Transcription
ReconstructiveDepartmentOptimizing the Closed Suction SurgicalDrainage SystemKatherine H. Carruthers, MSBradley S. Eisemann, MDSusan Lamp, BSN, RN, CPSNErgun Kocak, MD, MSBackground: Closed suction drainsare indicated in a wide array ofpostoperative settings, with manydistinct drainage systems available tothe surgeon. The purpose of this studywas to compare the suction gradientsKatherine H. Carruthers, MS, is amedical student at the University of ToledoCollege of Medicine in Toledo, Ohio.She recently earned a master’s degree inBiomedical Sciences at the University ofToledo College of Graduate Studies and iscurrently completing the first year of hermedical education.Bradley S. Eisemann, MD, graduatedfrom University of Texas Medical School atHouston and is now a first-year residentin the Department of Surgery, Division ofPlastic Surgery at the Baylor College ofMedicine in Houston, Texas.Susan Lamp, BSN, RN, CPSN, is a plasticsurgery nurse in the Department of PlasticSurgery at The Ohio State University’sWexner Medical Center in Columbus,Ohio. She is the editor of the ASPSNewsand serves on the PSN Journal EditorialBoard as the chair of the ReconstructionDepartment.Ergun Kocak, MD, MS, is an AssistantProfessor in the Department of PlasticSurgery at The Ohio State University’sWexner Medical Center. He completed hisresidency in plastic surgery at The OhioState University and continued his trainingwith a microsurgical fellowship at the M.D.Anderson Cancer Center in Houston, Texas.The authors report no conflicts of interest.Address correspondence to Ergun Kocak,MD, MS, 915 Olentangy River Road, Suite2100, Columbus, OH 43212 (e-mail:ergun.kocak@osumc.edu).DOI: 10.1097/PSN.0b013e31828425db38achieved using 2 different sizes ofsuction reservoirs and 2 differenttechniques for generating negativepressure.Materials and Methods: Drainagereservoirs of 100 and 400 ml werechosen to evaluate their ability toachieve suction. Suction was established in both sizes of drains by pressing the sides of the reservoir togetheror by pushing the bottom of the reservoir toward the top. Negative pressures were recorded with the reservoirempty, and after every 10-ml additionof saline. Averages were graphed toillustrate the applied suction over arange of drain volumes.Results: The 100-ml drainagesystem reached a peak suction of 117.6 mmHg, while the 400-mldrainage system reached only a peaksuction of 71.4 mmHg. Both ofthe maximum suction readings wereachieved using the full-squeeze technique. The bottom-pushed-in technique did not result in any sustainedmeasurable levels of suction usingeither of the reservoir volumes.Conclusions: Smaller drain reservoirsare more successful in generatinga high initial suction than largerreservoirs, especially when the volumeof fluid in the drain is relatively low.In all sizes of drains, compressing thePlastic Surgical Nursing CEsides of the reservoir is a far bettertechnique for establishing negativepressure than pressing the bottom ofthe drain up toward the top.Closed suction surgical drainagesystems are routinely used whenthere is a postoperative risk ofseroma development (Zawaneh& Putnam, 2008). Because of thefrequent use of surgical drains,several different variations ofdrains have been developed, witha range of reservoir volumes andshapes. However, despite somephysicians’ preferences to uselarger drainage reservoirs, manypatients comment that they findthese larger bulbs to be cumbersome and inconvenient duringtheir postoperative recovery, andthat they would have preferredsmaller reservoirs if they couldbe confident that they providedcomparable drainage. Furthermore, there are several methodsof compressing these reservoirsto generate the negative pressure needed to pull collectedfluid from the surgical wound(Figure 1). In the plastic surgical setting, drainage systemsare especially important whenperforming certain operations,such as latissimus muscle flapsor breast reconstructions thatrequire elevating abdominalJanuary–March 2013 Volume 33 Number 1Copyright 2013 American Society of Plastic Surgical Nurses. Unauthorized reproduction of this article is prohibited.PSN200241.indd 3813/02/13 2:06 AM
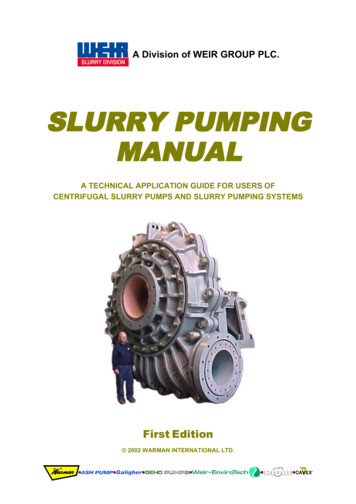
Figure 1. Actual photo of a patient with two 100-ml Jackson-Pratt drainsplaced in the abdomen. It can be observed that the drain with the side-to-sidefull-squeeze method for obtaining closed suction has begun to collect serousfluid, while the drain with the bottom-pushed-in method still appears to beempty.tissue, as these procedures areknown to have especially highrates of seroma formation(Scevola, Youssef, Kroll, & Langstein, 2002). Seromas that arenot properly drained can causedelayed wound healing or evenflap necrosis. Thus, it is vital toensure that the surgeon’s technique for applying suction andchoice of drain reservoir volumemaximize the ability of the drainage system to apply negativepressure to the potential space.Because of the wide range ofreservoir sizes and methods forestablishing negative pressure,it must be wondered whethercertain combinations are moresuccessful than others at drawing fluid out of the surgicalwound. The ability to effectivelyremove fluid more completelycould potentially reduce complications traditionally associated with flap elevation andeven facilitate patient recovery(Durai, Mownah, & Ng, 2009).The goal of this study was toobjectively analyze the suctiongenerated by drains with twocommon reservoir sizes andto compare the negative pressure attained by two frequentlyobserved techniques for achieving closed suction.Plastic Surgical Nursing January–March 2013MATERIALS AND METHODSAir was removed from 100-mlBard (Bard Medical Division,Covington, GA) and 400-ml Jackson-Pratt (Baxter HealthcareCorp., Deerfield, IL) surgicaldrain reservoirs by either squeezing the sides together (Figure 2a)or pushing the bottom towardthe top (Figure 2b). Of the twoports on the top of each drainreservoir, one port was connected to 80 cm of 19 French reservoir tubing with a three-waystopcock (Bard Medical Division), allowing for saline to beinjected into the drain reservoirin known volumes. The otherport was connected with similartubing to a sphygmomanometer(Figure 3). This device measurespressures ranging from 20 to 300 mmHg. Suction readingswere repeated five times, andmeasurements were obtained tothe nearest 1.0 mmHg with thedrain empty and after each subsequent injection of 10 ml ofsaline until the reservoir reachedcapacity or until level of suctiondropped below the measurablevalue of 20 mmHg.Average negative pressures foreach size of reservoir and for eachmethod of removing air from theFigure 2. Air was removed from surgical drain reservoirs to generate negativepressure by either (a) squeezing the sides together or (b) pushing the bottomtoward the top. Volume 33 Number 139Copyright 2013 American Society of Plastic Surgical Nurses. Unauthorized reproduction of this article is prohibited.PSN200241.indd 3913/02/13 2:06 AM
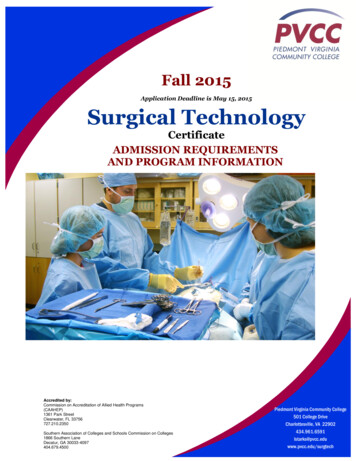
Figure 3. After removal of the air from the drain reservoir, one of the twoports on the top was connected to tubing with a three-way stopcock, allowingfor saline to be injected into the drain reservoir in known volumes. The secondport was connected with similar tubing to a sphygmomanometer to measurethe suction of the drainage system.reservoir were calculated with thedrain empty and after each addition of saline. The resulting datawere graphed to illustrate theapplied suction achieved over arange of drain collection volumes(Figures 4 and 5).RESULTSUsing the side-to-side full-squeezetechnique, drains with 100-ml reservoirs reached an average maximum negative pressure of 117.6mmHg (Table 1a). This value wasachieved with the reservoir emptyand the suction slowly droppedas the volume of retained salineincreased. By the time the reservoir was filled to 60 ml of saline,the suction had dropped below arecordable level. Similar resultswere obtained using the side-toside full-squeeze technique andthe 400-ml reservoir. Using the400-ml reservoir, the averagemaximum negative pressure was 71.4 mmHg, again achievedwhen the drain was empty (Table2a). A p value of less than .05was calculated when comparingthe maximum suction obtainedwhen using the 100-ml and 400ml reservoirs and the side-to-sidefull-squeeze technique. As withFigure 4. Using a 100-ml Bard drainage system, average suction was measuredusing either the full side-to-side squeeze or the bottom-pushed-in techniqueof generating negative pressure. Measurements were repeated five times andmeans were reported the standard deviation.40Plastic Surgical Nursing the 100-ml drain, suction slowlydecreased as the reservoir wasfilled; however, the 400-ml reservoir maintained measurable suction until it contained an averageof 130 ml of saline.Using the bottom-pushed-intechnique on the 100-ml drainagesystem, no measurable negativepressures were recorded until thesuction jumped to an averageof 24.0 mmHg when the reservoir contained 70 ml of saline(Table 1b). From this point, suction maintained a relatively stable level until the drain reachedcapacity. In contrast, the 400-mldrainage system never reachedtrue measurable levels of negative pressure using the bottompushed-in technique at any pointwhile the reservoir was filled(Table 2b).DISCUSSIONBecause of the wide variety of surgical drainage systems currentlyavailable on the market, there islittle consensus among surgeonsas to which drains and whichtechniques for generating negative pressure are most effective(Swartz et al., 2012). However, onthe basis of our findings, we concluded that smaller drain reservoirs were able to generate moresuction than larger reservoirs andthat compressing the sides of thedrain bulb was the most effectivetechnique for evacuating the air togenerate negative pressure.In 2002, Grobmyer and colleagues published a study thatattempted to determine the suction gradients of three commonlyemployed surgical drains (Grobmyer, Graham, Brennan, & Coit,2002). Among the three types ofdrains analyzed was the 400-mlJackson-Pratt closed suction system that was also analyzed inour current study. In accordancewith our data, Coit determinedthat the maximum suction wasachieved when the reservoir wasempty and that negative pressureJanuary–March 2013 Volume 33 Number 1Copyright 2013 American Society of Plastic Surgical Nurses. Unauthorized reproduction of this article is prohibited.PSN200241.indd 4013/02/13 2:06 AM
when applying suction to thedrainage system.In 2009, Halfacree, Wilson, andBaines (2009) published the firststudy to address how user technique could affect the efficiency ofa surgical drainage system. In thisreport, the investigators comparedone-hand and two-hand compression methods for removing theair from the drain reservoir togenerate suction. Regardless ofthe size of the drain reservoir,it was determined that the twohand compression method causedsignificantly greater negative pressure than the one-hand method.However, the one-hand methoddid still generate a measurablelevel of suction. While our studyanalyzed two different techniquesfor generating suction, it was concluded that the bottom-pushed-intechnique did not generate anymeasurable level of suction whilethe side-to-side full-squeeze method demonstrated a much moreclinically useful range of negativepressures as the reservoir filled.Figure 5. Using a 400-ml Jackson-Pratt drainage system, average suction wasmeasured using either the full side-to-side squeeze or the bottom-pushed-intechnique of generating negative pressure. Measurements were repeated fivetimes and means were reported the standard deviation.with different reservoir volumes(Whitson, Richardson, Iaizzo, &Hess, 2009). They determinedthat, when empty, 100-ml reservoirs were able to achieve a higher level of suction than 400 mldrain reservoirs. As before, ourdata verified this conclusionwhen using the side-to-sidefull-squeeze technique for generating suction. Although bothof these studies did address thequestions surrounding the commercially available drain options,neither discussed the variationin negative pressure that couldbe caused by the technique useddecreased as the reservoir filled.While it was not clear what technique was used to eliminate theair from inside the reservoir togenerate the reported suction gradient, the authors were able toconclude that different types ofclosed suction surgical drainagesystems do achieve different levels of negative pressure.Whitson and colleagues (2009)further explored the topic of comparing different types of closedsuction drains. In this study,the investigators comparednot only drains from differentmanufacturers but also drainsTABLE 1. Negative Pressures of 100-ml Drainage SystemVolume of SalineAdded (ml)AB0102030405060708090100Average negativepressure (mmHg) 117.6 69.0 47.6 34.6 23.2 20.5Standard ge negativepressure (mmHg)ⱕ 20ⱕ 20ⱕ 20ⱕ 20ⱕ 20ⱕ 20ⱕ 20 24.0 28.3 25.7 26.0Standard deviation0.00.00.00.00.00.00.04.05.40.60.0Full squeezeⱕ 20.0 ⱕ 20.0 ⱕ 20.0 ⱕ 20.0 ⱕ 20.0Bottom pushed inTABLE 2. Negative Pressures of 400-ml Drainage SystemVolume of SalineAdded (ml)0102030405060708090100110120130A Full squeezeAverage negativepressure (mmHg)Standard deviation 71.4 58.4 48.8 41.6 36.0 26.6 26.8 26.0 24.6 22.4 21.8 21.0 20.5 ⱕ 20.08.88.26.55.64.213.52.91.62.12.31.71.41.30.0B Bottom pushed inAverage negativepressure (mmHg)Standard deviationPlastic Surgical Nursing ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 ⱕ 20 20.5 ⱕ 200.00.00.0January–March 20130.0 0.0Volume 33 0.00.00.00.00.00.00.00.7Number 10.041Copyright 2013 American Society of Plastic Surgical Nurses. Unauthorized reproduction of this article is prohibited.PSN200241.indd 4113/02/13 2:06 AM
Our study, in conjunction withthese previous reports, clearlyillustrates the massive variationin suction levels that can occurdepending on the size and typeof the drainage system, as well asthe method used to generate thenegative pressure. When the highest levels of suction are needed toprevent seroma development, asurgical drainage system with asmall reservoir should be chosenand the surgeon should compressthe reservoir in a side-to-side,two-handed manner to evacuate the air. In addition, since itwas observed that drain suctiondecreased as the volume of fluidin the reservoir increased, drainsshould be emptied as frequentlyas possible to maintain the highestpossible level of suction. At a minimum, since the drains used in thisstudy lost any measurable amountof suction when the reservoir wasapproximately half full, care providers must empty the drain reservoirs before they reach this point,so that they can continue to pullfluid from the wound bed. If highoutputs preclude timely emptyingof fluid from the drain reservoirs,larger collection devices, such asthe 400-ml container used in this42study, should be considered at thesmall expense of slightly lower suction pressures. Although researchis slowly filling in the gaps in ourknowledge about the dynamicsof surgical drain suction, furtherstudies are still needed. It wouldbe beneficial to address how, orto what degree, the length of thereservoir tubing effects the levelof suction in the wound bed andhow placement of multiple drainseffects the total negative pressuregenerated in the potential space.In summary, smaller drain reservoirs are more successful ingenerating a high initial suctionthan larger reservoirs, especiallywhen the volume of fluid in thedrain is relatively low. However,larger bulbs do tolerate highervolumes of fluid collection andallow for longer times to elapsebefore emptying. In all sizes ofdrains, compressing the sides ofthe reservoir is a far better technique for establishing negativepressure than pressing the bottomof the drain up toward the top.REFERENCESDurai, R., Mownah, A., & Ng, P. C.(2009). Use of drains in surgery:Plastic Surgical Nursing a review. Journal of PerioperativePractice, 19(6), 180–186.Grobmyer, S. R., Graham, D., Brennan,M. F., & Coit, D. (2002). Highpressure gradients generated byclosed-suction surgical drainagesystems. Surgery of Infectious, 3(3),245–249.Halfacree, Z. J., Wilson, A. M., &Baines, S. J. (2009). Evaluationof in vitro performance of suctiondrains. American Journal of Veterinary Research, 70(2), 283–289.Scevola, S., Youssef, A., Kroll, S. S.,& Langstein, H. (2002). Drainsand seromas in TRAM flap breastreconstruction. Annals of PlasticSurgery, 48(5), 511–514.Swartz, A. L., Azuh, O., Obeid, L. V.,Munaco, A. J., Toursavadkohi, S.,Adams, J., et al. (2012). Developingan experimental model for surgicaldrainage investigations: An initialreport. American Journal of Surgery,203(3), 388–391; discussion 391.Whitson, B. A., Richardson, E., Iaizzo,P. A., & Hess, D. J. (2009). Notevery bulb is a rose: A functionalcomparison of bulb suction devices. Journal of Surgical Research,156(2), 270–273.Zawaneh, P. N., & Putnam, D. (2008).Materials in surgery: A review ofbiomaterials in postsurgical tissueadhesion and seroma prevention.Tissue Engineering Part B Reviews,14(4), 377–391.January–March 2013 Volume 33 Number 1Copyright 2013 American Society of Plastic Surgical Nurses. Unauthorized reproduction of this article is prohibited.PSN200241.indd 4213/02/13 2:07 AM
Susan Lamp, BSN, RN, CPSN Ergun Kocak, MD, MS Katherine H. Carruthers, MS, is a medical student at the University of Toledo College of Medicine in Toledo, Ohio. She recently earned a master's degree in Biomedical Sciences at the University of Toledo College of Graduate Studies and is currently completing the first year of her medical education.