Transcription
Coding DermatologyProceduresPresented by: Betty A HoveyDirector, ICD-10 Development and TrainingAAPC1
No part of this presentation maybe reproduced or transmitted inany form or by any means(graphically, electronically, ormechanically, includingphotocopying, recording, or taping)without the expressed writtenpermission of AAPC.2
CPT copyright 2012 American Medical Association. All rightsreserved. Fee schedules, relative value units, conversion factors and/orrelated components are not assigned by the AMA, are not partof CPT, and the AMA is not recommending their use. The AMA isnot recommending their use. The AMA does not directly orindirectly practice medicine or dispense medical services. TheAMA assumes no liability for data contained or not containedherein. CPT is a registered trademark of the American MedicalAssociation. The responsibility for the content of any “National CorrectCoding Policy” included in this product is with the Centers forMedicare and Medicaid Services and no endorsement by theAMA is intended or should be implied. The AMA disclaimsresponsibility for any consequences or liability attributable to orrelated to any use, nonuse or interpretation of informationcontained in this product.3
AGENDA AnatomyShaving of LesionsExcision of LesionsRepairsAdjacent Tissue TransferDestruction of LesionsMohs Micrographic Surgery4
5
Skin Cancer While skin cancers can be found on any part ofthe body most (about 80%) appear on the face,head, or neck The primary cause of skin cancer is ultravioletradiation -most often from the sun Also from artificial sources like sunlamps andtanning booths6
Skin CancerBCC Basal cell carcinoma is the most common formof skin cancer, affecting 800,000 Americanseach year The most common of all cancers 1 out of every 3 new cancers is a skin cancer Most are basal cell carcinomas (BCC) These cancers arise in the basal cells, whichare at the bottom of the epidermis More common in men, although more womenare getting BCCs than in the past7
Skin CancerWarning Signs of BCC1. Open sore that bleeds, oozes, or crustsand remains open for three or moreweeks2. A reddish patch or irritated area,frequently occurring on the chest,shoulders, arms, or legs3. Shiny bump, or nodule, that is pearly ortranslucent and is often pink, red, or white8
Skin CancerWarning Signs of BCC4. Pink growth with a slightly elevated rolledborder and a crusted indentation in thecenter5. Scar-like area which is white, yellow orwaxy, and often has poorly definedborders9
Skin Cancer SCCSquamous cell carcinoma (SCC), the secondmost common skin cancer after basal cellcarcinomaAfflicts more than 200,000 Americans eachyearArises from the epidermis and resembles thesquamous cells that comprise most of theupper layers of skinSCCs may occur on all areas of the body butare most common in areas exposed to thesun10
Skin Cancer1.2.3.4.Warning Signs of SCCA wart-like growth that crusts andoccasionally bleedsA persistent, scaly red patch with irregularborders that sometimes crusts or bleedsAn open sore that bleeds and crusts andpersists for weeksAn elevated growth with a centraldepression that occasionally bleeds. Agrowth of this type may rapidly increase insize11
Skin Cancer MelanomaMost serious form of skin cancerIf diagnosed and removed early it is almost100% curableOnce it metastasizes (spreads) to other partsof the body, it is hard to treat and can bedeadlyNumber of cases has increased more rapidlythan any other cancer over the past 10 yearsOver 51,000 new cases are reported to theAmerican Cancer Society each year12
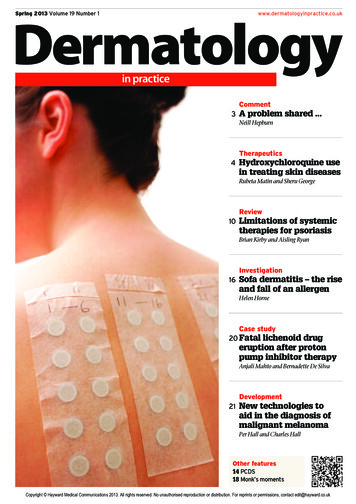
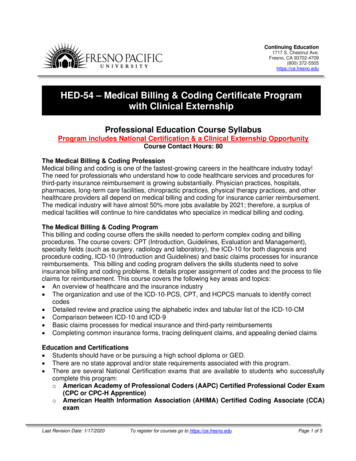
Skin Cancer1ABenign vs. Malignant3ASymmetrical2AEven Borders1BAsymmetrical2BUneven BordersOne Shade4ASmall than ¼”3BTwo/More Shades4BLarger than ¼”13
Skin CancerICD-9-CM Coding Chapter 2 of the ICD-9-CM contains thecodes for most benign and all malignantneoplasms. Certain benign neoplasms,such as prostatic adenomas, may be foundin the specific body system chapters. Toproperly code a neoplasm it is necessary todetermine from the record if the neoplasmis benign, in-situ, malignant, or of uncertainhistologic behavior. If malignant, anysecondary (metastatic) sites should also bedetermined.14
Skin Cancer Do not go to the Neoplasm Table first Reference histological term first, if given Melanoma a good example of when goingdirectly to the Table is not a good idea15
Skin Cancer Primary malignancy previously excised When a primary malignancy has been previouslyexcised or eradicated from its site and there is nofurther treatment directed to that site and there isno evidence of any existing primary malignancy, acode from category V10, Personal history ofmalignant neoplasm, should be used to indicate theformer site of the malignancy. Any mention ofextension, invasion, or metastasis to another site iscoded as a secondary malignant neoplasm to thatsite. The secondary site may be the principal orfirst-listed with the V10 code used as a secondarycode.16
TREATMENT OPTIONS Topical MedicationsCurettage and ElectrodessicationExcisional SurgeryRadiationMohs Micrographic SurgeryCryosurgeryLaser SurgeryPhotodynamic Therapy (PDT)17
ShaveCPT DefinitionShaving is the sharp removal bytransverse incision or horizontal slicing toremove epidermal and dermal lesionswithout a full-thickness dermal excision.This includes local anesthesia, chemicalor electrocauterization of the wound. Thewound does not require suture closure.18
11300 Shaving ofepidermal or dermallesion, single lesion,trunk, arms or legs;lesion diameter 0.5cm or less11305 Shaving ofepidermal or dermallesion, single lesion,scalp, neck, hands,feet, genitalia; lesiondiameter 0.5 cm orless11310 Shaving ofepidermal or dermallesion, single lesion,face, eyelids, nose,lips, mucousmembrane; lesiondiameter 0.5 cm orless11301 lesion diameter0.6 cm to 1.0 cm11306 lesion diameter0.6 cm to 1.0 cm11311 lesion diameter0.6 cm to 1.0 cm11302 lesion diameter1.1 cm to 2.0 cm11307 lesiondiameter 1.1 cm to 2.0cm11312 lesion diameter1.1 cm to 2.0 cm11303 lesion diameterover 2.0 cm11308 lesion diameterover 2.0 cm11313 lesion diameterover 2.0 cm
ExampleThe dermatologist shaved three epidermallesions that the patient chose not to havesubmitted to pathology: a 0.4 cm lesion fromthe patient’s chest, a 0.3 cm lesion from thepatient’s back, and a 0.2 cm lesion from thepatient’s forehead. 11310, 11300, 11300-59(modifier 51 may be needed depending onpayer)20
ExcisionCPT DefinitionExcision is defined as full-thickness(through the dermis) removal of lesion,including margins, and includes simple(non-layered) closure when performed Deeper than a shave (partial thickness)21
ExcisionCode selection is determined by measuringthe greatest clinical diameter of the apparentlesion plus that margin required for completeexcision (lesion diameter plus the mostnarrow margins required equals the exciseddiameter).The margins refer to the most narrow marginrequired to adequately excise the lesion,based on individual judgment.The measurement of the lesion plus marginis made prior to excision.22
ExcisionExcised diameter examples 1 cm melanoma with 2 cm necessarymargins is excised from patient’s back– 1 4 5 cm excised diameter lesion 11606 2 cm benign lesion with 2 cm margins, but0.2 cm necessary margins is excised frompatient’s neck– 2 0.4 2.4 cm excised diameter lesion 1142323
ExcisionCoding Lesion Excisions Benign v Malignant Anatomic Site Size (excised diameter) Type of Repair24
Excision The type of repair is important with excisionof lesions as simple repairs are bundled intothe excision codes per CPT guidelines. Layered and complex repairs are separatelyreportable. When an excision and repair are separatelyreported, modifier 51 may be necessarywhen reporting (payer issue).25
ExampleA physician refers a patient to the dermatologistfor excision of a “mole” on the patient’s leftcheek. The dermatologist suspects that themole is a small basal cell carcinoma (laterconfirmed pathologically). She performs anexcision to remove the 0.9 cm excised diameterlesion in the office. She then closes the woundvia simple repair. 11641 (repair not separately reported) 173.3126
ExampleA patient is seen for excision of a biopsyproven squamous cell carcinoma on hisback. The 4.2 cm excised diameter lesionrequires a 6.3 cm intermediate repair. 11606, 12032 (possible modifier 51) 173.5227
VIDEO DEMONSTRATINGLESION EXCISION WITHINTERMEDIATE REPAIR28
RepairRepair Coding Type of Repair Site of Repair Size of Repair When to Add Repairs29
Repair CPT defines a wound closure as a closure“utilizing sutures, staples, or tissue adhesives(eg, 2-cyanoacrylate), either singly or incombination with each other, or in combinationwith adhesive strips. If adhesive strips (i.e., butterfly) alone are used,then it is bundled in to the E/M service.30
RepairTypes of Repair Simple repair Intermediate repair– Single-layer closure of heavily contaminatedwounds that have required extensive cleaningor removal of particulate matter alsoconstitutes intermediate repair. Complex repair31
Repair According to the CPT manual we addtogether repairs when they are the sameclassification (simple, intermediate, complex)and the same anatomic grouping (scalp, arms,etc.). For example, you would add together a 4.0 cmsimple repair of the abdomen, a 5.6 cm simplerepair of the back, and a 2.2 cm simple repair ofthe chest as one 11.8 cm simple repair to thetrunk (12004).32
Repair But, when more than one classification of woundis repaired, they are reported separately. Themost complicated repair is listed as the primaryprocedure and the less complicated is listed asthe secondary procedure, with the modifier 51attached (depending on the payer).33
ExampleA patient has 2 benign lesions excised. Thefirst one is a 2.1 cm excised diameter lesionon the forehead, the second is a 2.5 cm onthe cheek. They both require intermediaterepair -2.6 cm on the forehead and 3.0 cmon the cheek. 12053, 11443, 11443-59 216.334
Adjacent Tissue Transfer Codes 14000-14302 are used for excision(including lesion) and/or repair by adjacenttissue transfer or rearrangement Z-plasty, W-plasty, V-Y-plasty Rotation flap Random island flap Advancement flap35
Adjacent Tissue Transfer What’s not an ATT? Secondary defect closure Size for code selection36
Adjacent Tissue TransferDefect examples Advancement flap performed with aprimary defect from excision of 1.0 cm X1.0 cm and secondary defect for flapdesign of 2.0 cm X 1.0 cm.– 1.0 sq cm 2.0 sq cm 3.0 sq cm Rotation flap performed with primary defectfrom excision 1.0 cm X 1.0 cm andsecondary defect for flap design 2.5 cm X1.2 cm– 1.0 sq cm 3.0 sq cm 4.0 sq cm37
Adjacent Tissue TransferATT Coding Bundling of lesion excision Site Size in square centimeter Additional coding38
ExampleExcision of basal cell carcinoma on nosewith rotation flap for closure. The lesion was2.1 cm X 1.5 cm. The secondary defectmade to perform the ATT was 4.5 cm X 2.5cm. 14061 173.3139
Destruction Codes 17000 – 17004 Codes 17110 and 17111A parenthetical note is under 17003 thatstates plantar or common warts are to bereported with 17110 and 17111. Numbers game40
Example 12 AKs and 9 SKs were destroyed in thesame session 17000, 17003 X 11 for the destruction ofthe AKsAND 17110 for the destruction of the SKs41
Mohs Micrographic Surgery Mohs is a highly specialized procedure fortreatment of skin cancers. Mohs allows for complete removal of skincancer at one session. It has the highest cure rates for squamousand basal cell carcinomas. The physician acts as surgeon andpathologist.42
Mohs Micrographic Surgery 17311Mohs micrographic technique, includingremoval of all gross tumor, surgical excision of tissuespecimens, mapping, color coding of specimens,microscopic examination of specimens by the surgeon, andhistopathologic preparation including routine stain(s) (eg,hematoxylin and eosin, toluidine blue), head, neck, hands,feet, genitalia, or any location with surgery directly involvingmuscle, cartilage, bone, tendon, major nerves, or vessels;first stage up to 5 tissue blocks 17312each additional stage after the firststage, up to 5 tissue blocks43
Mohs Micrographic Surgery17313Mohs micrographic technique, includingremoval of all gross tumor, surgical excision of tissuespecimens, mapping, color coding of specimens,microscopic examination of specimens by the surgeon,and histopathologic preparation including routine stain(s)(eg, hematoxylin and eosin, toluidine blue), of the trunkarms, or legs; first stage up to 5 tissue blocks 17314each additional stage after thefirst stage, up to 5 tissue blocks44
Mohs Micrographic Surgery 17315Mohs micrographic technique,including removal of all gross tumor, surgicalexcision of tissue specimens, mapping, colorcoding of specimens, microscopic examination ofspecimens by the surgeon, and histopathologicpreparation including routine stain(s) (eg,hematoxylin and eosin, toluidine blue), eachadditional block after the first 5 tissue blocks, anystage45
Example A physician performs Mohs surgery on a patientwith a basal cell carcinoma on his cheek. Thephysician takes the first stage with 6 tissueblocks, but does not remove all of the cancer. Asecond stage is removed with 4 tissue blocks.The second stage comes back and shows thatthe physician completely excised the cancer. 17311, 17312, 17315 173.3146
MohsLIVE SURGICALPICTURES ANDVIDEO OF MOHSSURGERY47
Thank YouENJOY THEREST OFCONFERENCE!48
Sources Mohs video allowed by permission of RichardDeAngelis, M.D. from Skin Cancer Centre inAnderson, S.C. www.skincancercentre.com Lesion excision video allowed by permissionof Adrian Richards, M.D. from Aurora PlasticSurgery and Cosmetic Centres, UnitedKingdom www.aurora-clinics.co.uk CPT 2013 Professional Edition ICD-9-CM 201349
American Cancer Society each year Skin Cancer 12 . Skin Cancer Benign vs. Malignant Symmetrical Asymmetrical 1A 1B Even Borders Uneven Borders . This includes local anesthesia, chemical or electrocauterization of the wound. The wound does not require suture closure. Shave 18 . 11300 Shaving of epidermal or dermal