Transcription
THE HAWAII DIET:AD LIBITUM HIGH CARBOHYDRATE, LOW FAT MULTI-CULTURAL DIETFOR THE REDUCTION OF CHRONIC DISEASE RISK FACTORS:OBESITY, HYPERTENSION, HYPERCHOLESTEROLEMIA, AND HYPERGLYCEMIATerry T. Shintani MD, JD, MPH, SheHa Beckham RD, MPH, Amy C. Brown PhD, AD,and Helen KanawaUwali O’ConnorAbstractIntroductionObjective: The purpose of this study was to determine the healtheffects of a high carbohydrate. low fat multi-cultural traditional diet,The Hawaii Diet, fed ad libitum to an adult population.Methods: Twenty-two adults recruited from various cultural backgrounds in Hawaii were fed, without calorie or portion size restriction, the Hawaii Diet for 21 days. The Hawaii Diet, based on familiartraditional foods from different cultures, is high in complex carbohydrate(77% of calories). lowin fat(12% of calories), and moderate inprotein (11% of calories) Participants were encouraged to eat tosatiety.Results: There was a significant weight loss on The Hawaii Dietaveraging 10.8 lbs (23.8 kg) (P .0001). Blood pressure wasdecreased from an average of 136.0/82.7mm Hg to 125.5/78.9mmHg yielding a significant decrease of 10.4 mm Hg for systolic (P .01). Beginning diastolic levels were normal so decreases in thesevalues were not significant. Average lipid values also decreasedwith total serum cholesterol being significantly reduced from 205.3to 156.9 mg/dl (P .0001); LDL from 125.9 to 94,9 mg/dl (P .001);and HDL from 38.3 to 31.3 mg/dl (P .0005). Triglycerides (238.7to 152.2 mg/dl) and the Chol:HDL ratio (5.8 to 5.2) improved atmarginally significant levels (P .08). There was also a significantreduction in blood glucose levels from 112.2 to 91.5 mg/dL (P .01).Conclusion: The Hawaii Diet consisting of high carbohydrate, lowfat ethnic meals appears to have a beneficial influence on weightloss and in decreasing systolic blood pressure, total cholesterol,LDL, and blood glucose values. Marginal improvement occurred fortriglyceride levels. There was also a significant drop in HDL levels,however, the Chol:HDL was ratio did not increase. Purther studiesof longer duration with a control group should be conducted to testthe effectiveness of The Hawaii Diet in maintaining these healthbenefits over a longer period of time.People in Hawaii live longer than those residing in any other state inthe United States.2 A major factor may be the multi-ethnic traditional diets that were brought to Hawaii by the wide range of ethnicgroups that have become the basis of the multi-cultural populationof Hawaii. The popular use of foods from traditional diets of multiethnic, cultural origin occurs to a greater degree in Hawaii than inother regions of the United States.According to MacGregor, diet is by far the most importantenvironmental factor determining longevity.3 Traditional diets havehistorically been associated with low rates of chronic disease fromthe Pacific to the Mediterranean. Although there is a common use oftraditional Asian, Polynesian. and European foods in Hawaii, themodern American diet has rapidly become the dietary mainstay.Along with this change is the gradual increase in all the risk factorsof related to the health problems of Americans such as obesity,coronary heart disease, certain cancers, diabetes, and strokes.In order to evaluate the healthfulness of a modern mix of traditional ethnic foods in Hawaii, individuals of various ethnic backgrounds were placed on a diet composed of the multi-ethnic foodsof Hawaii. This diet, called The Hawaii Diet, is a part of a greaterprogram known as the Hawaii Health Initiative which is a wholeperson. whole-community intervention strategy to help improve thehealth of the people of Hawaii. This multi-cultural traditional diet(77% carbohydrates; 12 % fat; and II % protein) consists of modernversions of traditional dishes from many cultures.While there are a number of studies that have demonstrated the45healthfulness of traditional diets of the Mediterranean and Asia,there is some controversy as to whether high carbohydrate low fatdiets are beneficial, The concern stems from certain studies indicating that high carbohydrate diets may increase triglycerides andlower HDL levels/ Recent findings also suggest that high insulinlevels may he a risk factor for coronary heart disease, and that these7 This concern ismay increase due to high carbohydrate diets.Hawaiiwhereespecially relevant inthe traditional diets of theancestors of most people in Hawaii are typically high in carbohydrate.The purpose of this nutrition-based intervention study was todetermine ifad-lihiturn feeding of high carbohydrate, low fat multiethnic meals known as The Hawaii Diet, reduced certain chronicdisease risk factors, Measurable outcomes were determined byvsaluating .eight loss/gim blood pressuro lipid piofile (totalcholesterol, LDL. HDL, triglycerides, and cholesterol:HDL ratio),and blood glucose values.Correspondence to:Sheila Beckham, MPH. RDPreventive Health DepartmentWaianae Coast Comprehensive Health Center86-260 Farhngton HwyWaianae, HI 96792(ph) 808-696-1511 (tax) 808-696-1533sbeckham@wcchc.comHOWAN M6DOAL. JOURNAL., VOL (07 MAROH 200’.69
MethodsStudy Population: Twenty two participants were selected fromvarious sectors ot the community to include the Governor, cabinetmembers, one legislator. members of one of the Hawaiian homesteads. and various political, business, and community leaders. Allresided on the island ofOahu. with the exception of one subject fromthe Big Island. A screening interview was conducted of individualsfrom this pool of potential participants. They were selected from thispopulation on the fol lo i ng basis:H Commitment to the program and its rules so as to ensure thesuccess of the program.2) Stahilit\ of health problems so as nor to pose a danger to theindividuals h\ a complete change in diet.3) Potential for facilitating change in the community.4) Ethnic diversity.Ten men and I 3 women whose ages averaged 49.9 years (range33 to 89 years of age) were selected for the study. The averageweightof the participants was 237 lb (107.7 kg) with arange of 123.5to 471 lbs (107.8 to 102.9 kg). Of these participants; 13 were ofnative Hawaiian ancestry, 7 were of Asian ancestry. 2 were orEuropean ancestry, and I was of African ancestry. One subjectdropped out due to a conflict in scheduling making 22 the finalnumber of participants. Patients were screened to eliminate unstablehealth conditions such as congestive heart failure, renal insufficiency, unstable angina, and poorly controlled hypertension. Chronicmedical conditions of the subjects included: 6 hypertensives onmedication; 1 borderline hypertensive not on medication; 4 diabetics on medications with one of these taking insulin; 2 with glucoseintolerance; 2 on estrogen replacement therapy; and 1 with thyroidinsufficiency taking synthroid. None of the subjects were takingcholesterol lowering medication, but one was taking a fiber supplement. metamucil. The Diet and Study Design: The Hawaii Diet was designed todemonstrate the effectiveness of a multi-ethnic diet in controllingchronic disease risk tactors in a multi-ethnic population. The selection of food on the program consisted of foods from the variousethnic groups in Hawaii such as Japanese. Filipino. Portugcse.Italian. Hawaiian. Chinese. Thai. and others. In keeping with thepatterns of healthy diets of the Pacific (including Asia), the fatcontent was kept low (below I 2 r ( and the animal protein contentwas limited to approximately 8 ounces per week. The menu includedstaple foods such as brown rice. pasta. oatmeal, whole wheat bread.taro (a starch root). poi (mashed taro. sweet potato, and yams:assorted vegetables such as salad greens. squash. eggplant, tomato.hroccoli.Chinesegreens. and seaweed: fruit suchasapples.oranaes.pears. and papa\as. and protein sources such as legumes. tofu, fish.and skinless chicken.The study period was 21 days. Patients were informed of theprotocol. the risks and the benefits ot the program. and a consentform xs as signed. This informed consent form was approved by theInstitutional Rex icy Board of [niversity of Hawaii. The participants sei-e instructed to adhere strictly to the dietary regimen andwere not allowed to eat any food or drink any beverages other thanwhat was prescribed. All meals were prepared at a common meal sitein Honolulu that was conveniently accessed by the participants.Unlimited quantities of foods were made available except for fishand chicken. To approximate the multi—ethnic diets of the Pacific.estimated to contain approximatel I 2% fat. the menus were identical to a research project prex iouslv conducted in which the foodintake was measured carefully and the macronutrients calculatedprecisely.”The participants were required to come to the meal site twice a dafor breakfast and dinner. In the mornings, blood pressures weretaken and an indi iduals who had diabetes had their blood sugartested, LLinch and snacks ere distributed at this time. In the eveningcver\ one met for a health education session over dinner.The Hawaii Diet Program physician was present each day toevaluate and monitor medical conditions including blood pressures.blood sugars, medications and any other medical problems. Fastingblood panels including MDL and brief physical exams were done atthe beginning and at the end of the program. Blood samples wereanalyzed at the largest licensed commercial laboratory in Hawaii.Weights were taken each day at the meal site on the same balancescale. All official blood pressures were taken by a trained physicianor registered nurse. The statistical significance of the results of theprogram were analyzed using a paired, two-tailed “t” test with a 95%confidence interval forcomparing the difference between the means.ResultsWeight loss: The average weight loss on The Hawaii Diet Programwas 10.8 lbs (13.8kg) (range: 2.3 kgto l5kg)or6.4% of total weightwithin the three week period (Table I) (P .0001). BMI decreasedfrom 35.6 to 34.09 for a total decrease of(P .0001).Blood pressure: Systolic. but not diastolic blood pressure fellsignilicantly. The average systolic blood pressure decreased from136.0/82.7 mm Hg to 125.5/78.9 mm Hg yielding a significantdecrease of 10.4 mm Hg for systolic blood pressure (P .01).Serum Lipids: Average lipid values also decreased with total serumcholesterol being significantly reduced from 205.3 to 156.9 mg/dl (P .000 H: LDL from 125.9 to 94.9 mg/dl P .001) (n l9 becausethree of the participants had triglyceride levels that were too high touse tor LDL calculation): and MDL from 38.3 to 31.3 mg/dl (P .0005). Triglycerides (238.7 to 152.2 mg/dfl and the Chol:HDL ratio(5.8 to 5.2) were also reduced, but at levels that were marginallysignificant (P .0X.Serum Glucose: There was also a significant reduction in bloodglucose levels from 112.2 to 91.5 mg/dL (P .01). The signilicanceof the effect of the diet on serum glucose is difficult to assess becausefour of the suhects crc diabetics on medications and two additional subjects were glucose intolerant. All who were on medicationhad their dosages reduced. Of those who were not on medication, allexperienced a reduction in their fasting blood glucose measurements.DiscussionIn general. ecologic stLidies on the relationship between traditionaldiets and health indicate that there is an association between modernization of diet and the rising rates of obesity and other cardiovascular risk t iLtoisOhcsits is often associated ssith the cardioxasHA.WAO M6DCAL JOURNAL VOL. 60. MARCH 20070
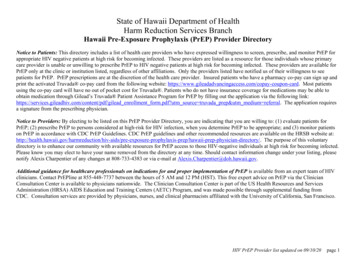
Table 1.—Average change in health risk factors for a multi-ethnicpopulation (n 22’) after 21 days on The Hawaii Diet.pHealth Risk 3102.9-10.8-4.9 .0001BMI(kg!m2)35.634.0-1.6 .0001Blood PressureSystolicDiastolic136.082.7125.578.910.43.8 .01 .07cholesterol (mg!dl)(mmobl)205.35,3156.94.1-48.5-1.25 .0001HDL(mg/dl)(mmol/l)38.31.0031.30.8-7.0-1.3 .001LDL(mg!dl)(mmol!l)125.93.394,92.5-310.8 chol!HDL ratio5.85.20.6 .5-1.0 001 .01n 19: 3 participants had triglyceride levels too high for LDL calculation.cular risk factors of hypertension, high total blood cholesterol, highLDL, low HDL. and higher fasting insulin levels.” Other majorconditions associated with obesity are some cancers. osteoarthritis,3 Obesity is a particularly problem for”2and gall bladder disease.’Hawaiians and Samoans,’7 however, unexplained differences in’4diet and physical activity, suggests that genetic factors play animportant role in the high prevalence of obesity in Native Hawai8 Nevertheless. multifactorial risk factor reduction is the mostians.’substantial benefit in decreasing cardiovascular morbidity and mor9tality.’Weight Loss: Studies have been conducted that show the value of20 Specifically, weight lossa low fat diet in producing weight loss.has been reported on ad libitum feeding of individuals with a low’ Our previous study utilizing the ad2energy density (LED) diet.lihitum feeding of very low fat (less than 10%), high carbohydrate(78%) pre-Western contact traditional diet yielded results that areconsistent with these studies,5 These studies suggest that a low fat,high carbohydrate, low energy density diet will produce steady andsafe weight loss sustained over a long period of time. Other researchstates that neither a low (35%) or high (45%) carbohydrate diet athypocaloric levels of 1200 Kcal/day had a greater advantage whenmeasuring weight 1055,22 On the otherhand, high energy density highfat foods have been suggested to facilitate the overconsumption of3fat.The multi-cultural Hawaii Diet in this study is both low in fatcontent (less than 12%) and low in energy density (0.80 cal/gm). Theaverage weight loss observed in this study (3.6 lbs/I .6kg per week)was somewhat greater than that found in other studies using LED24 and ad libitum low fat diets to reducediets (Weinsier 0.68 kg/wk)weight (Lissner 0.45 kg/wk)25 or other health risks (Buzzard, 0.2326kg/wk).These observations may he explained by the relatively high initialweight and BMI of the participants. The weight loss may also heexplained by the lower fat content of this diet (1 2%) compared to thatof other programs (15-23%). This hypothesis is based on studies thatsuggest that percent body fat retention is related to percent fat in the’ and that according to Pagliassotti et al. genetically obese27diet,29 Carmichaelprone rats do not become obese when fed low-fat diets.and associates also reported that a lower fat intake serves as apredictor of initial and sustained weight loss in obese subjectsconsuming an otherwise ad libitum diet. Another factor contribut3ing to the greater weight loss in this program may be the highcarbohydrate content in this diet that some studies suggest is directlyproportional to the amount of weight loss. This hypothesis is basedon the thermogenic effect of carbohydrate’ and on evidence that3shows that only a small percentage of carbohydrate is actuallyconverted to body fat.33’32These results and those of other recent studies, suggest thatvarying the mix of nutrients, in particular the amounts of fat andcarbohydrate, may be an effective way of dealing with obesitywithout requiring calorie counting. This is supported by Astrup et al.who reported that after a majorweight loss, an ad libitum low-fat dietprogram appears to be superior to caloric counting in maintainingweight loss two years later.34 It appears that ingesting LED dietscontributes to self-regulation of caloric intakes that decrease naturally as reported in previous studies with the traditional Hawaii dietwhich is naturally low in energy density.5 Supporting the importanceof energy intake is Ernst et al. who reported that, “A focus on fatintake alone without emphasis on energy balance is inadequate forachieving and maintaining recommended weight.”35Recently there has been some debate as to whether carbohydratescause a rise in insulin and therefore helps to reduce obesity. Thisstudy suggests that a traditional high carbohydrate diet based onwhole traditional foods that are low in energy density helps tocontrol blood sugar, insulin, and obesity.Hypertension: The significant decrease in systolic blood pressurein this study may have been related to the observed weight loss and/or decreased dietary sodium. Data involving 361 participants suggested that weight loss in the range of 4% to 8% of body weight wasassociated with a decrease in blood pressure in the range of 3 mm Hgsystolic and diastolic.3 The decrease in systolic, but not diastolicblood pressures observed in this study may have been influenced bythe blood pressure values prior to The Hawaii Diet. Five subjects hadhigh systolic blood pressure values compared to only one subjectwith high diastolic blood pressure before the study. and all 6 casesof hypertension normalized after being on the Hawaii diet for 3weeks.Serum Lipids: The decrease in serum cholesterol could he attrihuted to the low fat, low cholesterol content of the multi-ethnic foodsHAWA MEDCAt. JOURNAL, VOL 60. MARCH 200171
in the Hawaii DietInduced weight loss may also play a part inlowering cholesterol although even massive weight loss does notnecessarily induce a decrease in cholesterol.39 There was a moderatedecrease in LDL. and a slight significant decrease in HDL. Althoughthe decrease in HDL is not desirable, the decrease in total cholesterolyielded a net decrease in cardio ascular risk through the slightdecrease in Chol/lIDL ratio. The reduction in triglycerides is consisand inconsistent s ithtent ns ith high carbohydrate diet studiesothers that indicate that high a carhoh drate diet causes a rise intritzlvcerides.The triulvceridc le dc and Chol/HDL ratio mar—ci nall reduced on this high carboh drate diet (contrar to otherhigh carbohdrate studieri were possibl\ due to the use of morewhole cnu’hohvdrate foods such as whole grains and legumes insteadof refined carbohydrate ‘ourees such as sugar and white bread,The moderate reduction in serum lipids ith this diet occLirredover a relati ek short period. This suggests that a longer period onthis \ ei’ low fat diet could result in e en lower lipid levels and agreater decrease in cardiovascular risk than currently demonstrated.A recent diet study that yielded reduced cholesterol levels andradiographic evidence of reversal of atherosclerosis used a diet thatwas similarly very low in fat (I 09k) and suggests that The HawaiiDiet wotild have similar results.44paradoxical impact of this high carbohydrate, low fat diet ontriglycerides and glucose suggests that further study of this approachis warranted with an emphasis on the source of the carbohydratesand the overall energy density of the diet.AcknowledgementsThe authors would like to acknowledge the participants of the Hawaii HealthFoundation and the Waianae Coast Comprehensive Health Center who conductedthis study. We would also like to acknowledge the generous contributions of theQueen Emma Foundation, the Hawaii Medical Service Association. Aloha Care.and Aloha Airlines who made this project possible. In addition, we appreciate theassistance of Ke Ola Mamo. the Native Hawaiian health system for the island ofO’ahu for providing some of the staffing of the program and Alouettes Catering fopreparing the food. Finally, we want to acknowledge the support and participationof Honorable Benjamin Cayetano and his staff, the State of Hawaii. and thecommunity of PapakoIea for their cooperation in putting on this program.‘‘—.‘-Referencesat y State Stat Cu! Mefrop In r Co 1998 (3 99 3Kranczer S c no inBraun KL Y ng H On aA Honuch BY Life a d death ir H wan tt,ni van ti n in life expecta”n,anon 4 Cv 1080 nd 990 Ha MedJl 9655(122,8283 02OiacGr or GA Nutnti n nd b!009 pr su e Nutr Met b C rdiovasc Di 199 (4 Suppl) 6 16Srn ni U Hugh CK Tr di,iona! diet a the Pacific nd c n ‘y h art di a e CC rdiovasc Raet9941( (16- 0shin ni TT Hu h CK Be in m S OConno HK Ob ity and cardiov 5! r n k nt rv ntiorh ugh d (ibit m feeding ot traditional H w vs di t Am J Chn Cur 1991 53(16) 47S 51SRoche HM Diet ry carbohydr t and triacylg!ycero! metabob m p oc Nut Sod 999 58(1) 201 207La k o M lnsuhn Si t n e and c ton ry hear’ diaea e Curr Opin Llpido( 19967(4(21 226Shintani TT Becem n SK Bradley SH et aL The H w ii Diet Study (unpublished m nuac ipt--567PBlood Glucose: The decrease in fasting blood glucose was consistent with other programs using high complex carbohydrate. highfiber diets in the management of diahetes.’ The higher fibercontent of The Hawaii Diet, especially soluble fiber. may contributeto \\ hat Chandalia et al. observed as impro ing glvcemic control.decreasing hyperinsulinemia. and lowering plasma lipid concentrations m patients with Type II diahetes. The individual takingpsvllium supplements saw a reduction of blood sugar from 219 mgIdl to 120 mg/dl indicating that diet had a great impact overand abovehis baseline fiber supplement use.As stated above. interpretation of this data is difficult due to fourdiabetic subjects in the stud’ on medication, along with two subjectsdiagnosed with glucose intolerance. Because all 6 participants whohad high starting fasting serum glucose levels had significantlykm er blood sugar levels at the end of three weeks on the diet. ithan average reduction of 55 mgldl, it appears that the overall reduction in blood sugar would be even greater if this study wereconducted with participants who all had elevated beginning fastingblood sugar levels. In addition, because there is a close correlation49 it may he inferredbetween blood sugar levels and insulin levels,that insulin levels were also reduced by this diet, further decreasingcardiovascular risk.piog cc(Whittemor A Wu Wit: m AH cc M et a! Diet phwc ! activity nd co(orecta( cancer amoncChinese 9 North Amenc and Chin JNCI 1990 82 ft 915 926‘0 Yourg TK Sev nhuy en C Obsity a northern Canadian diana pattern d terminants. andconsequence Am C Chn Nutr 1989 49 786-79311 HarnsTB SavagePJ TeJIGS tal Carryinathebsrdenofcardiova cularriskinoldage associations9inc ght and se’ght o’-s’-o oth prevalent ardiovasculardisease ‘ac’ct—’s ond health status in theCard ovsocslar He’t’- o:.Oc Am J Cm Nutr 1997 66:4! 837-844Exp Can Enoocrr C’abetes t 998:106 Ssppi9be Leiva A Wnst sre:”e :refiy 4 moderate weight ioss210-13000dmanMT Hsnk’nJH WikensLR eta! dietbortysize ohysicalactini, sndtheriskoferdometriacancer Cancer Rca 10-97 7221 5077 50851Hughes CK Tsarin JA Mokuaj NK Dat-related cancer in Native Hawavsns Cancer 1906 78i7Ssppl: 1558-t56aMsu MK G’andinetti A A’seski RF et ai The niss!in resistance ayndrom n native Hawatiass Nstiue7C ‘3803Hawaiian HeaithNHHP1 Protect Diabetes Care 1997 20(9 ‘P Wasnich R Adipoaty and blood pre sa eNonotnu R D vi J“cltietnsic population a’‘-‘a t 1998 33: 167-LWo one’ in Hawarof12131415‘o“-:7 Pan’oorlG JaneG Bosic.’alriskoinlongevity SsmoanoinCsirorni- ncScrMedt982 162. 18319018 Grondinetti A C8 ng HK C en Petal Prevalence of overweight and centr diposity is asSociatesart oe.centag of indig nou ancestr among native Hscsnsn In J Obe Re! I Metab Diaord1499 2317: 31 Zaf a i Am Weng NK S cond ry preve9t on of “o’ons”y heart d e e Arch Phya med Reha bil199879)8 0061017H ‘(JO 61 ! n n EL Wyatt HT Di t ‘y t t ntske aid uat on of n rgv b (anc in a tans ‘ay C Cu 2 0 I 012 uppll 284 288S1I rRL U ft ct othigf’ ndloo n gvd n itydi 1 0iety n .gynKH Ba onJA WAn J rtn Nufr ‘98 3776 767on b e ssb(d i irrn of “b.9 In J Obo RyeGo! y Ana yr C 6” i YW ight is at (a r big c r a ydr10 7 1 7‘a D d20rIt’ a ‘rcsn rr cigvo na JNut’2 0 13012SRp 2sBS-DtI2-,a—tS“IConclusionThe high carbohydrate. low fat, loss energx density, multi—ethnicHiss ai Diet administered ad li/ritiwi ss as demonstrated to induce asieniticant weight loss and areduction in sv stolic hypertension, totalcholesterol. LDL. and serum glucose. Triglycerides and Chol: HDLratio were marginally reduced.Because these i nprovements in health risk factors ss crc obtainedvs ithout calorie ic striction or portion—si/c limitations iwith theexception ol animal protein i. this has important implications iiilone—term adherence to such a diet. Further research is needed toirtse’ss the lone term effectiveness of such ii proeram. In addition, the2B‘—K ‘I ,-3‘-V61,.‘E“—“.‘d’guII f’ p9505 1co1 ’——,‘‘—‘oe’,‘‘-si‘o3o-oAatv .‘-.3‘.lP L9,—,.,,4.“ 4”—, C‘--‘‘f—“-“‘‘,,‘-re—-—. �� ‘a’- a19I J0‘.-‘‘‘—‘-“‘0fIa’ alot 3 laca“-s’I I ova I I“iHJ e’o Ds—5,5—ai‘-,‘‘a’LL t”——5-’-RId“C, ‘—-“-.‘.a‘-0’-
“DNR Orders.” refJrence,s’ continued from p. 6733. Acheson KJ. Schutz Y. Bessard T, et aL Nutritional influences on lipogenesis and thermogenesis aftera carbohydrate meaL Am J Ptrysiol 1984:246(1 Pt 1 ):E62-70.34. Aatrup A. Toubro S. Raben A. Skov AR. The role of low-tat diets and tat substitutes in body weightmanagement: what have we learned from clinical studies? JAm Diet Assoc 1997:97(7 Suppl(:S82-87.35. Ernat ND, Obarzanek E, Clark MB. El al. Cardiovascular health risks related to overweight. JAm DietAssoc 1997:97(7 Supppl(:547-51.36. Murlow CD. Chiquette E. Angel L. Et al, Dieting to reduce body weight for controlling hypertension inadults. Cochrane Database Syst Rev 2000:2:CD000484.37. Chima CS. Miller-Kovach K. et al. Lipid management clinic: Dietary intemention for patients withhypercholeaterolemia. JAm Diet Assoc 1990:90:272-274.38. Connor WE. Connor SL. The dietary treatment of hyperlipidemia: rationale, technique, and efficacy.Med Clin North Am 1982:66:485-518.39. Kempner W. Newborg BD. Peachel RL, & Skyler JS. Treatment of massive obesity with rice/reductiondiet program. Arch mr Med 1975:35:1575-1584.40. Snehalatha C. Sivasankari S. Satyavani K. et al, Postprandial hypertriglyceridaemia in treated type 2diabetic subiects —the role of dietary components. Draberes Rca ON Pract2ODO:48(1 (:57-60.41. Turley ML, Skeaff CM. Mann JI. Con B. The effect of a iom-fat, high-carbohydrate diet on serum highdensity lipoprotein cholesterol and triglyceride. EurJ Clin Nutr 1998:52(10(:728-732.42. Blades B, Garg A. Mechanisms of increase in plasma triacylglycerol concentrations as a result of highcarbohydrate intakes in patients with non-insulin-dependent diabetes mellitus, Am J Clin Nutrt995:62(5(:996-t002.43. Garg A. Bantle JP, Henry RR, Coulston AM. Effects of varying carbohydrate content of diet in patientswith non-insulin-dependent diabetes mellitus, JAMA 1994:1 i18(:1 421-1428.44, Drnish D. Brown SE, Scherwitz LW. etal, Can lifestyle changes reverse coronary heartdisease? Lancet1990:336:129-133,45. Anderson JW. Hypolipidemic effects of high carbohydrate high fiber diets, Metabolism 1980:29:551558.46. Andersen B. P Hellstrom, et al. Effects of a rice rich versus a potato rich diet on glucose, lipoprotein,and cholesterol metabolism in noninsulin dependent diabetics, Am J Clin Nutr 1984: 39:598-606.47. Chandalia M, Garg A, Lutjohann D, et al. Beneficial effects of high dietary fiber intake in patients withtype 2 diabetes mellitus. N Engi J Med 2000:342(1 9(:1 392-1398.48. Morris KL. Zemel MB. Glycemic indes, cardiovascular disease, and obesity. Nutr Rev 1999:57(9 Pt1(:273’276.32. American Society of Anesthesiology. Ethical Guidelines for the Anesthesia Care of Patients with DoNot-Resuscitate Drders or Dther Directives that Limit Treatment; amended 1998.33. Statement of the American College of Surgeons on Advance Directives of Patients, “Do not resuscitate”in the operating room, ACLS Bulletin, 1994.34. Statement of the American College ot Surgeons on Advance Directives of Patients. “Do not resuscitate”in the operating room, ACLS Bulletin, 1994.35. Statement of the American College ot Surgeons on Advance Directives of Patients, “Do nor resuscitate”in the operating room, ACLS Bulletin, 1994.36. Amellcan Society of Anesthesiology. Ethical Guidellnes for the Anesthesia Care of Patients wrth DoNot-Resusc,tate Drders or Dther Directives that Limit Treatment; amended 1998.1. Hjt by a golf ball.F I V E WAYSTO D I E 0 N T H EGOLF2. Run over by a golf cart3. Whacked by a golf club.4. Struck by lightning.5. Forgot your hatSurprisingly, one million new cases of skin cancer are detected every year. One person an hour in the U.S. diesfrom melanoma, the deadliest form of skin cancer. If you spend a lot of time in the sun, you should protect yourself.One out of five Americans develops skin cancer during their lifetime. Don’t be one of them. Stay out of the middaysun. Cover up. Wear a hat, Seek shade. And use sunscreen. For more information on how to protect yourself fromskin cancer, call l-888—462-DERM or visit www.aad.org.are4 - ‘4U’U”AMERICAN ACADEMY OF DERMATOLOGYviAi,R’n.ii MEDICAL JOURNAL, VOL 60, MORON 200173
tion, the Hawaii Diet for 21 days. The Hawaii Diet, based on familiar traditional foods from different cultures, is high in complex carbohy drate(77% ofcalories). lowin fat(12% ofcalories), andmoderate in protein (11% of calories) Participants were encouraged to eat to satiety. Results: There was a significant weight loss on The Hawaii Diet