYY)Body Part 3:Body Part 2:Body Part 4:DWC-CA form 10232.1 Rev. 5/2020- Page 1 of 8(End Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)Body Part 1:Other Body Parts:0RSU
District office codes for place of venueLegend ta AnaBakersfieldEureka*FresnoLos AngelesLong BeachMarina del linasSanta Barbara**San BernardinoSan DiegoSan FranciscoSan JoseSan Luis ObispoSanta RosaStocktonVan Nuys* Eureka is a satellite office of Santa Rosa district office.** Santa Barbara is a satellite office of Oxnard district office.Use this document to complete forms,but do not file this document with your forms.DWC‐CA form 10232.1 Rev. 5/2020 – Page 7 of 8
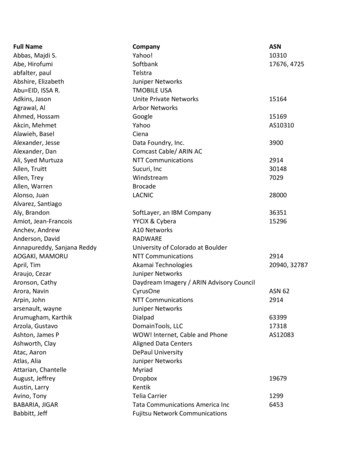
BODY PART CODES 0410411420430440450498DescriptionHead - not specifiedBrainEar - not specifiedEar - externalEar - internal including hearingEye - including optic nerves and visionFace - not specifiedJaw - including chin and mandibleMouth - including lips, tongue, throat and tasteTeethNose - including nasal passages, sinus and smellFace - multiple parts any combination of above partsFace - forehead, cheeks, eyelidsScalpSkullHead - multiple injury any combination of above partsNeckUpper extremities - not specifiedArm - above wrist not specifiedArm - upper arm humerusArm - elbow head of radiusArm - forearm radius and ulnaArm - multiple parts any combination of above partsArm - not specifiedWristHand - not wrist or fingersFingersUpper extremities - multiple parts any combination ofabove partsTrunk - not specifiedAbdomen - including internal organs and groinHerniaBack - including back muscles, spine and spinal cordChest - including ribs, breast bone and internal organs ofthe chestHips - including pelvis, pelvic organs, tailbone, coccyx andbuttocksShoulders - scapula and clavicleTrunk - use for side; multiple parts any combination ofabove parts
onLower extremities - not specifiedLegs - above ankles, not specifiedThigh femurKnee PatellaLower leg tibia and fibulaLeg - multiple parts any combination of above partsLeg - not specifiedAnkle malleolusFoot not ankle or toeToesLower extremities - multiple parts any combination of abovepartsMultiple parts more than five major parts use only in fifthposition of listing of body partsBody system - not specificCirculatory system - heart - other than heart attack, blood,arteries, veins, etc.Circulatory system - Heart attackDigestive system - stomachExcretory system - kidneys, bladder, intestines, etc.Musculo-skeletal system - bones, joints, tendons, muscles,etc.Nervous system - not specifiedNervous system - StressNervous system - Psychiatric/psychRespiratory system - lungs, trachea, etc.Skin dermatitis, etc.Reproductive systemsOther body systemsCOVID-19Unclassified - insufficient information to identify body parts
SAMPLEDOCUMENT SEPARATOR SHEETProduct Delivery UnitDocument TypeDocument TitleADJLEGAL DOCSAPPLICATION FOR ADJUDICATIONDocument DateAuthorDATE YOU FILLED OUT THE FORMMM/DD/YYYYYOUR NAMEOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2017 Page 1MM/DD/YYYY
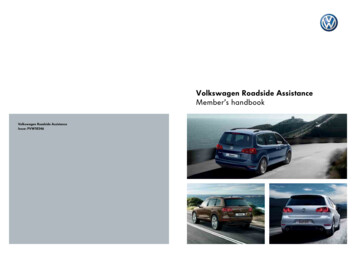
STATE OF CALIFORNIADIVISION OF WORKERS' COMPENSATIONWORKERS' COMPENSATION APPEALS BOARDAPPLICATION FOR ADJUDICATION OF CLAIMSAMPLEjD Amended ApplicationLEAVE BLANKCase No.YOUR SOCIAL SECURITY NUMBERSSN (Numbers Only)Venue choice is based upon (Completion of this section is required)D County of residence of employee (Labor Code section 5501.5(a)(1) or (d).)SELECT ONED County where injury occurred (Labor Code section 5501.5(a)(2) or (d).)D County of principal place of business of employee's attorney (Labor Code section 5501.5(a)(3) or (d).)USE 3 LETTER OFFICE CODE FROMDOCUMENT COVER SHEETSelect 3 - Letter Office Code For PlaceNenue of Hearing (From the Document Cover Sheet)Injured Worker (Completion of this section is required)YOUR FIRST NAMEFirst NameMlYOUR LAST NAMELast NameYOUR MAILING ADDRESSStreet Address/PO Box (Please leave blank spaces between numbers, names or words)Street Address2/PO Box (Please leave blank spaces between numbers, names or words)International Address (Please leave blank spaces between numbers, names or words)YOUR CITYStateCityApplicant (If other than Injured Worker)D Insurance CarrierD EmployerDZip CodeLien ClaimantName (Please leave blank spaces between numbers, names or words)Street Address/PO Box (Please leave blank spaces between numbers, names or words)Street Address2/PO Box (Please leave blank spaces between numbers, names or words)CityDWC/WCAB Form 1A (5/2020)- (PageState1)Zip CodeWCAB1j
ISAMPLEEmployer Information (Completion of this section is required)D InsuredD Self-InsuredDjD UninsuredLegally UninsuredNAME OF COMPANY YOU WERE WORKING FOR AT TIME OF INJURYEmployer Name (Please leave blank spaces between numbers, names or words)COMPANY ADDRESSEmployer Street Address/PO Box (Please leave blank spaces between numbers, names or words)COMPANY CITYCityZip CodeStateInsurance Carrier Information (If known and if applicable - include even if carrier is adjusted by claims administrator)NAME OF COMPANY INSURANCE CARRIERInsurance Carrier Name (Please leave blank spaces between numbers, names or words)INSURANCE CARRIER ADDRESSInsurance Carrier Street Address/PO Box (Please leave blank spaces between numbers, names or words)INSURANCE CARRIER CITYCityStateZip CodeClaims Administrator Information (If known and if applicable)NAME OF CLAIMS ADMINISTRATORName (Please leave blank spaces between numbers, names or words)CLAIMS ADMINISTRATOR ADDRESSStreet Address/POBox (Please leave blank spaces between numbers, names or words)CLAIMS ADMINISTRATOR CITYCityZip CodeStateIT IS CLAIMED THAT (Complete all relevant information):1. The injured worker, bornYOUR BIRTH DATE(DATE OF BIRTH: MM/DD/YYYY)(Choose only one)suffered a:Dspecific injuryDcumulative injuryThe injury occurred atYOUR JOB TITLE WHEN INJURED, while employed as a(n) ---- - - -:- -:- - -:-:---:- :- - - :-:: - :- -: - -:-::--(OCCUPATION AT THE TIME OF INJURY)DATE OF ACCIDENT(Date of injury: MM/DD/YYYY)which began on(Start Date: MM/DD/YYYY)and ended on(End Date: MM/DD/YYYY)ADDRESS WHERE ACCIDENT TOOK PLACEStreet Address/PO Box- Please leave blank spaces between numbers, names or wordsCityDWC/WCAB Form 1A (5/2020)- (Page 2)StateZip CodeWCAB1l
IBody Part 1:Body Part 2:SAMPLE(State which parts of the body were injured)PART OF BODY THAT WAS INJURED, USE LISTFROM DOCUMENT COVER SHEETBody Part 3:Body Part 4:Other BodyParts:2. The injury occurred as follows:(EXPLAIN WHAT THE WORKER WAS DOING AT THE TIME OF INJURY AND HOW THE INJURY OCCURED)INDICATE WHAT YOU WERE DOING AT THE TIME OF INJURY3. Actual earnings at the time of injury:Rate of Pay DMonthlyDWeeklyDDDDState value of tips, meals, lodging, or otheradvantages, regularly received HourlyNumber of hours worked per weekMonthlyWeeklyHourly----4. The injury caused disability as follows:Last day off work due to injury:LAST DAY WORKEDMM/ DD/YYYYFirst Period of Disability:Start DateSecond Period of Disability:Start DateFIRST DAY OFF WORKMM/DD/YYYYEnd DateDATE RETURNEDTO WORKMM/DD/YYYYEnd DateMM/DD/YYYYMM/DD/YYYY5. Compensation:Compensation was paid:DYesDNoTotal paid:Weekly rate(s):FROM CLAIMS ADMINISTRATORDate of last payment:-------MM/DD/YYYY6. Has the worker received any unemployment insurance benefits and/or any unemployment compensationYesNodisability benefits (state disability) since the date of injury?0DWC/WCAB Form 1A (5/2020)- (Page3)0WCAB1l
r;-;:-dical treatment:I ·M d al treatment was received:All treatment was furnished by the Employer or Insurance Carrier:Date of last treatment:-'i"'iM.,M""/ D"""D'""IY""'Y"'"Y""'Y Other treatment was provided/paid by:DYes0NoDYes0NoSAMPLEIF YOU OR PRIVATE INSURANCE PAIDFOR MEDICAL TREATMENT--- ----(NAME OF PERSON OR AGENCY PROVIDING OR PAYING FOR MEDICAL CARE)DYesDid Medi-Cal pay for any health care related to this claim?0NoNames and addresses of doctor(s)/hospital(s)/clinic(s) that treated or examined for this injury, but that were notprovided or paid for by the employer or insurance carrier:Name of Doctor/Hospital/Clinic 1 (Please leave blank spaces between numbers, names or words)Name of Doctor/Hospital/Clinic 2 (Please leave blank spaces between numbers, names or words)8. Other cases have been filed for industrial injuries by this worker as follows:LIST ANY OTHER CASES FILED WITH DWCCase Number 1Case Number 3Case Number 2Case Number 49. This application is filed because of a disagreement regarding liability for:DTemporary disability indemnityDPermanent disability indemnityDReimbursement for medical expenseDRehabilitationDMedical treatmentDSupplemental Job Displacement/Return to WorkDCompensation at proper rateDOther (Specify)DWC/WCAB Form 1A (5/2020)- (Page 4)WCAB1j
DYes D Nolis the Applicant Represented?If "No", applicant is to sign and date below.If "Yes", applicant's representative is to complete the following and is to sign and date below.D Law Firm/AttorneyDNon-Attorney RepresentativeSAMPLETLaw Firm or Company Name (If Applicable)Law Firm Number (If Applicable)Attorney/Representative First NameMlAttorney/Representative Last NameStreet Address/PO Box (Please leave blank spaces between numbers, names or words)CityStateZip CodeYOUR SIGNATUREApplicant SignatureApplicant Attorney/Representative SignatureDated atDate---------------- :-:--------------------'CityCaliforniaTODAY'S DATEMM/00/YYYYDWC/WCAB Form 1A (5/2020)- (Page5)WCAB1l
INSTRUCTIONS G AND SERVICE OF A DECLARATION OF READINESS IS A PREREQUISITE TO THE SETTING OF AI CASE FOR HEARING.Effect of Filing ApplicationFiling of this application begins formal proceedings against the defendant(s) named in your application.Assistance in Filling Out ApplicationYou may request the assistance of an information and assistance officer of the Division of Workers' Compensation.Right to AttorneyYou may be represented by an attorney or agent, or you may represent yourself. The attorney's fee will be set by theWorkers' Compensation Appeals Board at the time the case is decided and is ordinarily payable out of youraward.Filling Out ApplicationFor "amended" applications, the venue choice must be the same as that specified on the original application, unless anorder changing venue has issued. A street or P.O. Box address within the United States must be entered for the placewhere the injury occurred. Therefore, if the injury did not occur at a fixed or identifiable location (such as a field, ahighway,or on water), or if the injury occurred outside of the United States, the employer's business address or anotherappropriate address must be specified; however, a short explanation regarding the place of injury may be appended tothe application. If medical treatment has been paid for by Medi-Cal, Medicare, group health insurance, or a private carrier,please specify.Service of DocumentsYour attorney or agent will serve all documents in accordance with Labor Code section 5501 and the Workers'Compensation Appeals Board's Rules of Practice and Procedure.If you have no attorney or agent, copies of this application will be served by the Workers' Compensation AppealsBoard on all parties. If you file any other document, you must mail or deliver a copy of the document to all parties in thecase.IMPORTANT!If any applicant is under 18 years of age, it will be necessary to file a Petition for Appointment of Guardian ad Litem.Forms for this purpose may be obtained at the district office of the Workers' Compensation Appeals Board, or bycalling the district office and requesting this form.DWC/WCAB Form 1A (5/2020 ) - (Page 6)WCAB1l
SAMPLEDOCUMENT SEPARATOR SHEETProduct Delivery UnitADJDocument TypeLEGAL DOCSDocument TitlePROOF OF SERVICEDocument DateAuthorDATE YOU FILLED OUT THE FORMMM/DD/YYYYYOUR NAMEOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2017 Page 1MM/DD/YYYY
Proof of Service by MailSAMPLEI declare that:YOUR COUNTYI am (resident of / employed in) the county of ,California.I am over the age of eighteen years, my (business / residence) address is:PUT YOUR HOME ADDRESS HERENAME OF DOCUMENTTODAY'S DATE I served the attachedOn ,on the parties listed below in said case, by placing a true copy thereof enclosed ina sealed envelope with postage thereon fully paid, in the United State mail atCITY WHERE YOU MAILED THISaddressed as follows:1) WORKERS' COMPENSATION APPEALS BOARD: ADDRESS2) INSURANCE COMPANY: NAME, ADDRESS AND CLAIM NUMBER3) DEFENSE ATTORNEY (IF KNOWN): NAME AND ADDRESS4) ALL OTHER PARTIES INVOLVED IN YOUR CASE: NAME AND ADDRESSI declare under penalty of perjury under the laws of the State of California that theforegoing is true and correct, and that this declaration was executed onTODAY'S DATE at ,CITY(date) ,California.PRINT YOUR NAMEType or print nameSIGN YOUR NAMESignature
SAMPLEDOCUMENT SEPARATOR SHEETProduct Delivery UnitADJDocument TypeLEGAL DOCSDocument Title4906(h) DECLARATIONDocument DateAuthorDATE YOU FILLED OUT THE FORMMM/DD/YYYYYOUR NAMEOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2017 Page 1MM/DD/YYYY
SAMPLEDECLARATION PURSUANT TO LABOR CODE SECTION 4906(h)Pursuant to Labor Code Section 4906(h), I declare under penalty of perjury that I have notviolated Section 139.3 and I have not offered, delivered, received, or accepted any rebate, refund,commission, preference, patronage dividend, discount, or other consideration, whether in theform of money or otherwise, as compensation or inducement for any referred examination orevaluation.TODAY'S DATEDate:YOUR SIGNATURESignatureBefore signing this form, you should be aware that: “Any person who makes or causes to bemade any knowingly false or fraudulent material statement or representation for the purpose ofobtaining or denying workers’ compensation benefits or payments is guilty of a felony.”
WORKERS' COMPENSATION APPEALS BOARD DISTRICT OFFICES . ANAHEIM, 92806-2131 . 1065 North Link, Suite 170 . VAN NUYS, 91401-3370 . 6150 Van Nuys Boulevard, Suite 105 . Street Address/PO Box (Please leave blank spaces between numbers, names or words)