Transcription
Roheger et al. Diagnostic and Prognostic 2020) 4:7Diagnostic andPrognostic ResearchREVIEWOpen AccessPrognostic factors for change in memorytest performance after memory training inhealthy older adults: a systematic reviewand outline of statistical challengesMandy Roheger1* , Ann-Kristin Folkerts1, Fabian Krohm1, Nicole Skoetz2 and Elke Kalbe1AbstractBackground: The goal is to investigate prognostic factors for change in memory test performance in healthy olderadults and to report and discuss the different statistical procedures used for investigating this topic in the literature.Methods: Prognostic factors were here understood as any measures that were investigated to estimate change inmemory test performance. MEDLINE, Web of Science Core Collection, CENTRAL, and PsycInfo were searched up toNovember 2019. Prognostic factor and prognostic factor finding studies investigating prognostic factors on verbaland non-verbal short- and long-term memory after conducting memory training in healthy older adults wereincluded. Risk of bias was assessed using the QUIPS tool.Results: Our search yielded 12,974 results. We included 29 studies that address prognostic factors of changein memory test performance, including sociodemographic, (neuro-)psychological, genetic, and biologicalparameters. Studies showed high variation and methodological shortcomings with regard to the assessment,statistical evaluation, and reporting of the investigated prognostic factors. Included studies used differenttypes of dependent variables (change scores vs. post-test scores) when defining change in memory testperformance leading to contradictory results. Age was the only variable investigated throughout most of thestudies, showing that older adults benefit more from training when using the change score as the dependentvariable.Conclusion: Overall, there is a need for adequate reporting in studies of prognostic factors for change inmemory test performance. Because of inconsistencies and methodological shortcomings in the literature,conclusions regarding prognostic factors remain uncertain. As a tentative conclusion, one may say that thehigher the age of the participant, the more profound the improvement in memory test performance will beafter memory training.Trial registration: CRD42019127479.Keywords: Prognostic factors, Memory training, Prediction, Verbal memory* Correspondence: mandy.roheger@uk-koeln.de1Department of Medical Psychology Neuropsychology and Gender Studies& Center for Neuropsychological Diagnostics and Intervention (CeNDI),Faculty of Medicine and University Hospital Cologne, University of Cologne,Kerpener Str. 68, 50937 Cologne, GermanyFull list of author information is available at the end of the article The Author(s). 2020 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication o/1.0/) applies to the data made available in this article, unless otherwise stated.
Roheger et al. Diagnostic and Prognostic Research(2020) 4:7BackgroundEven in the absence of severe health issues, the agingprocess is associated with a decline in cognitive functioning, e.g., in memory, attention, or executive functions, which may result in a loss of autonomy andquality of life in older individuals [1]. One way thathas been discussed to be able to contribute to maintenance of cognitive function in the older age ( 55years) is cognitive training (CT, defined as guidedcognitive exercises designed to improve specific cognitive functions, as well as enhance performance inuntrained cognitive tasks [2]). Recent meta-analysesand reviews show that CT can be effective not onlyin improving cognitive functions in healthy older individuals, but also their quality of life [3, 4]. There aremany different types of CT, which differ regardingtheir settings (e.g., single vs. group settings), materialsused (e.g., computerized vs. paper-and-pencil tasks),but also regarding their focus on different outcomes(e.g., memory, attention, executive functions). Memory, which is a key function that typically decreasesin higher age, even in healthy older adults [5], canalso be improved or maintained with the help of CT[4]. However, one question that remains underinvestigated is: who (with which profile of, e.g., sociodemographic, neuropsychological, genetic parameters)benefits from CT? Yet, identifying prognostic factorsis highly important for providing new treatmentoptions and in term of dementia prevention [6].Prognostic factors (in literature also often referred toas “predictors”) for changes in test performance aftera CT that are under debate are sociodemographicvariables, brain imaging parameters, genetic parameters, and blood factors, as well as personality traits,cognitive and non-cognitive abilities at the entry ofthe training, and different training characteristics, e.g.,intensity of the trainings [7]. Yet, data is highly inconsistent: for example, there are several studies thatreport higher age as a positive prognostic factor forchanges in test performance after a CT in healthyolder adults [7, 8], while some studies indicate thatyounger individuals show improvement in test performance after a CT [9, 10].Yet, inconsistent results regarding prognostic factors ofCT can be seen throughout the prognostic factor literature for CT benefits so far, and the question arises, whythis is the case. Until now, no systematic review exists investigating prognostic factors for CT success in healthyolder adults in general, and memory training in particularto answer this question [11]. However, considering thefact that prognostic factors for change in cognitive performances after a CT in healthy older adults have many potential uses (e.g., aiding treatment and lifestyle decisions,improving individual dementia risk prediction, providingPage 2 of 23new treatment options [6]), and data so far revealshighly inconsistent results, systematic reviews andmeta-analyses are urgently needed to summarize evidence about the prognostic value of particular factorsto help to match cognitive interventions to individualsto improve their effectiveness in regard of a personalized medicine approach [12, 13].Therefore, the present review focuses on prognosticfactors for changes in memory performances after memory training, due to different reasons: first, memory belongs to the most vulnerable cognitive functions in aging(e.g., [5]). Second, we wanted to get a first overview overthe published data on prognostic research after traininginterventions in a narrower frame, therefore focusingonly on one specific relevant domain. Conclusions fromthis review could then help further research on prognostic factors of cognitive change induced by CTs.ObjectivesThe main goal of the present systematic review is to investigate prognostic factors for changes in memory performance after memory training in healthy older adults.Further, we wanted to investigate different methods usedto evaluate prognostic factors for changes in memoryperformance after memory training. Based on the checklist for critical appraisal and data extraction for systematic reviews of prediction modelling studies [12, 14, 15],which can also be used to assess prognostic factors studies [12], we defined our systematic review question usingthe “PICOTS system” [15]. Our target population arehealthy older individuals, defined as individuals aged 55 years with absence of any neurological or psychiatricdisease (P). Regarding the investigated intervention (I),we investigated all prognostic factors assessed for changein memory test performance after memory training. Nocomparator factor is being considered (C). Outcomeevents for this review are changes in memory test performance after memory training in the domains verbalshort-term memory, verbal long-term memory, as wellas non-verbal short- and long-term memory operationalized with objective and standardized measurement instruments (O). The measurement of the prognosticfactor had to be done before the memory trainingstarted and all follow-up information on the outcomes(all time periods) was extracted from the studies (T). Finally, prognostic factor measurement was studied innon-clinical settings to provide prognostic informationfor possibilities of prevention of cognitive decline (inother words, possibilities to strengthen cognitive function) in cognitively intact individuals (S).MethodsThe present systematic review was preregistered; the review protocol can be assessed at www.crd.york.ac.uk/
Roheger et al. Diagnostic and Prognostic Research(2020) 4:7PROSPERO/ (ID: CRD42019127479). The reportingfollows the Preferred Reporting Items for SystematicReviews and Meta-Analyses (PRISMA) guideline for systematic reviews and meta-analysis [16]. “The PRISMAfor Abstracts Checklists”, as well as “The PRISMAchecklist for systematic reviews” are displayed inSupplementary Tables 1 and 2.Search and study selectionA systematic search was conducted in MEDLINE Ovid,Web of Science Core Collection, CENTRAL, and PsycInfoup to October 2018. An update-search was conducted inthe same data bases until 12th November 2019. Referencelists of all identified trials, relevant review articles, andcurrent treatment guidelines were hand searched for further literature. In cases where no full text could be obtained, we contacted the authors and asked them toprovide full text publications within a 2-week time frame.Further information on the systematic search and the fullsearch strings for each database are presented in theSupplementary Material, Tables 3, 4, 5 and 6.Titles and abstracts were screened according to predefined eligibility criteria by two individual review authors(MR and AKF) with the Covidence Software (VeritasHealth Innovation) [17]. Afterwards, the full-text articlesof the studies meeting the inclusion criteria were furtherreviewed for inclusion in the systematic review. In caseswhere no consensus could be reached between the twoauthors MR and AKF, a third author (NS) was askedand the case was discussed until a final consensus wasreached.Page 3 of 23investigate changes in memory test performance aftermemory training were included in the review and metaanalysis. Memory training was defined as a CT that targets primarily on memory performance with a minimumof two sessions in total. The memory training can eitherinclude computerized or paper-pencil tasks with clearcognitive rationale, which are administered either onpersonal devices or in individual- or group settings heldby a facilitator. When multi-domain approaches wereexamined, memory had to be the main component ofthe program (at least 50% of the exercises).Prognostic factor studies, which investigate memorytraining benefits as an outcome (verbal or non-verbalshort- or long-term memory) measured with establishedobjective neuropsychological tests, were included. Working memory was excluded and is being investigated in adifferent review, as we define working memory as an executive function rather than a pure memory function[18]. We excluded subjective self-rated memory scales,as well as measures of memory strategy use. The factormeasurement of the included studies had to be conducted before the memory training started, and therewas no limitation regarding the length of the follow-ups.Data extractionTwo review authors (MR and AKF) independently extracted the data according to the Critical appraisal anddata extraction for systematic reviews of predictionmodelling studies prognostic factors (CHARMS PF)checklist [15] to investigate the reporting of prognosticfactors.Eligibility criteriaQuality assessmentThe review focused on peer-reviewed studies in Englishand German with no limitations regarding publicationdate which investigated prognostic factors of changes inmemory test performance after memory training. Fullstudy reports needed to be available; abstracts, books,book chapters, study protocols, and conference paperswere excluded.Prognostic factor studies on healthy older participants(age 55 years) were included. Data from participantswith dementia diagnosis, neurological and/or psychiatricdiseases, as well as uncorrected seeing or hearing impairments, assessed at least via self-report, were excluded.Studies with participants with mild cognitive impairment(if reported) were also excluded as we want to investigate healthy adults in the context of interventions.Regarding the investigated intervention and includedprognostic factors, all prognostic factors (e.g., sociodemographic factors, brain imaging parameters, genetic parameters, blood factors, personality traits, cognitiveabilities at the entry of the training, different trainingcharacteristics, e.g., intensity of the trainings, etc.) whichTwo reviewers (MR and AKF) independently assessed theextracted studies for the risk of bias using the Quality inPrognosis Studies (QUIPS) checklist, developed by Haydenet al. [19] to examine the risk of bias in prognostic factorsstudies across six domains [19]: Study participation,study attrition, prognostic factor measurement, outcome measurement, adjustment for other prognosticfactors, statistical analyses, and reporting. Each of thesix domains was judged with high, moderate or lowrisk. A detailed description of the domains includedin the tool and the judgment taken by the two reviewers is presented in Supplementary Material 7.Statistical analysesIn the pre-registration of the study, we registered ameta-analysis to investigate the predictive performanceof the different prognostic factors. The goal was tometa-analyze groups of “similar” prognostic effect measures with a random effects approach to allow for unexplained heterogeneity across studies. However, after thedata extraction, we found that data on prognostic factors
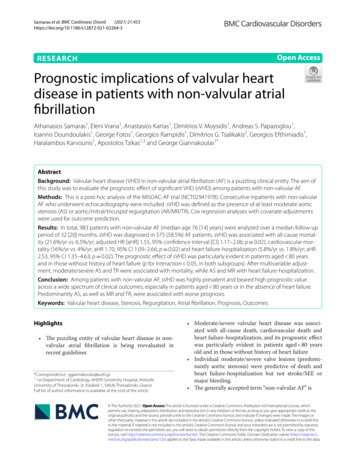
Roheger et al. Diagnostic and Prognostic Research(2020) 4:7Page 4 of 23Fig. 1 PRISMA diagram of the study selection processof changes in memory test performance after memorytraining were too heterogeneous and too poorly reportedto conduct a meta-analysis.ResultsStudy selectionThe total number of retrieved references and the numbers of included and excluded studies with reasons forexclusions are documented in a flow chart as recommended in the PRISMA statement [16]. The PRISMAdiagram in Fig. 1 illustrates the study selection process.Further, 10,703 studies were identified through the database search and by scanning the included studies in previously published systematic reviews and meta-analysison memory training success in healthy older adults, n 2271 studies were identified in an update search. Afterremoving the duplicates, n 9979 studies were screened.It was difficult to distinguish, from study abstracts alone,between prognostic factor finding studies and model development studies. We thus assessed 845 full-texts foreligibility. Finally, n 29 studies were included in thepresent review. All studies were published in English.Data extractionA main challenge was to distinguish between prognostic factor finding and model development studies,as the authors in general did not state their aim regarding prognostic factors or models. Therefore, weused full text interpretations to classify studies asprognostic factor finding or model development studies. Eight discrepancies were resolved after discussionwith a third reviewer (NK) with experience in thefield of prognostic research.Study characteristicsAn overview of the main characteristics of the included studies is outlined in Table 1. Further information of the included studies is illustrated inSupplementary Tables 8 and 9.Of the 29 studies included, we found that 15 studiesused a randomized controlled design, whereas six studiesonly used a controlled design (Table 1). Furthermore,eight studies used a non-randomized, non-controlledlongitudinal study design, which may be classified as acohort study, as the defining characteristic of the cohort
871.9 (66–81)74.77(6.57)60–70yearsKirchhoff et al. [23]Controlled trialn 16n n.a.Leahy et al. [24, 25]RCTn 22n 1Andrewes et al. [26]RCT controlled for sexn 20n 310810137Kirchhoff et al. [22]72.00 (66– 7Non-randomized, non81)controlled longitudinal studyn 16n 2 due to technicaldifficulties85315Mohs et al. [21]RCTn 68n n.a.78.30(7.40)78 O'Hara et al. [9]73.73(7.62) 34Non-randomized, noncontrolled longitudinal studyn 531n 419 due to severalreasons at 5-year follow-upPesce et al. [20]Stratified randomized studyn 30n 29 Sex1570.40(7.00)Study designInitial sample size for theexperimental groupDropout and reasons14SampleAge(years, M,SD)StudySome secondaryschooling: n 3Secondaryschool tradequalifications: n 5Completesecondaryschool: n 618.77 (2.62)14.8 (2.7)14.70 (2.90)16.00 (2.70)15.56 (2.79)9.60 (1.80)Education(years,M, SD)Memory handbook training forface-name and prospectivememory areas; independentlyimplemented at home4 weeks, 30 min per sessionVerbal memory assessed withCVLT, non-verbal memoryassessed with BFLT.Assessed 2 times at baseline,at post-test, 3 months and6 months follow-upNumber of words correctlyrecalled, number of wordscorrectly recalled in order.Assessed at baseline and 5-yearfollow-up measurementMissingImprovement in: Face-name Test,information Laboratory Prospective MemoryAssessment, Everyday ProspectiveMemory Assessment.Assessed at pre-test, post-testand 4-month FUAutobiographical memory specificity.Assessed at pre-test, post-test, and 3months follow-up.MissingRecognition memory usinginformation Remember/Know/New recognitionmemory decisions.Assessed at pre-training and posttrainingMissingMemory retrieval using Remember/information Know/New recognition memorydecisionsAssessed at pre-training and posttraining8101200RAVLT, MMSE2880OutcomesDefinition and method ofassessmentTiming of outcomeassessmentTotallength oftraining inminutesMemory specificity training to240improve the specificity of olderadults’ retrieval of autobiographicalmemories by providing systematicpractice.4 weeks, once a week for 60 minMemory strategy training andpractice2 training sessions.Memory strategy training andpractice.2 training sessionsStructured memory trainingfocusing on memoryimprovement and differentstrategies.Nine 90-min sessionsMethod of loci.2 weeks, 5 times a week for 2 hMethod of loci and generalstrategies.24 weeks, 2 times a weekfor 1 hDescription of memorytraining—content andfrequencyTrainingTable 1 Study and participant characteristics of the included studiesPrognostic factorsRAVLT, Warrington Forced-ChoiceRecognition for Faces, BDI, NART,Mattis Dementia Rating Scale.Memory specificity assessed withMEPS, functional limitationsassessed with FLP, self-rateddepression assessed with HADS,independence assessed with IADLActivity in prefrontal cortex, leftlateral temporal cortex.Hippocampal activityAge, education, gender, subjectivereported memory assessed withthe MFI and the MFQPre-training, gain scores followingtraining, age, education, reporteduse of mnemonic at follow-up,type of pre-training (standard vs.comprehensive) and length oftraining.Antioxidant levels assessedwith the Biological Antioxidantpotential Test; reactive oxygenmetabolites derivative compoundsassessed with the d-ROMs TestDefinition and methodsRoheger et al. Diagnostic and Prognostic Research(2020) 4:7Page 5 of 23
Memory training focused onimproving verbal episodicmemory through instructionand practice in strategy use6 weeks, 10 60-min sessionsNo demographics separately for thememory training groups were reported.73.60(3.00)Clark et al. [31]Multi-site RCT (ACTIVE)n n.a.n n.a.de Lange et al., [32]Controlled trialn 76n 9 due to timeconstraints2551Memory training focusedon improving verbal episodicmemory through instructionand practice in strategy use6 weeks, 10 60-min sessionsNo demographics separately for thememory training groups were reported.15.00 (2.70)Learning and practicing theMethod of Loci techniqueaiming to improve episodicmemory performance.10 weeks, once a week 8 weekly online homeassignmentsPre-training: imagery training,verbal elaboration andrelaxation.Name-Face Mnemonic:three-step mnemonicMethod of loci: method ofloci for serial word recall.2 weeks, 5 times a week for120 min)Clark et al. [30]Multi-site RCT (ACTIVE)n n.a.n n.a.15.33 (2.58)n.a.n.a.68.58(7.05)Learning and practicing theMethod of loci techniqueaiming to improve episodicmemory performance10 weeks, once a week 8 weekly online homeassignmentsModified recollection trainingprocedure2 weeks, 4 sessions per dayat 7 daysBrooks et al. [8]RCTn 224Dropout not reportedOld: 14.70 (2.90)18.00 (3.30)Method of lociNo information on trainingduration and frequencyOld:49n.a.10.70 (n.a.)TrainingOld: 73.40 Old:(3.00)29n.a.Bissig and Lustig [28]74.50Non-randomized, non(6.10)controlled longitudinal studyn 19n 1 due to low accuracyof studied words7Began tertiaryschool: n 6Bråthen et al. [29]Controlled trialn 126n 32SampleAnschutz et al. [27]73.50Non-randomized, non(n.a.)controlled longitudinal studyn 10n 1 due to severe illnessStudyTable 1 Study and participant characteristics of the included studies (Continued)Hopkins Verbal Learning Test,RAVL, RBMT.Measured at baseline, immediatepost-training, 1-;2-, 3-; 5-, and10-year FUHVLT, RAVL, RBMT.Measured at baseline, immediatepost-training, 1-;2-, 3-; 5-, and10-year FUProper name recall task, wordrecall task (16 common words).Assessed at pre-test andpost-testMissingMemory improvement: Wordinformation list recall6006001200MissingMemory improvement: changeinformation in correct written recall of wordlist consisting of 100 nouns.Assessed at pre-test andpost-testMissingRanking: participants wereinformation ranked by final lag level (lagbetween lure repetitions).Assessed and adapted individuallyduring each training performanceMissingFree-recall of two lists andinformation recognition of two listsconsisting of 12 nouns each.Assessed at pre-test and34 months after finishing thetrainingOutcomesInterindividual variability inwhite matter microstructureEducation (self-reported asyears of completed schooling)Obesity, determined from BMI(in kg/m2) computed frommeasured height and weightdata obtained at baselinePretraining, pretest score, age,length of training, pretrainingx lengthCortical volume, hippocampalvolume, ALFF, fALFFAge, crystallized intelligenceFree-recall pre-test, free recalllist 1, agePrognostic factorsRoheger et al. Diagnostic and Prognostic Research(2020) 4:7Page 6 of 23
326Hill et al. [38]75.40Non-randomized, non(10.50)controlled longitudinal studyn 102n n.a.76.85(5.27)ApoE 4Leahy, Ridout, andHolland, [24]RCTn 20n 1 due to unrelatedhealth problemsLópez-Higes et al. [39]n.a.1470n.a.n.a.17.75 (2.65)n.a.5.80 (1.10)TrainingMemory training consistingMemory flexibility program4 weeks, once a week for60 minName- and face andlist-learning program usingan imagery and judgmenttechnique and method ofloci method.2 weeks, 7 times a week for120 minMnemonic training2 weeks, twice a week for120 minObject Location Assignmentencoding and retrieval withmnemonic strategy from acognitive rehabilitationprogram2 weeks, 5 sessions 1follow-up session onemonthlaterMethod of lociNo information on trainingduration and frequencyMemory training focusedon improving verbalepisodic memory throughinstruction and practice instrategy use6 weeks, 10 60-min sessionsLearning and practicing theMethod of Loci techniqueaiming to improve episodicmemory performance.10 weeks, once a week 8 weekly online homeassignmentsOutcomesMemory factor: Immediaterecall HVLT, RAVLT, paragraphrecall, RBMT270024016801680Logical Memory and WordAutobiographical memoryspecificity in the AMT.Assessed at pre-test, post-test,and 3 month FU.Improvement in Name-Facerecall, Improvement inList-RecallRecall performance in name-facerecallMissingModified change score ofinformation Object Location AssignmentaccuracyMissingMemory improvement gaininformation scores of a list of 16 commonwords recall600MissingMemory improvement: wordinformation list test (100 words)Prognostic factorsApolipoprotein E genotypingBaseline cognitive flexibilitymeasured with the verbalfluency sub-score of ACE-III.MMSE.Rated confidence (perceivedconfidence in recalling thenames of unfamiliar faces).Medial temporal lobe volumetrics(hippocampus, amygdala,inferior lateral ventricles),standardized neuropsychologicalmeasures (RBANS Delayed MemoryIndex, TMT B)Age, education, MMSE score,depression score, neuroticismand extraversion scale of theNEO-PIInstrumental activities of dailyliving, 18 questions of theMinimum Dataset Home CarescaleWhite matter microstructure(2020) 4:7n.a.n.a.67.80(7.50)Hill et al. [37]Controlled trialn 59n n.a.16.10 (3.40)n.a.73.20(7.70)Hampstead et al. [36]RCTn 12n 1 due to ongoingdiseasen.a.30% 70% n.a.Finkel and Yesavage [35]71.29Controlled trial(6.31)n 77n 16 due to illness (n 5),frustration (n 7), badweather (n 2), no reason(n 1)No demographics separately for thememory training groups were reported15.70 (3.10)Tomaszewski Farias et al.[34]Multi-site RCT (ACTIVE)n n.a.n n.a.2373.30(2.70)de Lange et al., [33]Controlled trialn 44n 021SampleStudyTable 1 Study and participant characteristics of the included studies (Continued)Roheger et al. Diagnostic and Prognostic ResearchPage 7 of 23
4681174.69(5.74)73.00(4.20)68.73(6.05)McDougall et al., [41]RCTn 135Loss to post-test: n 8Loss to FU: n 12Loss to end of study: n 8Neely & Bäckman [42]RCTn 23n n.a.74.00O’Hara et al., [43]Non-randomized, non(7.90)controlled longitudinal studyn 212n 11369.81(4.90)McDougall et al., [40]RCTn 135Loss to post-test: n 8Loss to FU: n 12Loss to end of study: n 8Park et al. [7]RCTn 39n n.a.Rosi et al., [44]Non-randomized, non-n.a.28321910510511.36 (3.50)11.41 (4.31)15.50 (2.70)9.90 (3.10)13.39 (3.90)13.39 (3.90)TrainingMemory training program.6 weeks, once a week forMulti-strategic memory training.10 sessions once a week, eachsession lasted 1.5 hMemory training was notfurther described.Missing information on durationand frequency.Encoding operations includinginteractive imagery andmethod of loci; attentiontraining, relaxation training.Training was conducted ingroups with 11–12 subjects,met twice a week for 5consecutive weeks, eachsession lasted 1.5 hCBMEM-based intervention,based on the four componentsof self-efficacy theory4 weeks, twice a week including 8sessions and 4 booster sessionsCBMEM-based intervention,based on the four componentsof self-efficacy theory4 weeks, twice a week including 8sessions and 4 booster sessionsof cognitive stimulation,memory concepts, managementof forgetting everydayexperiences, meta-memorytraining3 months, 30 90-minsessions360900Age, education, racial/ethnicgroupEthnicity, group assignment,time, educationPrognostic factorsWord list learning (memorypracticed task), grocery listElderly verbal learning test ofthe EMS to assess verbal memory;Simple Rey Figure Test of theEMS to assess non-verbalmemory.Assessed at pre-test andpost-test (within 3 monthsafter finishing the training)Vocabulary test, Raven standardprogressive matrices, listeningAll baseline values of the scoresof neuropsychological tests, age,gender, years of educationApolipoprotein E genotyping.Recall of concrete words, recallPretest score for each dependentof objects, recall of subject-performed variable, MMSE score, age, yearstasks, recall of abstract wordsof educationAssessed at pre-test, post-testdirectly after training, 6 months FURelative gains in HVLT-R, RBMTAll outcome measures wereadministered at baseline,post-class (2 months afterbaseline), post-booster(6 months), post-classroomFU (14) and at the end ofstudy (24 months)HVLT-R, BVMT-R, RBMT.All outcome measures wereadministered at baseline,post-class (2 months afterbaseline), post-booster(6 months), post-classroomFU (14) and at the end ofstudy (24 months)MissingBVRT, Logical Memory Test,information Associate Learning Test,List-learning test.Assessed at baseline and FU4-5 years after memory training.900720720OutcomesList from WMS-III(2020) 4:7n.a.3074.69(5.74)RCTn 50n 5)StudyTable 1 Study and participant characteristics of the included studies (Continued)Roheger et al. Diagnostic and Prognostic ResearchPage 8 of 23
5611.90 (3.70)600OutcomesNumber recall.Assessed at pre-test, post-testand FUlearning (memory non-practicedtask), associative learningAssessed at pre-test andpost-test.Prognostic factorsThree measures of episodicmemory (free recall of concretenouns, free recall of abstractnouns, paired-associate recall),three measures of workingmemory (listening span, twoversions of computation span),nine measures of processingspeed, two measures of verbalknowledge, depression (ZSRDS),vocabularyspan test, letter comparison,ageAll reported values regarding sample size, dropouts, and sociodemographic variables only refer to the memory training groups. For the variables age (in years) and education (in years) means and standard deviationswere displayed, when reported. Otherwise, ranges and/or absolute numbers are statedRAVLT Rey Auditory Verbal Learning Task, BDI Beck Depression Inventory, NART National Adult Reading Test, dROMs reactive oxygen metabolites derivative compounds, FU follow-up, ALFF amplitude of low-frequencyfluctuation, fALFF fractional amplitude of low-frequency fluctuation, BMI body mass index, MMSE Mini-Mental State Examination, NEO-PI NEO Personality Inventory, RBANS Repeatable Battery for the Assessment ofNeuropsychological Status, TMT B Trial Making Test Version B, AMT Autobiographical Memory Task, ACE
Prognostic factors for change in memory test performance after memory training in healthy older adults: a systematic review . the more profound the improvement in memory test performance will be after memory training. Trial registration: CRD42019127479. . study reports needed to be available; abstracts, books, book chapters, study protocols .