Transcription
Effect of an evidence-based answering service on GPsand their patients: a pilot studyBlackwell Publishing, Ltd.Anita A. H. Verhoeven* and Jan Schuling, *University Library and Department of General Practice,University of Groningen, Ant. Deusinglaan 1, 9713 AV Groningen, the NetherlandsAbstractObjectives: For general practitioners (GPs), an important obstacle to practisingevidence-based medicine is lack of time. An evidence-based answering servicewas developed that took over searching and appraisal of medical evidence fromthe GPs. GPs sent in questions, and the informationist formulated the answers.Our objectives were to find out if such an evidence-based answering service wasfeasible, including assessing the effect of the answers on GPs and their patients,as reported by the GPs.Methods: After attending a workshop on building well-formulated questionsfrom daily practice, the GPs sent in questions to the informationist. The literature was searched, the relevant information was appraised, and the answers tothe questions were formulated. With a questionnaire, the effect of the answerson the GP and the patient was assessed, as well as the perceived barriers toimplementing the answers.Results: From 26 GPs, 61 questions were received. For 12% of questions, information was found with the highest evidence level, while for 36%, no information was found. However, for 89% of the questions for which no informationcould be found, the answer ‘no information found’ did have an effect on the GPconcerned. In total, 81% of all the answers had an effect on the GP, and,according to the GP, 52% had an effect on the patient. Few barriers to implementing the evidence were perceived. Most of the answers were found inPubmed/Medline, the Cochrane Library and Embase.Conclusions: This study indicates that an evidence-based answering servicecan have an impact on GPs and their patients. Librarians can provide anevidence-based answering service for GPs and their patients. The evidence-basedanswering service for GPs in this study had an impact on 81% of the GPs and on52% of their patients. Although for one-third of the questions no evidence-basedanswer was found, this message in itself had an impact on 89% of the GPs. Aninformationist as mediator between medical information and doctors can savedoctors’ time.IntroductionCorrespondence: Anita A. H. Verhoeven, University Library andDepartment of General Practice, University of Groningen, Ant.Deusinglaan 1, 9713 AV Groningen, the Netherlands.E-mail: a.a.h.verhoeven@med.rug.nlMedical libraries offer training sessions to theirpatrons on how to search medical databaseseffectively, 1,2 which stimulates the practice ofevidence-based medicine (EBM). EBM includes Health Libraries Group 2004 Health Information and Libraries Journal, 21 (Suppl. 2), pp.2 7 – 3527
28Study of evidence-based answering service, Anita A. H. Verhoeven and Jan Schulingformulating a well-built clinical question encountered in daily practice, performing a literaturesearch in a medical literature database, criticallyappraising relevant articles, and implementing theevidence-based answer in medical practice.3However, McColl et al. found that general practitioners (GPs) prefer predigested, evidence-basedinformation to searching the evidence themselves.4This is also our experience after having offeredmany literature courses for 10 years to GPs. Previous qualitative research found many barriers toimplementing evidence-based medicine, and oneimportant factor constantly occurring was lack oftime.5 9 Therefore, an evidence-based answeringservice for GPs10 14 was introduced in which literature searching, appraising of relevant articles, andformulating the answer was taken over by aninformationist.15This study will describe the characteristics ofthe authors’ evidence-based answering service, theeffect of the answer on the GP and the patient, andthe perceived barriers to implementing the answer.MethodsGPs who were affiliated to the Department ofGeneral Practice at the University of Groningenin the Netherlands were invited to participate inthe study. These GPs worked in the north of theNetherlands, and for 1 or 2 days a week they wereinvolved in either teaching or research. We did notregister the GPs’ personal or practice characteristics.Before the GPs could send in patient-orientatedquestions to the informationist of the literatureservice, they attended a 1.5 h workshop led bythe informationist on how to formulate well-builtclinical questions in the patient–intervention–comparison–outcome (PICO) format.16 The workshops were offered at the Department of GeneralPractice, at conferences, or on site at the workplace.The medical informationist is a new health profession.15 The informationist in our project wastrained as a GP and worked as such for several years.She has worked in a medical library for 15 years asa medical information specialist, in addition toworking as a university teacher of evidence-basedmedicine at the Department of General Practice.She is also an experienced researcher in the field ofmedical information sciences.17 In the context ofthis study, an informationist should have thecombination of skills of a librarian (identifyingrelevant literature references) with those of a GP(being familiar with the setting and the mentalprocess GPs are going through when seeing patients,and being able to communicate through the medical language). Furthermore, an informationistneeds knowledge about both content and structure of the medical literature required for criticalappraisal.The informationist was able to provide theevidence-based answering service with the supportof a 1-year grant for 2 days a week. The Universityextended this period for another year. The informationist worked at the Department of GeneralPractice Library, which is part of the largely digitalized University Library. All literature databasesand electronic journals therefore were accessiblefrom the informationist’s desk, as well as servicesfor document delivery and interlibrary loan. Thisinfrastructure was essential for the work as aninformationist.The GPs sent in questions on special requestforms derived from those used in Hayward’s study.10They provided the following information: asummary of the case history; the PICO-formulatedquestion; urgency (answer needed in 1, 2, 3 ormore than 3 weeks); comments, e.g. informationsources already used; and personal information,i.e. their name, address, telephone, fax: and e-mailaddress. They sent in the forms by ordinary postor by fax, and could choose how to receive theanswer: by post, fax: or e-mail. No reminders weresent about the evidence-based answering service.To answer the question a GP had sent in, theinformationist selected appropriate informationsources (Table 1) based on availability and accessibility, quality of the content (meta-analyses,systematic reviews, randomised controlled trials,critically appraised articles), and focus on primarycare. The order of the information sources wasbased on the focus of the question and the contentand quality of the information source. A typicalsearch started in the highest quality evidencebased sources: the Cochrane Library and ClinicalEvidence. If necessary, the most important journalarticle databases such as Medline, sources referringto primary research giving comments (e.g. ACPJournal Club), and medical search engines (e.g. Health Libraries Group 2004 Health Information and Libraries Journal, 21 (Suppl. 2), pp.27 –35
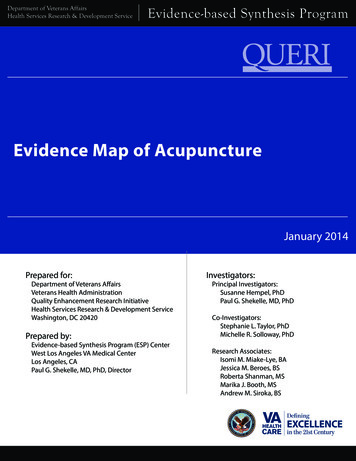
Study of evidence-based answering service, Anita A. H. Verhoeven and Jan SchulingTable 1 Databases used for answering61 clinical questionsDatabase nameFrequencyof use (% ofquestions)Frequencyof databaseused that ledto answer (%of questions)Medline/PubMedCochrane LibraryEmbaseSumSearchNat. Guidelines ClearinghouseTRIP databaseACP Journal ClubBandolierHSTATClinical EvidenceMedlinePlusOther databasesUnknownNo answer57 (93)49 (80)43 (71)34 (56)34 (56)33 (54)32 (53)26 (43)23 (38)20 (33)18 (30)16 (26)——24 (39)8 (13)5 (8)04 (7)1 (2)1 (2)001 (2)04 (7)2 (3)20 (33)PubMed (free) at http://pubmed.gov is the largest medical database with referencesfrom 4500 biomedical journals from all around the world. The Cochrane Library (notfree) at http://www.update-software.com collects evidence about the effects of healthcare. It consists of several databases of which the Cochrane Database of SystematicReviews, the Database of Abstracts of Reviews of Effects (DARE) and The CochraneCentral Register of Controlled Trials (CENTRAL) were used in our study. Embase fromElsevier Science (not free) is available at http://www.ovid.com is a comprehensivepharmacological and biomedical database renowned for extensive indexing of druginformation from 3600 journals. SUMSearch (free) at http://sumsearch.uthscsa.edusearches medical evidence in several databases on the Internet. National GuidelinesClearinghouse (free) at http://www.guideline.gov is a USA governmental resource forevidence-based clinical practice guidelines. The TRIP database (not free) at http://www.update-oftware.com/trip/about.htm searches evidence-based healthcareresources available on the Internet. ACP Journal Club (not free) at http://www.acpjc.org selects, summarizes and comments on articles from 100 internalmedicine journals. Bandolier (free) at http://www.jr2.ox.ac.uk/bandolier distilsinformation from (secondary) reviews of (primary) trials using evidence-basedmedicine techniques to provide advice about particular treatments or diseases. HSTAT(Health Services/Technology Assessment Text) (free) at me/s/51817 is a searchable collection of large, full-textclinical practice guidelines, technology assessments and health information. ClinicalEvidence (not free) at http://www.clinicalevidence.com summarizes the current stateof knowledge and uncertainty about the prevention and treatment of clinicalconditions based on searches and appraisal of the literature. MedlinePlus (free) athttp://www.nlm.nih.gov/medlineplus is a consumers’site with information fromgovernmental and other sources on over 600 diseases and conditions.TRIP database and SUMsearch) were searched.To conclude, quality guidelines were searched, inwhich original studies were tracked down. In general, information with the strongest evidence wasused; for therapy questions a meta-analysis fromthe Cochrane Library. However, if no strong evidence was found, weaker evidence was used, e.g.cohort studies, or guidelines based on consensusbetween experts.The search strategy consisted in many casesof only one concept, the disease or problem, e.g.arthrosis. This concept was translated into aMedical Subject Term, e.g. ‘osteoarthritis-knee’, usedby many of the information sources (Medline, Health Libraries Group 2004 Health Information and Libraries Journal, 21 (Suppl. 2), pp.2 7 – 3529
30Study of evidence-based answering service, Anita A. H. Verhoeven and Jan SchulingCochrane Library, SUMsearch), or the conceptwas translated into the controlled vocabulary of thedatabase used (e.g. Embase uses ‘knee arthritis’).If needed, free-text terms were added as well, e.g.‘knee arthrosis’. If the results were too broad, asecond or third term was added, combined withthe Boolean operator ‘AND’. If too many relevantarticles were found, the search was restricted withmethodology terms, such as ‘meta-analysis’, ‘randomised controlled trial’, or ‘cohort studies’. InPubMed, the ‘clinical questions’ feature was usedfor this purpose. If no full text article could beobtained, the appraisal and answer were basedon the abstract. Relevant articles were criticallyappraised by quality and relevancy criteria. Themethodology considered was as follows: whetherthe study was experimental or observational; if thetrial was randomized, blinded, and the allocationconcealed; what was the sample size, the length offollow-up, the drop out rates; and which outcomeswere used. In addition, the location of the study(the geography, primary or secondary care) wasimportant. If available, the comments of expertson the article were used as described in secondary,referring sources such as the ACP Journal Club.The answer to the patient-orientated questionswas returned to the GP with a list of references onwhich the answer was based. A five-level evidencescore according to Dutch national guidelines wasadded to each answer (see Table 2). The consultedinformation sources were not included.The informationist had the opportunity to askan independent person for their opinion on difficultquestions. GP colleagues from the Department ofGeneral Practice and librarian colleagues from theUniversity Library were occasionally consulted.The informationist did not have any backup forthe times she was on leave from work: questionsthat arrived during these periods were not answereduntil her return.After a few weeks, a short questionnaire foreach posed question with eight items was sent tothe GP. Following this, the GP had the opportunity to see the patient again and inform themabout the results of the evidence-based answeringservice. No instructions were given to the GPs totake notes about their actions or attitudes aroundthe time they received the answer to their question.The questionnaire included questions about theTable 2 Level of evidence (from the Dutch Institute for HealthCare Improvement (CBO)18Level 0Level 1Level 2Level 3Level 4No information foundMeta-analyses or 2 RCTs of high quality2 RCTs of lower quality or nonrandomised trials,cohort studies, case–control studiesOther research studiesExpert opinionRCT, randomized controlled trial.effect of the answer on the GP and on the patient,and the perceived barriers in the GP and in thepatient when implementing the answer. SPSS(version 10.0) was used to analyse the results.ResultsQuestionsBetween March 2000 and April 2002, 21 GPsattended the workshops. Following this, 61 questionsfrom 26 GPs were received; some GPs sent inquestions without having attended the workshop.If necessary, the informationist reformulated thequestion after having consulted the GP. Table 3shows three examples of questions. Most questionswere somatic (93%), focused on therapy (56%) orprognosis (21%). The largest groups of questionsclassified by the International Classification ofPrimary Care (ICPC) were the skin (16%) and thelocomotive apparatus (15%).GPs did not send in many urgent questions: areturn time of more than 3 weeks was acceptablefor 90% of the questions. Only 10% of the questionswere identified as urgent, i.e. labelled by the GPswith a required return time of less than 1 week.Searching and appraisingThe three most used databases for finding theanswer were Medline/PubMed (93%), the CochraneLibrary (80%) and Embase (71%), and is the sameranking order as where the answer was actuallyfound: in Medline/PubMed (40%), the CochraneLibrary (13%), and Embase (8%) ( Table 1). Searchingand appraising articles was quite a time-consumingactivity. The time needed to find and appraiserelevant articles was on average 3 h (range 15 min Health Libraries Group 2004 Health Information and Libraries Journal, 21 (Suppl. 2), pp.27 –35
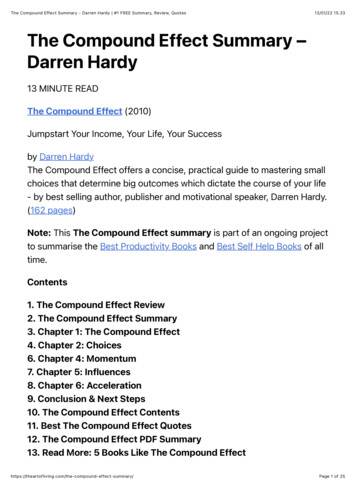
Study of evidence-based answering service, Anita A. H. Verhoeven and Jan SchulingTable 3 Three examples of questions sent in by GPsCase 1QuestionWhat are the effects of intra-articular knee injections with corticosteroids compared with a placebo for severe osteoarthritis inelderly patients?Search strategy and keywordsInformation sources: Cochrane Library, TRIP database, ACP Journal Club, Bandolier, National Guidelines Clearing House,PubMed, Embase, HSTAT, MedlinePlus, CAT, SUMsearch, Clinical Evidence.Keywords (MeSH): Osteoarthritis, injections-intra-articular, anti-inflammatory agents-steroidal, aged.ResultsEvidence found in the Cochrane Library and Clinical Evidence (systematic reviews), and in MedlineKirwan JRR. Intra-articular therapy in osteoarthritis. Baillierres Clinical Rheumatology 1997, 11, 769 –94.Ravau P, Moulinier L, Giraudeau B, Ayral X, Guerin C, Noel E et al. Effects of joint lavage and steroid injection in patients withosteoarthritis of the knee: results of a multicenter, randomized, controlled trial. Arthritis Rheumatism 1999, 42, 475 –82.Answer sent back including quality assessmentThe evidence indicated that intra-articular injections of the knee have a short term benefit only (1-4 weeks) compared with aplacebo. After a month no benefit was measured for pain relief.We found the answer in a systematic review from 1997 which included 10 randomized controlled trials from 1958 to 1996.These results were confirmed by a more recent randomized controlled trial published in 1999.The level of evidence is: 1.Case 2QuestionAre sleeping disorders found more frequently in the pre-menstrual phase than in the pre-ovulatory phase? The reason for thisquestion is a healthy 48-year-old woman, who complains about sleeplessness. She doesn’t use contraceptive pills. Sheassumes the sleeplessness is related to her menstrual cycle. Her question is whether the contraceptive pill is a solution for her.Search strategy and keywordsInformation sources: PubMed, Embase.Keywords in Medline: Menstrual cycle, sleep disordersKeywords in Embase: Ovary cycle, sleep disorder, somnolence, insomnia, menstrual cycle, pre-menstrual syndrome.ResultsWe found evidence in Medline and EmbaseManber R, Bootzin RR. Sleep and the menstrual cycle. Health Psychology 1997, 16, 209 –14.Shibui K, Uchiyama M, Okawa M, Kudo Y, Kim K, Liu X et al. Diurnal fluctuation of sleep propensity and hormonal secretionacross the menstrual cycle. Biological Psychiatry 2000, 48, 1062–8.Answer sent back including quality assessmentIt is plausible that there is a relation between sleep and the menstrual cycle. In one study, thirty-two healthy women kept asleep/awake diary twice a day during two menstrual cycles. In each woman, significant difficulty in falling asleep was reportedduring the luteal phase. Also, a significant reduction of sleep efficiency and sleep quality was reported.In another study, eight healthy women notified a significant higher sleepiness by day during the luteal phase.The level of evidence is: level 2.Case 3QuestionIf a woman with a postpartum psychosis is hospitalised will admission of the baby have a positive effect on the psychosis of themother?Search strategy and keywordsInformation sources: Cochrane Library, Clinical Evidence, Medline, Embase, PsycInfo, TRIP database and SUMsearch.Keywords (MeSH): depression-involutional, treatment outcome, patient admission, mother-child relations, child of impairedparents.ResultsNo evidence was found, only personal opinions. Health Libraries Group 2004 Health Information and Libraries Journal, 21 (Suppl. 2), pp.2 7 – 3531
32Study of evidence-based answering service, Anita A. H. Verhoeven and Jan Schulingto 12 h). Most time was spent on appraising thearticles and in formulating the answer.AnswersOf the answers, 46% were returned within 3 weeks.Only one of the six urgent questions was notreturned in time (but still within 60 days). The GPsindicated that 86% of the questions was returnedin time. In 92% of the questions, the GPs indicatedthat the question was completely or partly answered,although in 36% of the questions no informationwas found. Evidently, no answer to the questioncould be an answer for the GP. The highest level ofevidence was found for only 12% of the questions.Effects and barriers of answersOf the 61 questionnaires about the effects andbarriers of the answers, 48 (87%) questionnaireswere returned. Of the answers, 81% had an effecton the GP. Of the questions for which no information could be found, relatively more answers(89%) had an effect on the GP. Answers with thehighest level of evidence had an effect on the GPin 67% of the cases. On the questionnaire, manyGPs gave examples of effects of implementing theevidence provided by the answer (Table 4). Theanswer could lead to an increase of new knowledgeor to refreshing of old knowledge. It also couldcreate more confidence. An effect on the patientwas noted for 52% of the answers. According tothe GP, patients felt reassured and better informedand gained more knowledge as an effect of theanswer. GPs did not perceive many barriers whenimplementing the answer, either through their ownactions (only 6%), or those of the patient (2%).Barriers noted included the ‘old habits’ of the GPs,and the consultant as an easy model for them tocopy (Table 5). Consultants, who were seen as moreskilled than their GPs, presented a barrier to thepatients’ acceptance of the evidence.DiscussionThis study indicates that the questions posedby the participating GPs largely have a somatic,therapeutic character related to skin and thelocomotive apparatus. These topics are commonin general practice. This finding may indicatethat knowledge among GPs about these topics islimited, but could also indicate that these areas aremore suitable for the formulation of questions asthese topics are not urgent or life-threatening.Of the databases the informationist used, SUMsearch, Bandolier, HSTAT and MedlinePlus didTable 5 Effects of the answer of the evidence-basedanswering service on the patient, and barriers in the patient toimplementing the answer, as perceived and noted by the GPEffect of the answer onthe patient (n)Barrier to implementing answerin the patient (n)Reassurance (7)Better informed (5)Consultant more trustworthy (1)Difficulties with admittingbeing wrong (1)More knowledge (4)Change in referral (2)Relief of symptoms (2)Greater acceptance ofsymptoms (1)Higher quality educationgp trainees (1)Table 4 Effects of the answer of the evidence-based answering service on the GP, and personal barriers experienced by the GPin implementing the answer, as perceived by the GPEffect of the answer on the GP (n)Personal barriers experienced by GP in implementing answer (n)New knowledge (20)Confirmation/validation/more confident of self (12)Refresh old knowledge (5)Prescribing habits due to pharmaceutical commercials (1)Old habits (1)Convenient use of drugs without necessary intake instructionsprevails over those with necessary instructions (1)Consultants as easy model (1)Patients ask for it (1)Advice not applicable on groups or population level (1)More confident with respect to consultant (1)Improvement in relationship with consultant (1)More confident with respect to gp trainees (1)New ideas for research (1) Health Libraries Group 2004 Health Information and Libraries Journal, 21 (Suppl. 2), pp.27 –35
Study of evidence-based answering service, Anita A. H. Verhoeven and Jan Schulingnot add any evidence to the answer, and could bedeleted in the future. In practice, these databasesare being searched to confirm that no (more) evidence has been published. For future work, Web ofScience could be added to the list of databases, asthis is an interdisciplinary database in whichsearching by cited references is possible.A number of lessons were learned by the informationist. During the project, a sense of the searchorder of databases was developed by the informationist, depending on the topic of the question.When many publications were expected, thesearch was started high in the evidence hierarchywith the Cochrane Library or Clinical Evidence.When no or few publications were expected, thesearch was started in Medline. A second lessonwas that the number of relevant articles foundand the time needed to appraise them seemed todepend on the consensus of the management ofthe condition by the medical profession. Somelevels of acceptance by the medical professioncould be detected. Most time (up to 12 h) was spenton searching for information on topics on whichmuch was written, but few or no systematicreviews had been published (e.g. ‘How long does ittake to heal an anal fissure with topical nitroglycerine?’). In addition, a significant amount of timewas spent on responding to questions on controversial topics on which much was published (e.g.‘Do asymptomatic men who have been tested forprostate specific antigen in routine screening forprostate cancer live longer than asymptomaticmen who have not been tested?’). Less than halfan hour was required to answer questions on topicsof which systematic reviews are published, e.g.in the Cochrane Library or in Clinical Evidence(e.g. ‘Does oestrogen replacement therapy in apostmenopausal 58-year-old-woman increase theincidence of endometrial cancer compared with atherapy with progestins added?’), or questions ontopics on which nothing or little was published. Athird lesson was that not the searching itself, butreading and appraising the relevant articles, andformulating an answer took by far the most of theinformationist’s time. This finding that the synthesisof multiple items of evidence into a clinically useful statement has been undervalued in both effortand time was confirmed by research carried outby Ely et al.9In addition to these lessons, the informationistacknowledged the fact that those GPs who werepersonally known to her and were aware of hermedical qualifications were more likely to use theservice and submit questions.The effect of the answer was most evident onthe GPs themselves (in 81% of the questions), farmore than the 20% in Hayward’s study.10 It wasinteresting that the GPs found a ‘no answer available’ result useful in itself. Possibly, they welcomedthat as a strong endorsement of the current practice. Few barriers to implementing the evidencewere formulated by the GPs. Most of the barriersmentioned were related to convenience and habits.A limitation of this study is that the participatingGPs did not represent GPs in general. The participating GPs were interested in evidence-based medicineand they were prepared to attend the PICO workshop.The GPs in this study asked fewer questionsthan mentioned in the literature: in 2 years 26 GPsasked 61 questions. Dutch GPs indicated in aquestionnaire they have seven questions a week;17in other countries the number of questions askedvaried from five questions per patient to 0.5 question per half-day, depending on the methodologyused and the setting.19 23 It is possible that theurgent questions especially (of which answers wereneeded within a week) were not sent to our informationist. We conclude this from the fact that theGPs marked only six of the 61 questions as neededto be returned within a week; all the other questionscould be returned later. They probably assumed theanswering service would take some time to respond.Another possible reason for the low number ofquestions the GPs submitted may be a low awareness of having questions. Therefore, it could beimportant to study the factors that influenceawareness and formulating questions. Structuringquestions into the PICO format could be one ofthe factors that may lower the likelihood ofquestions being asked. Having the knowledgeand skills of structuring questions may enhanceformulating questions. A second recommendationconcerns the impressive number of questions forwhich no answer was found. These questions couldbe used as a pool for research questions. Such newresearch is of high relevancy to medical practice.The evidence-based answering service savedGPs’ time. GPs invested in 11/2 hours of training Health Libraries Group 2004 Health Information and Libraries Journal, 21 (Suppl. 2), pp.2 7 – 3533
34Study of evidence-based answering service, Anita A. H. Verhoeven and Jan Schulingtime, followed by approximately 5 min to fill in therequest form for each question. The informationistundertook the searching and appraising, whichtook an average of 3 h. It is estimated that even forthe first question, more than an hour of the GP’stime was saved.Comparing this evidence-based answeringservice with Hayward’s study,10 the present servicewas more vulnerable. Hayward’s service was staffedby three persons for 1 month, the present studywas staffed by one part-time informationist for2 years. Characteristics of the questions were quitesimilar. In Swinglehurst’s information service12 theinformationist was also a part-time GP. The timeneeded to answer questions was on average 9 days;in Hayward’s study this was 3 days. In the presentstudy, 90% of the questions were labelled by theGPs to have a return time of more than 1 week,which gave the informationist more time to answerthe questions. Both Hayward’s and Swinglehurst’sstudy confirmed the time consuming process ofrequiring access to and critical appraisal of the fulltext articles. The ATTRACT study11 was especiallycreated to provide rapid, evidence-based summaries to clinical questions (within 6 h) and staffed byan information manager. All these studies promoted the usefulness of an evidence-based answering service, and 20–55% of the GPs indicated thatthe given answers had an effect on their patients.ConclusionThis study indicates that clinical questions on patientcare answered using the principles of evidence-basedmedicine could have a high impact on GPs andtheir patients. Although no evidence was found inone-third of the questions, this finding still had animpact on the majority of the GPs. These questionswithout evidence-based answers could be developedas a source for future research. Significant barriers toimplementation of the evidence were not perceived.References1 Brettle, A. Information skills training: a systematic reviewof the literature. Health Information and Libraries Journalof 2003, 20(S1), 3 – 9.2 Snowball, R. ‘Find the evidence’: reflections on aninformation skills course for community-based clinicalhealth-care staff at the Cairns Library, Oxford. HealthInformation Libraries Journal of 2002, 19, 109–12.3 Sackett, D. L., Straus, S. E., Richardson, W. S.,Rosenberg, W. & Haynes, R. B. Evidence-Based Medicine:How to Practice and Teach EBM. Edinburgh: ChurchillLivingstone 2000.4 McColl, A., Smith, H., White, P. & Field, J. Generalpractitioners’ perceptions of the route to evidence-basedmedicine: a questionnaire survey. BMJ 1998, 316, 361–5.5 F
time.5 9 Therefore, an evidence-based answering service for GPs10 14 was introduced in which liter-ature searching, appraising of relevant articles, and formulating the answer was taken over by an informationist.15 This study will describe the characteristics of the authors' evidence-based answering service, the