Transcription
Pain Management – Anatomy,Conditions and Coding ConcernsCynthia Stewart, CPC, CCS-P, CPMA, CPC-H, CPC-IObjectivesReview Spine anatomy Look at pain causing conditions Identify types of pain Review treatment methods Discuss Documentation requirements Coding of procedures CMS coding guidelines1
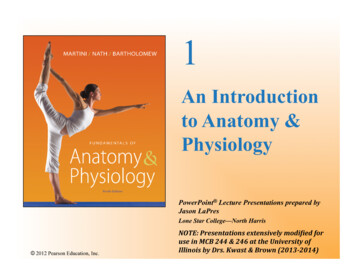
Spine – VertebraSpine Articulating Surface Facet jointEpidural space Neural Foramen 2
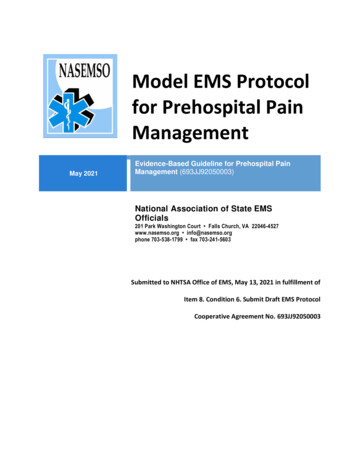
Sacrum & Sacroiliac JointSpine – Connective Tissue3
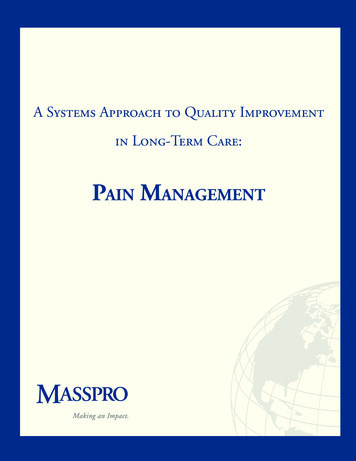
Central Nervous SystemEpidural Space Subdural Space Subarachnoid Space Spinal Meninges Dorsal Root Ventral Root Central Canal Spine and Central Nervous System4
Types of PainAcute Chronic Neoplasm associated pain Spinal painPost surgical pain Post-surgical LCD L28529 (R8)Acute“PainPain elicited by the injury of body tissues andactivation of nociceptive transducers at the site oflocal tissue damage.This type of pain is often a reason to seek healthcare, and it occurs after trauma, surgicalinterventions,, and some disease pprocesses.”5
Chronic“Persistent or episodic pain of duration or intensityfffthat adverselyy affectsthe functionor well-beingg offthe patient, attributable to any nonmalignantetiology” Failed repeated attempts at medicalmanagementg Usually has been present for at least three tosix months.Neoplasm Associated“ Includes pain associated with diseaseprogression as well as treatment.treatment ”Multiple causes include: Disease progression Treatment Co-occurring diseases6
Spinal“ generates from multiple structures in thespinespine” Condition may not be detectable Structure must be identified as source ofpain using reliable and valid diagnostictechniquesPost Surgical -Spinal“PostlaminectomyPostlaminectomy syndrome or pain followingoperative procedures of the spine, sometimesknown as failed management syndrome, isbecoming an increasingly common entity inmodern medicine.”7
Conditions –Spinal Origin Pain Disc disruptionFacet arthritisPost-Surgical – failed backMyofascial syndromesSacroiliac joint syndromeDegenerative disorders StenosisSpondylolysispy ySpondylolisthesisScoliosisSegmental instabilitySpinal hyperostosisStenosis8
Spondylolysis vs SpondylolisthesisDiffuse Idiopathic SpinalHyperostosis - DISH9
Documentation Requirements Thorough evaluation Systematic assessment Location Intensity Pathophysiology of pain Detailed Pain History Prior treatment Response to treatment Detailed physical exam Review of pertinent diagnostic testDiagnosis and Treatment Neural Blockade Trigger Point InjectionsEpidural Intrathecal InjectionsTransforaminal injectionsParavertebral Joint/Nerve BlocksSacroiliac Joint InjectionsDestruction Nerve Denervation10
Trigger Point InjectionsTrigger Point Indications History of injury or sprainDistribution pattern of painRestriction of range of motionIncreased sensitivity to stretchMuscular deconditioningFocal tendernessPalpable taut band of muscleLocal taut responseReproduction of referred pain pattern11
Treatment Noninvasive Pharmacologic Nonpharmacologic Physical therapy Invasive Trigger point injectionDocumentationHistory of onset of the painful condition,conditionand its presumed cause (injury, sprain,etc.) Thorough physical exam Presence of clinical features Results of noninvasive treatment ifapplicable 12
Codes20552 – Injection(s); single or multipletrigger point(s), 1 or 2 muscle(s)20553 – Injection(s); single or multilpletriggergg ppoint(s),( ), 3 or more muscle(s)()CMS Coding GuidelinesOne trigger point injection per day Local anesthetic is bundled Routine injections not medicallynecessary Anesthetics and corticosteroids only Saline or botanical substances not covered13
Epidural and Intrathecal InjectionsEpidural and Intrathecal Injections Diagnostic Determine dose Determine patient’s response Therapeutic Acute/sub-acute pain syndromesNerve root injuries and neuropathic painSpinal cord myelopathyComplex regional pain syndromeEpiduralE id l scarringiMultiple rib fractures or vertebral compression fracturesPhantom limb painManagement of intractable spasticityPost-herpetic neuralgia and herpes zoster14
Documentation Requirements Failed conservative management Disabling and debilitating pain Poor surgical risk or Surgery is unacceptable to patient Adjunct treatment Provide relief to aggressive rehabilitative programCodesEpidural an intrathecal injections62310 – Injection,I j ti single,i l nott iincludingl di neurolyticl ti substances,btwith or without contrast, of diagnostic or therapeuticsubstance(s), epidural or subarachnoid; cervical or thoracic62311 - lumbar, sacral62318 – Injection, including catheter placement, continuousinfusion or intermittent bolus, not including neurolyticsubstances, with or without contrast, of diagnostic ortherapeutic substance(s),substance(s) epidural or subarachnoid; cervicalor thoracic62319 - lumbar, sacral01966 – Daily hospital management of epidural orsubarachnoid continuous drug administration15
CMS Coding GuidelinesCodes 62310-62311, 62318-62319Includes insertion of needle Injection of drug or diagnostic substance Bilateral surgery indicator of “0” No 50 No LT or RTCMS Coding Guidelines One unit billed per spinal region Cervical/thoracic (62310) Lumbar/ sacral (62311)Not used for operative anesthesia Time separate Daily management (01966) 2nd day Once per day Place of service 2116
Transforaminal InjectionsTransforaminal Injections Diagnostic Identify type, site and source of pain Therapeutic Radicular pain Resistant to other treatment Surgery contraindicated Post surgical scarring or decompressive radiculitis Monoradicular pain Acute herpes zoster or post-herpetic neuralgia17
Documentation Requirements Presence of multi-levelmulti level Nerve root compression StenosisIdentified on Imaging studies Responsible for symptoms and findings Codes Transforaminal injections64479 – Injection(s),Injection(s) anesthetic agent and/orsteroid, transforaminal epidural, with imagingguidance; cervical or thoracic, single level66480 - cervical or thoracic, each additionallevel64483 - lumbar or sacral,sacral single level64484 - lumbar or sacral, each additional level18
CMS Coding GuidelinesCodes 64479 – 64484 Bilateral surgery indicator “1”1 Same level - 50 Different levels - LT and/or RT One code/unit per level First level 64479 or 64483 Second level 64480 or 64484Paravertebral Joint Injections19
Paravertebral Joint Injections Diagnostic Double-comparative Intra-articular Block of medial branch nerves Attempt to reproduce pain Multiple blocks prior to diagnosisParavertebral Joint Injections Diagnostic blocks Hypertrophic arthropathy causing back orneck pain Post-trauma neck or back pain Axial pain greater than apical pain Post fusion back or neck pain associated withsuspectedt d motionti segmentt iinstability,t bilithypermobility or pseudoarthrosis20
Paravertebral Joint Injections Therapeutic Nerve Block considered if Frequency of once per two months (or less)Initially 80% - 90% pain relief Relief of previous pain upon movementContinuingg for minimum of six weeks 50% of pain relief Continued ability to perform previously painfulmovementsParavertebral Joint Injections Therapeutic Nerve Denervation considered if Nerve block provide relief Relief of pain is of short duration EffectsshouldEffh ld lastl 6 monthsh21
Documentation RequirementsJoint level(s) injected Pre and post procedural pain scores Degree and duration of pain relief Improvement in functional status Imaging confirmation of needle placement Denervation Failed conservative treatment Studies performedCodes – Nerve Blocks64490 – Injection(s), Diagnostic or therapeutic agent,paravertebral facet joint (or nerves innervating thatjoint) with image guidance, cervical or thoracic; singlelevel64491 - cervical or thoracic; second level64492 - cervical or thoracic; third and any additionallevel(s)64493 - lumbar or sacral; single level64494 - lumbar or sacral; second level64495 - lumbar or sacral; third and any additional level(s)22
CMS Coding GuidelinesCodes 64490 – 64495 64492 and 64495 once per day Bilateral surgery indicator of “1” Same level 50 Different level LT or RT One code/unit per level Level joints not medial nerve branches T12-L1 level 64493Codes – Nerve Denervation64622 – Destruction by neurolytic agent,pparavertebral facet jjoint nerve;; lumbar or sacral,,single level64623 - lumbar or sacral, each additional level64626 - cervical or thoracic, single level64627 - cervical or thoracic, each additionallevel64999 – Unlisted procedure, nervous system23
CMS Coding GuidelinesCodes 64622 - 64627 Bilateral surgery indicator of “1”1 Same level 50 Different level LT or RTOne code per level Needle placement confirmation is integralto procedure Pulsed radiofrequency not covered Sacroiliac Joint Injections24
Sacroiliac Joint Injections Diagnostic Determine pain source Double comparative Therapeutic Low back painp Sacroiliac joint dysfunctionDocumentation Requirements Results of prior Conservative therapy Noninvasive treatmentImaging confirmation of needle placement Results of previous SI injections 25
Codes27096 – Injection procedure for sacroiliacjoint,joint arthrography and/oranesthetic/steroidG0260 – Injection procedure for sacroiliacjoint; provision of anesthetic, steroidand/or other therapeutic agent, with orwithout arthrographyCMS Coding GuidelinesCodes 27096 and G0260 Not billable for “routine”routine SI injections Bilateral surgery indicator “1” G0260 follows same guidelinesOne unit of service Imaging for needle placement is bundled G0260 – Only POS 24 26
Guidance Codes77003 – Fluoroscopic guidance andlocalization of needle or catheter tip forspine or paraspinous diagnostic ortherapeutic injection procedures77012 – Computed tomography guidancefor needle placement, radiologicalsupervision and interpretationGuidance Procedure requiring guidance Transforaminal epidural injectionsParavertebral joint/nerve injectionsParavertebral denervationsSacroiliac joint injections“Therefore, injections performed without imagingguidance will be considered inappropriate andnot reasonable or necessary.”27
Additional InformationMultiple different procedures same day Both are therapeutic Both effected structures contribute to pain Documentation supports both procedures First injection assessed with incomplete painrelief Multiple pain generators are present in patientsrequiring the stop of anticoagulants (V58.61)Additional InformationAll procedures on one claim Item 19 of CMS-1500 Indicate level of injection or denervation L4/5, or C3/4 Indicate diagnostic or therapeutic injection dx or tx28
QuestionsSourcesCMSLCD for Pain Management (L28529)Article for Pain Management –Supplemental Instructions Article (A48042)Association of Pain ManagementgAnesthesiologistseOrthopod www.eorthopod.comAMA, Current Procedural Terminology 201129
Attempt to reproduce pain Multiple blocks prior to diagnosis Paravertebral Joint Injections Diagnostic blocks Hypertrophic arthropathy causing back or neck pain Post-trauma neck or back pain Axial pain greater than apical pain Post fusion back or neck pain associated with suspect d ti t i t bilit ted motion segment instability,