Transcription
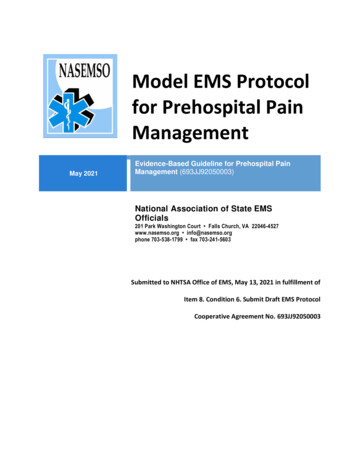
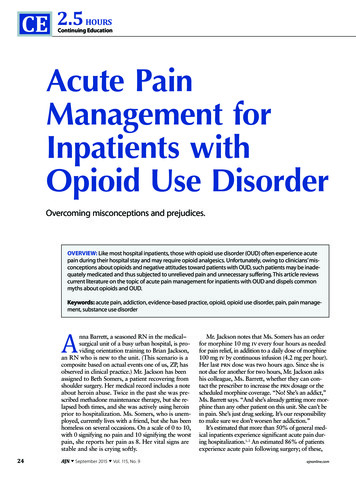
10Abdominal PainAdrian MirandaAcute abdominal pain is usually a self-limiting, benign condition thatis commonly caused by gastroenteritis, constipation, or a viral illness.The challenge is to identify children who require immediate evaluationfor potentially life-threatening conditions. Chronic abdominal pain isalso a common complaint in pediatric practices, as it comprises 2-4%of pediatric visits. At least 20% of children seek attention for chronicabdominal pain by the age of 15 years. Up to 28% of children complainof abdominal pain at least once per week and only 2% seek medicalattention. The primary care physician, pediatrician, emergency physician, and surgeon must be able to distinguish serious and potentiallylife-threatening diseases from more benign problems (Table 10.1).Abdominal pain may be a single acute event (Tables 10.2 and 10.3), arecurring acute problem (as in abdominal migraine), or a chronicproblem (Table 10.4). The differential diagnosis is lengthy, differs fromthat in adults, and varies by age group. Although some disorders occurthroughout childhood (constipation, gastroenteritis, lower lobe pneumonia, urinary tract infections), others are more common in a specificage group (see Table 10.2).PATHOPHYSIOLOGY OF ABDOMINAL PAINAbdominal pain results from stimulation of nociceptive receptors andafferent sympathetic stretch receptors. The pain is classified as visceralor parietal (somatic).Visceral PainVisceral pain receptors are located on the serosa surface, in the mesentery, within intestinal muscle, and mucosa of hollow organs. Pain isinitiated when receptors are stimulated by excessive contraction,stretching, tension or ischemia of the walls of hollow viscera, thecapsule of a solid organ (liver, spleen, kidney), or of the mesentery.Increased contraction of the smooth muscle of hollow viscera may becaused by infection, toxins (bacterial or chemical agents), ulceration,inflammation, or ischemia. Increased hepatic capsule tension may besecondary to passive congestion (heart failure, pericarditis) or inflammation (hepatitis).Afferent fibers involved in processing visceral pain are unmyelinated C-fibers that enter the spinal cord bilaterally, resulting in dull,poorly localized pain. Visceral pain is often of gradual onset, andalthough localization may be imprecise, some general rules may behelpful (Fig. 10.1).Parietal PainParietal pain arises from direct noxious (usually inflammation) stimulation of the contiguous parietal peritoneum (e.g., right lower quadrant at the McBurney point, appendicitis) or the diaphragm (splenicrupture, subdiaphragmatic abscess). Parietal pain is transmittedthrough A-delta fibers to specific dorsal root ganglia and thus isusually sharp, and more intense. It can usually be exacerbated bymovement or cough, is accompanied by tenderness over the site ofirritation, and lateralizes to one of four quadrants. Because of therelative localization of the noxious stimulation to the underlyingperitoneum and the more anatomically specific and unilateral innervation (peripheral-nonautonomic nerves) of the peritoneum, it isusually easier to identify the precise anatomic location that is producing parietal pain (Fig. 10.2).ACUTE ABDOMINAL PAINThe clinician evaluating the child with abdominal pain of acute onsetmust decide quickly whether the child has a “surgical abdomen” (aserious medical problem necessitating treatment and admission to thehospital) or a process that can be managed on an outpatient basis.Even though surgical diagnoses are fewer than 10% of all causes ofabdominal pain in children, they can be life-threatening if untreated.Approximately 55% of children evaluated for acute abdominal painhave a specific medical diagnosis; in another 45%, the cause is neverdefined.HistoryObtaining an accurate history is critical for making an accurate diagnosis but is dependent both on the ability and willingness of thechild to communicate and on the skill of the parent or guardian asan observer. The person providing an infant’s care is the best sourceof information about the current illness; the examining physicianshould try to elicit as much information from the child as possible.Some children give a good account of their illness when they aresimply asked to describe it; most children must be asked open-ended,non-leading questions. To determine the presence of anorexia, thephysician must ask questions about food intake, the time the foodwas eaten, and how that behavior compares to the child’s normalintake. The answers are often quite different from the responses tothe more general questions “Are you hungry?” and “Have you eatentoday?”During the history taking, the child should remain in the parent’sarms, at play, or comfortably seated beside the parent, as appropriatefor the child’s age. While the history is obtained, there is no particularreason that the child should be undressed. The clinician must resist theurge to speed things up by examining the child while taking the history.On occasion, when seeing a seriously ill child, the physician may needto abbreviate the diagnostic process, but taking short cuts may lead toinaccurate conclusions.Essential Components of the HistoryTime of onset of pain. Pain of fewer than 6 hours’ duration isaccompanied by nonspecific findings, and observation is often neededto determine the nature of the illness. Pain lasting from 6-48 hours ismore apt to have a cause that warrants medical intervention, althoughdelays in presentation and diagnosis in children are not unusual.Timing of the progression of symptoms must be detailed.161Downloaded for Sarah Barth (s.barth@elsevier.com) at Elsevier - Demonstration Account from ClinicalKey.com by Elsevier on March 09, 2018.For personal use only. No other uses without permission. Copyright 2018. Elsevier Inc. All rights reserved.
162Section 3 Gastrointestinal DisordersTABLE 10.1Distinguishing Features of Abdominal Pain in sFunctional: irritablebowel syndromeRecurrentPeriumbilicalNoneDull, crampy, intermittent,duration 2 hrCaused by unknown physiologicfactors; diarrhea/constipationare symptomsGastroenteritisAcute or gradualPeriumbilical, rectaltenesmusNoneCrampy, dull, intermittentEmesis, fever, watery diarrhea ordysentery (mucus and blood)Esophageal refluxRecurrent, aftermeals, bedtimeSubsternalChestBurningSour taste in mouth, SandifersyndromeDuodenal ulcerRecurrent, beforemeals, at nightEpigastricBackSevere burning, gnawingRelieved by food, milk, antacids;family Constant, sharp, boringNausea, emesis, markedtendernessIntestinalobstructionAcute or gradualPeriumbilical–lowerabdomenBackAlternating cramping (colic)and painless periodsDistention, obstipation, biliousemesis, increased bowelsoundsAppendicitisAcute or gradual(1-2 days)Initially periumbilical orepigastric; later localizedto the right lower quadrantBack or pelvisif retrocecalSharp, steadyNausea, emesis, localtenderness with/without fever;patient is motionlessMeckel diverticulitis(mimicsappendicitis)Recurrent orconstantGeneralized diffuse withperforation: periumbilical–lower abdomenNoneSharpHematochezia: painless unlessintussusception, diverticulitis,or perforationInflammatory boweldiseaseRecurrentDepends on site ofinvolvementDull cramping, tenesmusFever, weight loss, bilical–lowerabdomenNoneCramping, with painlessperiodsGuarded position with kneespulled up, “currant jelly” stoolsLactose intoleranceRecurrent withmilk productsLower abdomenNoneCrampingDistention, gaseousness,diarrheaUrolithiasisAcute, suddenBackGroinSevere colicky painHematuria; calcification on KUBx-ray study, CT scanPyelonephritisAcute, suddenBackNoneDull to sharpFever, costochondral tenderness,dysuria, pyuria, ight upper quadrantRight shoulder,scapulaSevere colicky painHemolysis with/without jaundiceCT, computed tomography; KUB, kidney, ureter, and bladder.Data from Andreoli TE, Carpenter CJ, Plum F, et al. Cecil Essential of Medicine. Philadelphia: WB Saunders; 1994:326; Behrman R, Kliegman R.Nelson Essentials of Pediatrics. 2nd ed. Philadelphia: WB Saunders; 1994:396.Location of pain. The location of the pain at its onset and anychange in location are very important (Table 10.5; see also Table 10.1).Most intraperitoneal visceral pain is a response to the stimulation ofstretch fibers in the bowel wall and is mediated through the spinalnerves. This pain is sensed as a deep, aching periumbilical pain. Paincaused by inflammation of the parietal peritoneum (acute appendicitis) is localized to the area of the inflamed organ or is diffuse if theinflammation is extensive and involves more of the peritoneal cavity.Pain resulting from obstruction of an organ is localized to the area ofthat organ and radiates to the commonly innervated region (e.g.,stones in the ureter cause intense flank pain with radiation into thegroin). Pain that is migratory or fleeting in location is rarely suggestiveof a problem requiring operative intervention.Character of pain. The character of the pain is often difficult forthe child to describe. Some older children may be able to differentiatecramping, aching, and burning sensations, but most children do notdo this well. Children can relate whether the pain comes and goes oris continuous and unrelenting. The character of the pain is usuallyunknown in the toddler and infant, although the parent can determinewhether the discomfort is constant, cramping, or intermittent. If thechild intermittently draws the legs up in a flexed position and cries, theclinician can assume that intermittent pain is present.Child’s activity level. The effect of the pain on the child’s activitiesis an important indicator of the severity of the underlying disease. Ifthe pain is sufficiently severe to awaken the child from a sound sleep,it is of much more significance than pain that occurs only at schooland never on weekends. If a child has had to avoid a favorite activity,the pain is more apt to have a defined organic cause. This applies onlyto children with acute abdominal pain because children with chronicfunctional abdominal pain may wake up from sleep and may missfavorite activities due to pain and disability. Asking whether motionworsens the pain helps differentiate peritoneal irritation or musculoskeletal diseases from more nonspecific problems. The child with acuteappendicitis lies motionless, whereas the child with a renal stone, gallstone, gastroenteritis, or pancreatitis may toss and turn and writhe indiscomfort. Localized, superficial, tender trigger points in theDownloaded for Sarah Barth (s.barth@elsevier.com) at Elsevier - Demonstration Account from ClinicalKey.com by Elsevier on March 09, 2018.For personal use only. No other uses without permission. Copyright 2018. Elsevier Inc. All rights reserved.
CHAPTER 10 Abdominal Pain163TABLE 10.2 Causes of Acute Abdominal Pain by Age GroupNeonateNecrotizing enterocolitis*Incarcerated on with volvulus*Meckel diverticulitisIdiopathic or drug (indomethacin, steroid)–induced intestinal perforationSuperior mesenteric artery syndromeInfant ( 2 yr)Intussusception*TyphlitisMesenteric adenitisSpontaneous bacterial peritonitisIncarcerated hernia*DKAUrinary tract infection*Streptococcal l obstructionMalrotation with volvulusAdolescent (12-19 yr)Appendicitis*Trauma (e.g., abuse)Pelvic inflammatory disease*Pneumonitis (lower lobe)Trauma*Hirschsprung diseaseTubo-ovarian abscessAerophagiaFitz-Hugh–Curtis syndromeSpontaneous bacterial peritonitisLabor (pregnancy)Gastroesophageal refluxHepatitisChild (2-11 yr)Appendicitis*Pancreatitis (any cause)Ectopic pregnancyGastroenteritis*Crohn diseaseTrauma*Ovarian cyst/mittelschmerz*Henoch-Schönlein purpuraSickle cell crisisHemolytic uremic syndromePeptic ulcer diseaseHepatitisOmental torsionPeptic ulcer diseasePsoas abscess or hemorrhageSickle cell anemia: vasoocclusive crisisMesenteric adenitisPancreatitisUrinary tract infectionPneumonia (lower lobe)Muscle strain (exercise, coughing)Abdominal tumorsDKAPyelonephritis/cystitisTesticular torsionTesticular torsionIdiopathic*†Torsed cryptorchid testis*Most commonly seen problem.†Gastroenteritis indicates intestinal infection with viral, bacterial, protozoal, or parasitic agents. Giardiasis and cryptosporidiosis are particularlycommon and may produce acute or chronic pain.DKA, diabetic ketoacidosis.abdominal wall may suggest abdominal wall (muscle, cutaneous) pain.The localized pain results from entrapment of cutaneous terminalbranches of intercostal nerves (7th-12th) penetrating the rectusabdominis muscle and can easily be missed without the proper historyor exam.Gastrointestinal symptoms. The presence or absence of gastrointestinal symptoms may differentiate intestinal problems (acuteappendicitis, gastroenteritis, acute cholecystitis) from those arisingfrom other intraabdominal organs (urinary tract infection, ovariandisease, abdominal wall pain).Anorexia and nausea are difficult symptoms for a small child todescribe. Often, if simply asked whether he or she is hungry, a childwill respond in the affirmative. Questions about recent food intake,normal eating habits, the last normal meal, and the current desirabilityof a favorite food often provide more accurate information about theSudden Acute ExcruciatingAbdominal Pain (Within Minutes)TABLE 10.3Intestinal PerforationPeptic ulcer diseaseAppendicitisDiverticulaLuminal OcclusionUrolithiasisCholelithiasisStrangulated herniaVascular OcclusionMidgut volvulusEmboliEndocarditisStrangulated herniaOvarian torsionTesticular torsionIntraabdominal HemorrhageEctopic pregnancyRuptured aortic aneurysmRuptured spleenDownloaded for Sarah Barth (s.barth@elsevier.com) at Elsevier - Demonstration Account from ClinicalKey.com by Elsevier on March 09, 2018.For personal use only. No other uses without permission. Copyright 2018. Elsevier Inc. All rights reserved.
164Section 3 Gastrointestinal Disorderspresence or absence of anorexia and nausea than do direct questionsabout appetite or nausea.Vomiting associated with acute pain is usually related to intestinaldisease, such as ileus, gastroenteritis, or acute problems of the gastrointestinal tract that warrant surgery. However, vomiting may occur asa response to severe non-intestinal pain such as in testicular torsion;TABLE 10.4 Causes of Chronic andRecurrent Abdominal Pain by Age Group*Infant ( 2 yr)Colic†Inguinal herniaMalabsorption‡Milk allergyHirschsprung diseaseCystic fibrosisRotational defectsMalformationsEsophagitisChild (2-11 yr)Constipation†Functional pain†Giardiasis†Peptic ulcer diseaseToxins steomyelitisAbdominal migraineDiabetes mellitusVolvulusIntraabdominalabscess§Choledochal cystAdolescent(12-19 yr)Irritable bowel syndrome†Psychogenic factors†Dysmenorrhea†Mittelschmerz†Peptic ulcer diseaseGallbladder diseasePelvic inflammatorydiseaseOvarian cystsDiabetes mellitusInflammatory boweldiseaseMalignancyGiardiasisSerositis (e.g., SLE,familial Mediterraneanfever)Intraabdominal abscess§Hereditary angioedema*See also Table 10.6.†Most common diagnoses.‡Includes lactose and sorbitol (and other fruit-juice polyalcohols)intolerance.§Hepatic, pancreatic, subphrenic, psoas, perinephric, renal, pelvic.SLE, systemic lupus erythematosus.this vomiting is usually not recurring and is not a prominent feature.Vomiting may be a sign of increased intracranial pressure, which mayor may not be accompanied by associated headache or vital signchanges (bradycardia, hypertension, irregular respirations), a bulgingfontanel, an altered level of consciousness, or neurologic findings (3rdor 6th cranial nerve palsies). Care should be taken to determinewhether the pain occurs before or after the onset of the vomiting. Withacute surgical lesions (those caused by intestinal obstruction, acuteappendicitis, acute cholecystitis), the pain usually occurs before orduring the vomiting. If the vomiting occurred before the onset of pain,the clinician should suspect gastroenteritis or another nonspecificproblem. The appearance of the vomited material is also important.Feculent or dark-green material suggests intestinal obstruction. Darkbrown or frankly bloody material indicates gastritis, prolapse gastropathy, or peptic ulcer disease as the source of pain.Diarrhea occurs commonly in intestinal diseases of viral, parasitic,or bacterial origin. The stool volume is large, and defecation is usuallypreceded by cramping pain that is alleviated by the passage of thediarrheal stool. Diarrhea may also occur in the presence of acuteappendicitis or other pelvic infections (such as those resulting frompelvic inflammatory disease, tubo-ovarian abscess); in these cases,diarrhea is caused by inflammation and irritation of an area of colonadjacent to an inflammatory mass. The diarrhea in this instance is ofsmall volume and is frequent. It is important to obtain an estimate ofthe volume and consistency of stool. Diarrhea may also occur in lesionsthat cause partial obstruction of the bowel, such as strictures, adhesions, and Hirschsprung disease. In this situation, the patient also hassome degree of abdominal distention. Constipation alone can causeacute abdominal pain and may also indicate other gastrointestinaldysfunction. Some constipated children present with a picture verysimilar to that seen in acute appendicitis but have a large amount ofstool filling the entire colon. It is therefore important to obtain a goodhistory of not only bowel movement frequency but also consistencyas well (see Chapter 16). The history and exam is sufficient to makethe diagnosis of constipation, and imaging is usually not necessary.Once the diagnosis is made, appropriate treatment should start witha proper clean-out followed by maintenance therapy. The clinicianshould not be fooled by the symptom of tenesmus, where the patienthas a feeling of constantly needing to pass stools despite having an123123FIGURE 10.1 “Visceral” abdominal pain: deep, dull, diffuse. The three general localizations of midline“visceral” abdominal pain are epigastric (1), periumbilical (2), and hypogastric (3). 1, Epigastric pain usuallysuggests disease of the thorax, stomach, duodenum, pancreas, liver, or gallbladder. 2, Periumbilical painusually implies disease of the small intestine, cecum, or both. 3, Hypogastric pain usually implicates thelarge intestine, pelvic organs, or urinary system. (From Reilly BM. Abdominal pain. In: Practical Strategies inOutpatient Medicine. 2nd ed. Philadelphia: WB Saunders; 1991:702.)Downloaded for Sarah Barth (s.barth@elsevier.com) at Elsevier - Demonstration Account from ClinicalKey.com by Elsevier on March 09, 2018.For personal use only. No other uses without permission. Copyright 2018. Elsevier Inc. All rights reserved.
CHAPTER 10 Abdominal Pain1122335448577661. Pleurisy2. Subdiaphragmaticabscess3. (Peri) hepatitis4. Cholecystitis5. Perforated duodenalulcer6. Appendicitis7. Ectopic pregnancy,tuboovarian hemorrhage,abscess, or rupture8. Perforated colon(cancer or diverticulum)A6. Appendicitis7. Perforated colon(carcinoma)1. Pleurisy2. Splenic rupture or infarct3. Pancreatitis4. Diverticulitis5. Ectopic pregnancy,tuboovarian hemorrhage,abscess, or ruptureB98765127111512233464107. Acute pancreatitis1. Appendicitisand/or pseudocyst2. Acute Crohn’s disease8. Perforated duodenal3. Ectopic pregnancy,ulcertuboovarian abscess, or9. Acute cholecystitsovarian torsion/10. incarcerated inguinalhemorrhagehernia4. Pelvic inflammatory11. Meckel’s diverticulitisdisease12. Leaking aortic5. Cecal diverticulitisaneurysm6. Colon cancer(perforation)1. Sigmoid diverticulitis2. Pelvic inflammatorydisease3. Ectopic pregnancy,tuboovarian abscess, orovarian torsion/hemorrhage4. Perforated sigmoidcarcinoma5. Perforated gastric ulcer6. incarcerated inguinal hernia7. Leaking aortic aneurysmCDFIGURE 10.2 Common and uncommon conditions that may cause “parietal” pain and localized peritonitisin the various quadrants of the abdomen. A, Right-upper quadrant. B, Left-upper quadrant. C, Right-lowerquadrant. D, Left-lower quadrant. (From Reilly BM. Abdominal pain. In: Practical Strategies in OutpatientMedicine. 2nd ed. Philadelphia: WB Saunders; 1991:703.)Downloaded for Sarah Barth (s.barth@elsevier.com) at Elsevier - Demonstration Account from ClinicalKey.com by Elsevier on March 09, 2018.For personal use only. No other uses without permission. Copyright 2018. Elsevier Inc. All rights reserved.165
166Section 3 Gastrointestinal DisordersLocalization of AbdominalPain: Referred or RadiatedTABLE 10.5REFERREDExtraabdominal Lesion PainReferred to AbdomenIntraabdominalExtraperitoneal eat vesselsPelvic organsRetroperitoneal spaceRADIATEDOrigin Is Primary Site with Simultaneously Perceived Painin a Secondary SiteCholecystitis radiates to subscapular areaSplenic injury radiates to shoulderUreteral colic (stones) radiates to testis, upper leg or groinPancreatitis radiates to backempty colon. Tenesmus can be seen in the setting of proctocolitis orinflammatory bowel disease and is often misinterpreted by the patientas constipation.Associated symptoms. The presence of headache, sore throat, andother generalized aches and pains moves the examiner away from adiagnosis of an acute problem warranting surgery and strongly suggests a viral flu-like illness. Asking the child to point to the area ofworst pain sometimes results in the child pointing to the head orthroat. The examiner must be careful to remember the whole child andnot to focus on the abdomen just because that is the area of the presenting complaint. Many systemic diseases directly or indirectlyproduce abdominal pain and must be considered in the differentialdiagnosis (Table 10.6).Family history and personal medical history. Viral gastroenteritis,other viral syndromes, and food poisoning may affect the patient’sfamily or schoolmates; it is important to ask about other familymembers, classmates, or playmates who have recently had similarsymptoms. Certain systemic and inherited diseases, such as sickle cellanemia, diabetes mellitus, celiac disease, spherocytosis, familial Mediterranean fever, and porphyria, are associated with episodes of abdominal pain. A strong family history of migraine headaches in a childwith several previous episodes of intense abdominal pain that haveresolved, who presents with a new “attack,” suggests the possibility ofabdominal migraine. The family must be asked about familial diseasesand any previous episodes of pain in the child. Previous intraabdominaloperations may result in adhesions that can cause pain, intestinalobstruction, or both. A history of previous intraabdominal surgeriessuggests the possibility of bowel obstruction. Some specific medicalillnesses result in identifiable or predictable causes of abdominal pain(Table 10.7).Physical ExaminationThe physical examination begins when the clinician enters the roomand observes the child’s activity and demeanor while obtaining thehistory. Does the child appear ill? Is the patient lethargic, rolling aboutin discomfort, alert but lying very still, or bouncing all over the room?Each of these activities conveys a message. The listless, lethargic childmay be in shock, dehydrated, and very ill. The child who is crying outloudly and generally dominating the scene probably does not have aproblem that warrants surgery and may have mild pain that is selfresolving. The child who seems only mildly ill but moves with greatcare, if at all, is assumed to have an inflammatory process until it isproven otherwise.Physical examination techniques and findings are age dependent.Younger children may have difficulty cooperating because of fear ordiscomfort. Younger children may be more cooperative if kept on theirparent’s lap. Older children should be asked to get onto the examination table with as little assistance as possible. If the child does this easily,the probability of an acute intraabdominal inflammatory process isquite low. Outer bulky clothing should be removed to allow goodexposure of the abdomen without the child having to feel vulnerable.The examination must be performed in a relaxed, friendly mannerwith attention fully focused on the child. An accurate examinationdepends on the child’s trust and cooperation. A conversation with thechild about family, friends, pets, school, sports, music, or other specificinterests of that child diverts attention (distraction) from the examination and increases cooperation. The examiner should never surprisethe child and should never lie. The first surprise or untruth, suchas the statement “This won’t hurt,” destroys any trust that hasdeveloped.Low-grade fever ( 38.3 C) is seen in early appendicitis but is alsocommon in many other diseases. The absence of fever does not excludethe diagnosis of acute appendicitis or other problems necessitatingsurgical intervention. Tachycardia may reflect anxiety or may be causedby dehydration, shock, fever, or pain. Tachypnea suggests a metabolicacidosis (shock, diabetes mellitus, or toxic ingestion), an intrapulmonary process, sepsis, or fever. The vital signs must be viewed in contextbut may be the first clue to a serious illness.Examination of the head, neck, chest, and extremities may precedethe abdominal examination. In children too young to describe thelocation of the pain, a careful examination of the ears is important,but can be performed at the end of the examination. Streptococcalpharyngitis or mononucleosis is sometimes accompanied by severeabdominal pain. Affected children will present with fever, appear ill,and have tender cervical adenopathy and an obvious tonsillitis, pharyngitis, or both.Decreased breath sounds and/or rales in a lower-lung lobe, especially on the right side, may indicate pneumonia. Children with lowerlobe bacterial pneumonia present with severe abdominal pain, highfever, tachypnea, and, on occasion, vomiting. This presentation couldmimic that of a child with peritonitis; however, the abdominal findingsare not consistent with the diagnosis of an acute intraabdominalprocess, and examination of the lungs should demonstrate thepneumonia.The abdominal examination should be performed systematicallyand with the child as comfortable as possible. Before the examineractually touches the child’s abdomen, he or she should observe it,looking for distention, inguinal masses, peristaltic waves, and scarsfrom old injuries or surgical incisions. Inguinal and femoral herniasare often overlooked but a common cause of abdominal pain. Next,the child should be asked to indicate with one finger the point of greatest pain. The point may be a vague circle in the area of the umbilicus,but if the child specifies a defined spot, the examiner should avoid thatarea until the remainder of the abdomen has been palpated.Gentleness is essential to successful palpation of the abdomen. Theexaminer must warm both hands and the stethoscope before touchingthe patient. The stethoscope is an excellent tool for palpation of theabdomen. Auscultation of the chest can simply be extended to theabdomen, with the examiner assuring the child that the stethoscopedid not hurt on the chest. The initial examination of the abdomen withDownloaded for Sarah Barth (s.barth@elsevier.com) at Elsevier - Demonstration Account from ClinicalKey.com by Elsevier on March 09, 2018.For personal use only. No other uses without permission. Copyright 2018. Elsevier Inc. All rights reserved.
CHAPTER 10 Abdominal PainTABLE 10.6167Systemic Causes of Acute Abdominal PainMetabolic, HematologicAcute porphyriaDrugs, ToxinsHeavy metal poisoningFamilial Mediterranean feverLeadHereditary angioedemaArsenicSickle cell crisisMercuryLeukemiaMushroom ingestionAcute hemolytic statesNarcotic withdrawalDiabetic ketoacidosisBlack widow spider biteHemolytic uremic syndromeAddison diseaseUremiaElectrolyte disturbancesHyperparathyroidism-hypercalcemia (urolithiasis, pancreatitis)Hypertriglyceridemia (pancreatitis)Fabry diseaseInfectious, InflammatoryAcute rheumatic feverInfectious mononucleosisRocky Mountain spotted feverMeaslesMumpsPneumonia (lower OsteomyelitisEpididymitis/orchitisThoracic nerve root dysfunctionHenoch-Schönlein purpuraTrauma/child abuseHemolytic uremic syndromeHerniaSystemic lupus erythematosusPsoas abscess or hemorrhageEndocarditisNeurologicAbdominal epilepsyPharyngitisAnaphylaxisAbdominal migraineOtherPneumothoraxBrain tumorPulmonary embolismMultiple hyHerpes zosterDysautonomia (Riley-Day syndrome)the stethoscope should be just for listening, with no pressure exerted,so that no discomfort results.Bowel sounds are usually nonspecific in most children with abdominal pain; however, in certain processes, they are helpful. High-pitchedtinkling sounds or rushes are usually associated with an obstructiveprocess. Bowel sounds in gastroenteritis are ordinarily very active andloud but may be normal. Acute appendicitis is accompanied by normalsounds in the early stages, but bowel sounds disappear with diffuseperitonitis.Watching the child’s reaction to the auscultation may be a valuableclue to areas of true tenderness. As the examiner continues to listenover the entire anterior abdomen, the pressure on the head of thestethoscope increases until the examiner is, in fact, palpating with thestethoscope. This often is a much more reliable method of eliciting truetenderness and guarding than is the palpating hand.Palpation is begun as far away from the area of pain identified bythe child as possible. The examiner’s hand should be softly placed flat(in parallel) on the child’s abdomen. Directing fingers into the abdomen(perpendicular) as a method of p
the pain is more apt to have a defined organic cause. This applies only to children with acute abdominal pain because children with chronic functional abdominal pain may wake up from sleep and may miss favorite activities due to pain and disability. Asking whether motion worsens the pain helps differentiate peritoneal irritation or musculo-