Transcription
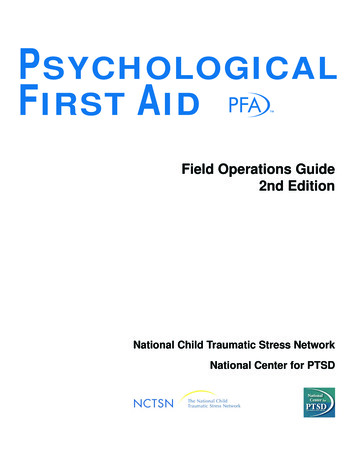
C L I N I CA L CA R EThe Pupillary Response inTraumatic Brain Injury:A Guide for Trauma NursesAndrea Adoni, BSN, RN, CCRN, CEN, EMTMolly McNett, PhD(c), MSN, RN ABSTRACTTraumatic brain injuries (TBIs) affect more than 1.4 million Americans annually. Trauma nurses caring for thesepatients routinely perform serial neurologic assessments,including pupillary examinations. While trauma nursesare likely familiar with basic components of the pupillary examination, some confusion about more specificaspects of the examination and the physiologic basis ofthe pupillary response may still remain, particularly as itpertains to patients with TBI. Therefore, the purpose ofthis article is to identify the key components of a pupillary examination and its associated physiologicresponse. A case study is provided to illustrate the application of this information among patients with TBI. KEY WORDSBrain injury, Pupil, TraumaTraumatic brain injury (TBI) affects more than 1.4 million Americans annually.1 These injuries, defined as ablow or penetrating injury to the head that disrupts normalbrain function,2 occur as a result of falls (28%), motorvehicle crashes (20%), being struck by or against a movingor stationary object (19%), and assaults (11%).3 Injuries tothe brain are classified as focal, such as cerebral contusions,lacerations, and hematomas/hemorrhages, or diffuse,which include concussions and diffuse axonal injuries.4Because the signs and symptoms of patients who have sustained TBIs may change quickly and evidence of deterioration may be subtle, trauma nurses must be adept atperforming astute neurologic assessments.A key component of any neurologic assessment is thepupillary examination.4 Trauma nurses at all levels ofcare routinely perform pupillary assessments on patientsand are likely to be familiar with the basic componentsof the pupillary examination. However, some confusionmay still remain about more specific aspects of the examination and the physiologic basis of the pupillaryresponse, particularly as it pertains to patients who havesustained TBIs. Therefore, the purpose of this article is toidentify the key components of the pupillary examination, explain the physiologic basis of the pupillaryresponse, and illustrate the application of this information in patients with TBI through a case study. CASE STUDYAndrea Adoni, BSN, RN, CCRN, CEN, EMT, is Flight NurseSpecialist, Cleveland Metro LifeFlight; MetroHealth MedicalCenter, and ACNP student, Frances Payne Bolton School ofNursing, Case Western Reserve University; and Molly McNett,MSN, RN, is Research Coordinator, Department of NursingResearch, MetroHealth Medical Center, Cleveland, Ohio.Corresponding Author: Andrea Adoni, BSN, RN, CCRN,CEN, EMT, Cleveland Metro Lifeflight Office, 4th FloorHamann, MetroHealth Medical Center, 2500 MetroHealth Dr,Cleveland, OH 44109 (aadoni@metrohealth.org).An 18-year-old woman was a restrained driver of a vehicle that was T-boned (lateral) at a high speed on the driver’s side of the car. The car subsequently rolled over ontoits roof. Emergency medical services arrived to find thevictim conscious but with a Glasgow Coma Scale (GCS)Score of 13 (Table 1). The victim’s pupils were noted tobe equal and reactive. The victim’s level of consciousnesscontinued to deteriorate while the emergency medicalservices worked to free her from the wreckage. Shearrived at the regional emergency department after40-minute extrication with a GCS Score of 8: she was givena 2 for opens eyes to painful stimuli, a 2 for unintelligibleverbal response, and a 4 for withdraws to pain. Herpupils were now unequal. The right pupil measured 5 mmand was nonreactive to a direct light, whereas her leftpupil measured 2 mm and displayed a sluggish reactionOctober–December 2007Journal of Trauma Nursing Volume 14, Number 4191
IDENTIFYING TBITABLE 1The GlasgowComa ScaleEye openingSpontaneous4Response to verbal command3Response to pain2No response1Best verbal responseOriented5Confused4Inappropriate words3Incomprehensible sounds2No verbal response1Best motor responseObeys commands6Locales to pain5Withdraws to pain4Flexion to pain3Extension to pain2No motor response1to direct light. She was noted to have a small foreheadlaceration with surrounding ecchymosis. She wassedated, paralyzed, and intubated by the emergencydepartment staff to ensure airway protection. A computerized tomography (CT) scan of the patient’s head wasperformed, which revealed a large subdural hematoma.The patient’s neurologic status continued to deteriorate,and, therefore, the local air medical service was immediately dispatched to transport the patient to a level Itrauma center. She was transported to a level I traumacenter for further evaluation of her head injury. Upon herarrival to the trauma center, her trauma evaluation wascompleted, and she was transferred to the surgical intensive care unit. Her pupils were found nonreactive on herinitial trauma evaluation at the trauma center. In the surgical intensive care unit, a neurosurgical consultation forthe treatment of an acute subdural hematoma and possible surgical evacuation was obtained.192Journal of Trauma Nursing Volume 14, Number 4Identifying an acute brain injury in patients with traumarequires serial neurologic examinations, including pupillary assessments, a CT scan, and possibly a magnetic resonance imaging. As depicted in the case study, evidence ofTBI may be present in the initial neurologic examinationperformed at the scene. Victims may have altered GCSscores or impaired level of consciousness ranging from subtle to severe. The initial pupillary examinations may appearbenign, and pupillary changes may not surface until hoursafter the occurrence of the injury. Performing serial neurologic examinations, including pupillary assessments, aids inidentifying subtle changes in a patient’s neurologic status.These subtle changes can indicate the presence of TBIand/or an acute deterioration in a patient’s condition.4 Thepresence of TBI is confirmed with a CT and/or a magneticresonance imaging once a patient arrives in a healthcarefacility. The CT scan can quickly aid in differentiatingbetween a focal and a diffuse brain injury.Subdural hematomas are one type of focal brain injuryoccurring in approximately 30% of patients with TBI.4 Anacute subdural hematoma occurs usually after a deceleration injury in which cerebral veins rupture because ofeither a linear or rotational shearing force.5 Rupture ofthese vessels causes bleeding into the subdural space. Thisbleeding may exert additional pressure onto the surrounding brain tissue, causing shifting of the tissue or masseffect. Because the subdural space is not limited by the cranial sutures, this bleeding can potentially spread along theentire cerebral hemisphere.6 As the size of the bleed andthe mass effect on the brain increases, the patient’s neurologic status declines, and pupillary changes often appear.As bleeding continues, the likelihood of a poor prognosisalso increases: mortality rates as high as 50% have beenreported among the patients who present with a subduralhematoma requiring immediate surgical evacuation.6 THE PUPILLARY EXAMINATIONThe standard of care for any patient with TBI includesserial neurologic examinations. These examinationsinclude a pupillary assessment and are often performedby trauma nurses at the scene, in the emergency department, and in the acute and critical care units.7 Unlikeother components of the neurologic examination thatrequire patients to be conscious, the pupillary examination is one of the few neurologic signs that can beassessed in an unconscious patient or in a patient receiving neuromuscular blocking agents and sedation. Thepupillary examination is a minimally invasive assessment,which provides valuable information about the severityand progression of the brain injury, as well as brainstemfunction. Thus, it is important for trauma nurses to perform pupillary examinations thoroughly and understandthe physiologic basis of the pupillary response.October–December 2007
When performing a pupillary examination in patientswith TBI, a trauma nurse should make the consciouspatient focus on a distant object straight ahead. In thecomatose patient, pupils are assessed per the positionthey are found in. A pupil assessment should include theexamination of size and equality of pupils, pupillaryshape, and reactivity to light.Pupil Size and EqualityPupil size is reported as the width or diameter of eachpupil in millimeters. A standardized pupil gauge shouldbe used to report the pupil size in millimeters. The use ofthis gauge aids in decreasing subjectivity, particularlywhen serial assessments are performed. The normaldiameter of the pupil is between 2 and 5 mm, with theaverage pupil measuring 3.5 mm. Although both pupilsshould be equal in size, a 1-mm discrepancy is considered a normal deviation. This condition is known asanisocoria and is present in 15% to 17% of the population without any known clinical significance.6 Pupil sizeshould be assessed both before and after the pupilresponds to direct light.Pupil ShapePupil shape is reported as round, irregular, or oval. Thenormal shape of the pupil is round. An irregular-shapedpupil may be the result of ophthalmological proceduressuch as cataract surgery or lens implants, and this shouldbe noted on the initial assessment and confirmed with thepatient or family. A pupil that is oval in shape may indicate the early compression of cranial nerve III due toincreased intracranial pressure (ICP), and thus should beaddressed immediately. If an oval pupil is detected, measures should be taken to decrease ICP. As ICP is reduced,the oval-shaped pupil should resolve. However, if ICPcontinues to rise or is not treated, the oval-shaped pupilwill become further dilated and will eventually becomenonreactive to light.Reactivity to LightA complete pupillary reactivity examination alsoincludes assessment of the consensual pupillary responseand accommodation. The consensual pupillary responseis the constriction that normally occurs in a pupil whenlight is shown into the opposite eye.6 Because of thisresponse, the trauma nurse should wait for several seconds before assessing pupillary light reflex in the secondeye, as that pupil may be temporarily constricted.Accommodation is the constriction of pupils that occurswhen a conscious patient is focusing on a close object.Pupils should normally constrict bilaterally when anobject is held within 4 to 6 inches of a patient’s nose.6 PHYSIOLOGICAL BASIS OF THEPUPILLARY RESPONSEThe pupil is a small hole in the center of the iris, whichallows light to enter in the lens of the eye. The diameter of the pupil is controlled by smooth muscle withinthe iris; and pupillary size, shape, and reactivity tolight are regulated by the autonomic nervous system.6The diameter of the iris is controlled by 2 muscles: thepupilloconstrictor, which is a sphincter muscle controlled by the parasympathetic nervous system; andthe pupillodilator, which has sympathetic nervous system control.8Parasympathetic Response: Pupillary ConstrictionNormally, when light is shone into the eye, the rods andcones of the retina serve as sensory receptors and send theimpulse via afferent nerve pathways through axons in theoptic nerve, optic chiasm, and optic tract.6 This impulsereaches the Edinger–Westphal nuclei in the midbrain. Theparasympathetic response originates in these nuclei, andefferent nerve pathways transmit the impulse via cranialnerve III to the pupilloconstrictor muscle.4 Both the ipsilateral and the contralateral Edinger–Westphal nucleireceive identical afferent input, which causes the consensual light reflex.8 The neurotransmitter responsible forthe synaptic response in pupillary constriction is acetylcholine.Pupil reactivity is reported as the response or reflex ofeach pupil to direct light. Reactivity is assessed byshining a low-beam flashlight inward from the outercanthus of each eye. Each eye should be checked separately. The light should not shine directly into thepupil because the glare or reflection may obscure visualization.6 The reaction that each pupil has to the lightstimulus should be recorded. The speed of pupillaryreactivity is recorded as brisk, sluggish, or nonreactive.Normally, pupils should constrict briskly in responseto light. A sluggish or slow pupillary response mayindicate increased ICP, and nonreactive pupils areoften associated with severe increases in ICP and/orsevere brain damage.The sympathetic pathway responsible for pupil dilationoriginates in the posterior-lateral hypothalamus andinvolves 3 neurons.4 The first ipsilateral preganglioniccentral neuron travels through the lateral brainstem tothe spinal cord. The second preganglionic neuron crossesthe lung apex and ascends the neck where it synapses inthe cervical ganglion. The third postganglionic neuronaccompanies the internal carotid into the skull base to thetrigeminal ganglion and joins the nerve fibers of theabducens as it passes through the inferior orbital fissure.This neuron then continues through the trigeminal nerveuntil it reaches the pupillodilator muscle in the iris. TheOctober–December 2007Journal of Trauma Nursing Volume 14, Number 4Sympathetic Response: Pupillary Dilation193
TABLE 2Abnormal Pupils Observed in Patients With TBIaPupillary AbnormalityUnequal pupilsPupillary Response/Assessment FindingsMydriasis: One pupil is dilatedand nonreactive to light. Otherpupil is of normal size andreacts to light.CausesDefect in efferent pathwayCompression of cranial nerve IIIUncal herniationCompression of posteriorcommunicating arteryDamage to nerve endings insphincter muscle of iris fromdirect traumaConstricted pupilsAdie’s pupil: One pupil is largerthan the other. The affected(larger) pupil does notimmediately respond to director consensual light reflex;however, if light stimulus isprolonged, this pupil willslowly constrict to light andslowly dilate in the dark.Accommodation in theaffected pupil is sluggish.The other pupil is of normalsize and reacts to light.Defect in efferent pathwayHorner’s syndrome: One pupil issmaller than the other. Theaffected (smaller) pupil has animpaired response to light andaccommodation. There isptosis of the eyelid on the sideof the affected pupil. There is aloss of sweating on theaffected side.Defect in efferent pathwayMiosis: Pupils are pinpointbilaterally and too small toobserve reaction to light.Loss of parasympathetic nervesupply to sphincter muscle iniris (frequently caused by viralinfection)Sensitivity to cholinergic drugsTotal or partial loss ofsympathetic innervation topupil (due to lesion insympathetic fibers inbrainstem or spinal cord)Damage to hypothalamusDefect in efferent pathwayDisruption in sympatheticpathway (can be due tointraocular inflammationfrom trauma/direct orbitalinjury)Irritation of parasympatheticpathwaysPontine hemorrhageDrug induced: opiates/narcotics,pilocarpine, acetylcholine(continues)194Journal of Trauma Nursing Volume 14, Number 4October–December 2007
TABLE 2(Continued)Abnormal Pupils Observed in Patients With TBIaPupillary AbnormalityDilated pupilsPupillary Response/Assessment FindingsCausesArgyll–Robertson: Pupils aresmall and irregular in shape,and may be unequal. Pupils donot respond to light stimulus,but do constrict withaccommodation. May dilateminimally in the dark.Defect in afferent pathwayDrug-induced mydriasis: Pupilsare dilated bilaterally. Pupilsmay or may not have reactionto light stimulus.Defect in efferent pathwayUsually due to viral infection(neurosyphilis, encephalitis)Sympathetic stimulants orparasympathetic blockingagents cause pupillary dilation.Caused by hallucinogens,antihistamines, amphetamines,anticholinergics, dopamine,and barbituratesMay be caused by ophthalmicmydriatics that are administeredfor intraocular examinations(atropine, scopolamine)Equal pupils with abnormalresponseAnoxia mydriasis: Pupils aredilated bilaterally and do notrespond to light stimulus.There is no consensualresponse or accommodation.Defect in efferent pathwayHippus: Pupils may be equal insize. Pupils initially react brisklyto light, but then alternatebetween dilation andconstriction.Defect in efferent pathwayMarcus Gunn pupil: Pupils areequal in size, but one pupilhas an abnormal response tolight. When direct light isshone into the affected eye,there is a sluggish reaction.When direct light is shoneinto the normal eye, theaffected eye will constrict(normal consensual reaction),but when the light is thendirected back to the affectedeye, the pupil in the affectedeye will dilate.Defect in afferent pathwayTranstentorial herniationAnoxiaBrain deathEarly compression of cranial nerve IIILesion/injury to midbrainBarbiturate toxicityLesion or atrophy of the retinaor optic nerve causes damageto afferent nerve fibersRetinal detachmentOcclusion in retinal vasculatureaFrom Hickey4 and Barker.6October–December 2007Journal of Trauma Nursing Volume 14, Number 4195
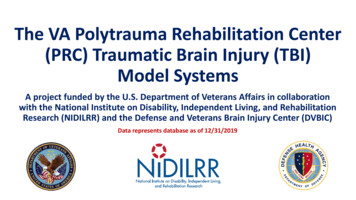
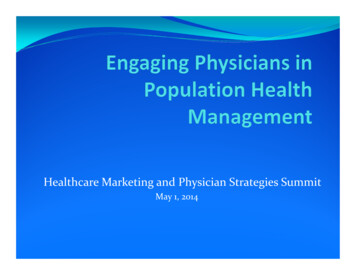
neurotransmitter responsible for this synaptic reaction isnorepinephrine.ICP monitoring will aid in definitively identifying thecause of the abnormal pupil.Cranial Nerves CONCLUSIONSThe eye is innervated by 3 cranial nerves (CN III, IV, VI),which work together to provide smooth eye movements.Cranial nerve III (oculomotor) controls the parasympathetic response of the pupil, causing pupillary constriction.6 Cranial nerves III, IV, and VI innervate the musclessurrounding the eye and are responsible for extraoculareye movements (EOMs). Assessment of EOM is appropriate in the conscious trauma patient and can be particularly important when caring for patients with facialtrauma. However, assessment of EOMs in the unconscious patient with TBI is not always possible or indicated. When caring for this type of patient, it is necessaryto assess only cranial nerve III by testing the pupillaryresponse to light. ABNORMAL PUPILLARY RESPONSEIN TBI PATIENTSWhen performing pupillary examinations in patients withTBI, trauma nurses may detect abnormalities, such as anirregular pupil size, shape, or a sluggish or nonreactivepupil. When an abnormality is detected, the trauma nurseshould first identify whether the abnormality was presenton the previous pupillary examination. If an abnormalpupil is present on the initial pupillary examination, itshould be clearly documented, and a physician should beimmediately notified. Immediate notification of a physician should occur with changes in pupillary response.Comparing the current examination with the previous toprovide time-oriented data for the physician is wise butshould never delay immediate physician notification.A complete neurologic examination should be performed and any changes in the patient’s condition shouldbe noted and reported to a physician. An abnormal pupilin a patient with TBI is often indicative of increasing ICPdue to progression of the hematoma/hemorrhage or cerebral edema. However, the trauma nurse should be awareof other clinical factors that may cause an abnormal pupilresponse. Table 2 highlights abnormal pupils that may beseen in TBI patients and identifies both physiologic andclinical factors contributing to the abnormalities.Regardless of the cause of an abnormal pupil, the traumanurse should always notify a physician immediately whenan abnormal pupil is detected. A CT scan and continuous196Journal of Trauma Nursing Volume 14, Number 4Interdisciplinary care for patients with TBI is oftenextremely complex, and trauma nurses have an integralrole in early detection and monitoring of changes inpatient status. The pupillary examination is a crucialcomponent of the serial neurologic assessments routinelyperformed by trauma nurses at all levels of care delivery.The pupillary examination can be quickly and easily performed in the unconscious or minimally responsivepatient when a TBI is suspected, and can provide valuableinformation about the degree of initial or progressingbrain injury. As evidenced in the case study, a specific typeof TBI, the subdural hematoma, may cause pupillarychanges, which indicate the need for rapid interventionsto decrease ICP and/or cerebral bleeding and edema. Bygaining a better understanding of the physiologic basis ofthe pupillary response and the particular components ofthe pupillary examination, trauma nurses are in a keyposition to detect early changes in a patient’s conditionand administer or advocate for immediate interventions.REFERENCES1. Centers for Disease Control and Prevention, Division of Injury andDisability Outcomes and Progress. Traumatic brain injury in theUnited States: emergency department visits, hospitalizations, anddeaths. www.cdc.gov/ncipc/pub-res/TBI in US 04/TBI-USA BookOct1.pdf. Accessed March 10, 2006.2. Centers for Disease Control and Prevention, National Center for InjuryPrevention and Control. Injury topics and fact sheets: traumatic braininjury. http://www.cdc.gov/ncipc/factsheets/tbi.htm. Accessed January5, 2007.3. Langlois J, Rutland-Brown W, Thomas K. Traumatic brain injury inthe United States: emergency department visits, hospitalizations, anddeaths. http://www.cdc.gov/ncipc/pubres/TBI in US 04/TBI%20in%20the%20US Jan 2006.pdf. Accessed January 5, 2007.4. Hickey J. The Clinical Practice of Neurological and NeurosurgicalNursing. 5th ed. Philadelphia: Lippincott Williams & Wilkins;2003:132–135, 170–176.5. Davis AE. Mechanisms of traumatic brain injury: biomechanical, structural and cellular considerations. Crit Care Nurs Q. 2000;23:1–13.6. Barker E. Neuroscience Nursing. St Louis, MO: Mosby;2001;45:60–78, 334–335.7. March K, Wellwood J, Lovasick D, Madden L, Criddle L, HenricksonS. Craniocerebral trauma. In: Bader M, Littlejohns L, eds. AANN CoreCurriculum for Neuroscience Nurses. 4th ed. St Louis, MO: Saunders;2004:277–334.8. Gilman S, Newman S. Manter and Gatz’s Essentials of ClinicalNeuroanatomy and Neurophysiology. Philadelphia: FA Davis; 2003.October–December 2007
services worked to free her from the wreckage. She arrived at the regional emergency department after 40-minute extrication with a GCS Score of 8: she was given a 2 for opens eyes to painful stimuli, a 2 for unintelligible verbal response, and a 4 for withdraws to pain. Her pupils were now unequal. The right pupil measured 5 mm