Transcription
Dr Nick McIvorDr John ChaplinHead & Neck SurgeonNorth Shore HospitalAuckland City HospitalAucklandAuckland Expert RhinoplastySurgeonGillies HospitalAuckland14:00 - 14:55 WS #48: Managing Thyroid Nodules15:05 - 16:00 WS #60: Managing Thyroid Nodules (Repeated)
Thyroid nodulesAucklandHead & NeckAssociatesJohn ChaplinNick McIvorThyroid & Head and Neck SurgeonsAucklandAuckland Head and Neck Associates
Thyroid NoduleAucklandHead & NeckAssociates Common–––––3-5% palpable50-70% ultrasoundIncrease with ageMore in women95% benign
Thyroid NoduleAucklandHead & NeckAssociates What do you want toknow?Auckland Head and Neck Associates
Thyroid NoduleAucklandHead & NeckAssociates What do you want toknow?– Is it malignant?– Is it toxic?– Is it compressive?– Cosmetic effect?Auckland Head and Neck Associates
Is it malignant?AucklandHead & NeckAssociates 5% malignant– Decision algorithm for resectionbased on combination of: Clinical– History– examination Cytology Bloods Radiology– Ultrasound– CT/ MRIAuckland Head and Neck Associates
Is it malignant?is it important?Auckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it malignant?is it important?Korea’s Thyroid-Cancer “Epidemic”— Screening and Overdiagnosisn engl j med 371;19 nejm.org november 6, 2014Auckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it malignant?is it important?Auckland Head and Neck Associatesn engl j med 371;19 nejm.org november 6, 2014AucklandHead & NeckAssociates
Is it malignant?is it important?JAMA. 2006 May 10;295(18):2164-7.Increasing incidence of thyroid cancer in the United States, 1973-2002.Davies L1, Welch HG. 2.4-fold increase in incidence of thyroid cancer from 1973 to 2002 Virtually the entire increase is attributable to an increase in incidence of papillary thyroidcancer. No significant change in the incidence of the less common histological types:follicular, medullary, and anaplastic 49% of the increase consisted of cancers measuring 1 cm or smaller 87% consisted of cancers measuring 2 cm or smaller. Mortality from thyroid cancer was stable between 1973 and 2002 (approximately 0.5deaths per 100,000).Auckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it malignant?is it important?JAMA. 2006 May 10;295(18):2164-7.Increasing incidence of thyroid cancer in the United States, 1973-2002.Davies L1, Welch HG.CONCLUSIONS: The increasing incidence of thyroid cancer in the United States is predominantly due tothe increased detection of small papillary cancers. These trends, combined with the known existence of a substantial reservoir of subclinicalcancer and stable overall mortality, suggest that increasing incidence reflects increaseddetection of subclinical disease, not an increase in the true occurrence of thyroid cancer.AucklandHead & NeckAssociates
Is it malignant?is it important?AucklandHead & NeckAssociatesATA guidelines –investigate suspicious nodules that are at least 1cm in size
Is it malignant?historyAucklandHead & NeckAssociates Risk Factors– Family history Papillary––––95% sporadic5% RET-PTC gene mutationx2 first degree 50%X3 first degree 97% Medullary– 25% Syndromic– Familial MTC– MEN 2a, 2b» RET oncogene mutations– Radiation exposure Therapeutic Environmental– Nuclear» power plants» weapons– VolcanoesAuckland Head and Neck Associates
Is it malignant?clinicalAucklandHead & NeckAssociates– Nodule90%– Can be nodule in MNG– Nodes– Extrathyroid 10%3-5%HoarsenessAirwayDysphagiaSkin– Distant3-5%Auckland Head and Neck Associates
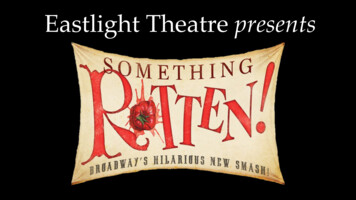
Is it malignant?ultrasound AucklandHead & NeckAssociatesSolidHypoechoicTaller than wide shapeIrregular marginMicrocalcification Associated nodes with similarfeaturesTIRADS 1-6Auckland Head and Neck Associates
Malignant thyroid nodulesAucklandHead & NeckAssociates
AucklandHead & NeckAssociates
Is it malignant?US guided FNA cytologyFNA is a safe test with negligible risk of seedingAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it malignant?FNA cytologyBethesda 50-60%97-100%Non diagnosticBenignAtypical follicularFollicular neoplasmSuspicious for cancerCarcinomaAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it malignant?FNA cytologyBethesda 50-60%97-100%Non diagnosticBenignAtypical follicularFollicular neoplasmSuspicious for cancerCarcinomaAucklandHead & NeckAssociatesobservation vs surgerysurgeryAuckland Head and Neck Associates
Is it malignant?FNA cytologyBethesda 50-60%97-100%Non diagnosticBenignAtypical follicularFollicular neoplasmSuspicious for cancerCarcinomaAucklandHead & NeckAssociatesrepeat FNAobservation vs surgeryrepeat FNA vs surgerysurgeryAuckland Head and Neck Associates
Is it malignant?bloodsAucklandHead & NeckAssociatesTSH, T3, T4- standard. TSH usually normal in ca.Rapid swelling with hypothyroid consider lymphoma? Thyroglobulin, Tg Ab- useful for surveillance? Calcitonin- ?Bethesda 4-6 solitary nodule, FHAuckland Head and Neck Associates
Is it toxic/hypothyoid?History/exam Toxic Heat intoleranceIrritabilityTremorExopthalmosLid lagGoitre/ nodule Hypothyroid FatigueSluggish reflexesOedemaAlopeciaDry skin May be subclinicalAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it toxic/hypothyroid?Bloods Thyrotoxic––––AucklandHead & NeckAssociates HypothyroidTSH supressedT4, T3 elevatedThyrd Abs ve in 50% GravesThy Stim Ig ve in Graves– TSH elevated– T3,T4 low– Thyroid Abs ve 90%TSH most senstive. ie. can have altered TSH without T3, T4Auckland Head and Neck Associates
Thyroid function PathologyFirst line therapy Hyper thyroidAucklandHead & NeckAssociates Hypothyroid– Antithyroid Drugs– Repacement Carbimazole PTU – B blockers– Weekly TFT until euthyroidthen 3 monthlyThyoxineWTERepeat bloods 6-8/526/12- 1 yr once euthyroid (or if pregnant)Auckland Head and Neck Associates
TSH supressed & TSHr –ve(partic with nodule or goitre)Scintiscan Toxic Goitre Toxic Nodule(s)Toxic nodules are almost never malignantAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
ThyrotoxicosisDefinitive: surgery vs radio-iodine RAI Surgery– Advantages– Advantages Single treatment Minimal riskhypothyroidism inipsilateral nodule Reduced dysthyroid eyedisease in Graves Better for toxic goitre– Disadvantages Scar complications No surgery May be better in smallGraves without eyedisease– Disadvantages Need repeat doses in largethyroid Risk of hypothyroid intoxic nodule Does not remove antigenAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it compressive?AucklandHead & NeckAssociates eCoughShort of breathExercise intoleranceOSAAuckland Head and Neck Associates
Globus PharyngeusAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Is it compressive? Signs– Stridor, wheeze, SOB– Absent lower border/ dull topercussion thorax– Sleep apnoea– Pemberton’s signAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Compressive goitre Investigations– Resp function tests Fixed obstruction– Laryngeal exam Endoscopy Voice analysis– CT Thoracic extension Airway compromise RecurrenceAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Thoracic goitre CT– Shows thoracic extension– Allow planning of access– Rare to split sternum but needCTSU surgeonAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
CosmesisAucklandHead & NeckAssociates Trade off:– Nodule vs scar– Risk op vs no opAuckland Head and Neck Associates
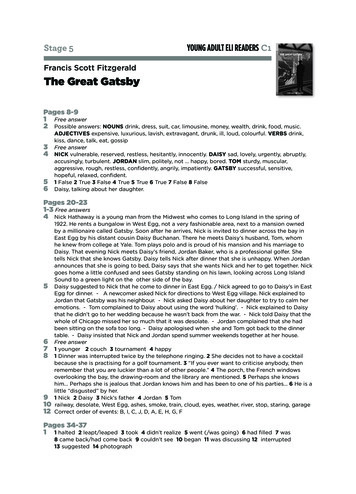
Case 1 50 yr old man Hard masslow right neck FNA mass suggestsbenign thyroidfollicular cellsAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 1 What is this most likely to be.––––a. metastatic thyroid cancerb. benign thyroid cystc. lateral aberrant thyroid tissued. pathologist errorAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 1 What is this most likely to be.––––a. metastatic thyroid cancerb. benign thyroid cystc. lateral aberrant thyroid tissued. pathologist errora. Metastatic thyroid cancerAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 1 Papillary cancer is welldifferentiated and cells canlook benign. Nodal mass won’t elevatelike thyroid even though insame position Epithelial cells don’t belongin a lymph nodeAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 2 20 yr old woman Month history of very sorethroat, pain on cough andswallow radiating to ears. Very tender and hard rightthyroid nodule T4 32, TSH 0.002 ESR 40 No toxic symptoms or signsAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 2Most likely diagnosisa.b.c.d.Subacute thyroiditisGraves diseaseBleed into a thyroid noduleHashimotos thyroiditisAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 2Most likely diagnosisa.b.c.d.Subacute thyroiditisGraves diseaseBleed into a thyroid noduleHashimotos thyroiditisa. Subacute or de Quervain’s or painful thyroiditisAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
de Quervains subacute thyroiditisWhat is best confirming test?a. FNAb. Ultrasoundc. Thyroid lobectomyd. scintigraphyAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
de Quervains subacute thyroiditisWhat is best confirming test?a. FNAb. Ultrasoundc. Thyroid lobectomyd. scintigraphyd. scintigraphy- shows reduced uptake in glandAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
de Quervains subacute thyroiditis Inflammatory condition– Thought to be viral origin (occurs in clusters)– Can be ipsilateral, bilateral or sequential– Ultrasound can show a suspicious, infiltrative pattern– FNA Painful, shows inflammatory lymphocytes with giant cells– Treatment Responds very well to anti-inflammatory steroids– Follow up Repeat thyroid function tests monthly as high risk of developinghypothyroidismAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 3 35 yr old woman Sudden 3cm right thyroid swelling Ultrasound shows part fluid, partsolid mass Tender to palpationAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 3 Most likely diagnosisa.b.c.d.Thyroid cancerViral thyroiditisBleed into noduleThyroid abscessAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 3 Most likely diagnosisa.b.c.d.Thyroid cancerViral thyroiditisBleed into noduleThyroid abscessc. bleed into noduleAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 5AucklandHead & NeckAssociatesFollowing thyroidectomy for thyroid cancer what are theusual follow-up blood tests?a.b.c.d.TSH onlyTSH, T3, T4TSH, Thyroglobulin onlyTSH, Thyroglobulin, Thyroglobulin AbAuckland Head and Neck Associates
Case 5AucklandHead & NeckAssociatesFollowing thyroidectomy for thyroid cancer what are theusual follow-up blood tests?a.b.c.d.TSH onlyTSH, T3, T4TSH, Thyroglobulin onlyTSH, Thyroglobulin, Thyroglobulin Abd. TSH, Thyroglobulin, Thyroglobulin AbAuckland Head and Neck Associates
Case 6Thyroglobulin in the normal range following totalthyroidectomy for PTC, radioactive iodine and thyroidreplacement indicates .?a.b.c.d.No cancer, adequate thyroid replacementNo cancer, inadequate thyroid replacementPersisting cancerCan’t tell – need scansAuckland Head and Neck AssociatesAucklandHead & NeckAssociates
Case 6AucklandHead & NeckAssociatesThyroglobulin in the normal range following totalthyroidectomy for PTC, radioactive iodine and thyroidreplacement indicates .?a.b.c.d.No cancer, adequate thyroid replacementNo cancer, inadequate thyroid replacementPersisting cancerCan’t tell – need scansc.Auckland Head and Neck AssociatesPersisting cancer
Case 7AucklandHead & NeckAssociates 27 year old woman2.8cm right noduleNo nodesFNA PTC- Bethesda 6What other tests?
Case 7 AucklandHead & NeckAssociatesA. CT scan?B. MRI scan?C. Laryngoscopy?D. all of above?D All of the aboveD. All of above
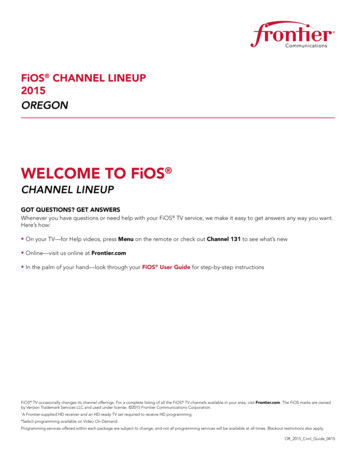
Case 7AucklandHead & NeckAssociates Booked for total thyroidectomy At surgery extension into extrathyroid tissues posteriorlyadherent to RLN Good case for nerve monitoring?
RLNAucklandHead & NeckAssociatesAuckland Head and Neck Associates
Case 8 31 yr old woman Previous total thyroidand level 6 neckdissection London UK 2yrs prior Rising Thyroglobulin –ve Tg abs Palpable right lateralnodeAucklandHead & NeckAssociates What is appropriate initial investigation––––A. Radioiodine scanB. Chest XRC. Neck ultrasoundD. FNA
Case 8C. Neck ultrasoundAucklandHead & NeckAssociates
Case 8AucklandHead & NeckAssociates Surgery mainstay treatment of recurrence
Thyroid nodulesAucklandHead & NeckAssociatesJohn ChaplinNick McIvorThyroid & Head and Neck SurgeonsAucklandAuckland Head and Neck Associates
Increasing incidence of thyroid cancer in the United States, 1973-2002. Davies L1, Welch HG. 2.4-fold increase in incidence of thyroid cancer from 1973 to 2002 Virtually the entire increase is attributable to an increase in incidence of papillary thyroid cancer. No significant change in the incidence of the less common histological types: