Transcription
POLICYLABE V I D E N C E TO A C T I O N B R I E F S P R I N G 20 17TR ANSITIONINGTO ADULT CARE:SUPPORTING YOUTH WITHSPECIAL HE ALTH CARE NEEDSCaren Steinway, Jennifer Gable, Sophia Jan policylab.chop.eduP R O D U C E D I N C O L L A B O R AT I O N W I T H C H O P ’ S M I N T P R O G R A M
CONTENTS2E X EC U T I V E S UM M A R Y4B AC KG RO U N D8W H AT W E L E A R N E D14W H AT W E C A N D O24C O N C LUS I O NEXECUTIVE SUMMARYThe transition from pediatricto adult health care systemscan be daunting for anyone,but is especially challengingfor young people withintellectual disabilities orother special health careneeds. Children with specialhealth care needs have oneor more chronic physical,developmental, behavioralor emotional conditions andrequire health and relatedservices beyond what childrengenerally require.1,2The health care transition frequently occursconcurrently with and has major implicationsfor other life changes, such as graduatingfrom high school, entering the workforce orcontinuing into higher education and livingindependently. At this time, youth typicallylose access to occupational, physical andspeech therapies, medical equipment andother services that were covered by insuranceor provided in schools. People with complexconditions often need these specializedservices to maintain and improve their abilityto function.2TRANSITIONING TO ADULT CARE: SUPPORTING YOUTH WITH SPECIAL HEALTH CARE NEEDS
Figure 1JOHN’S STORY: TRANSITIONING FROM PEDIATRIC TO ADULT CAREJOHN IS 23 YEARS OLD AND LIVES WITH DOWN SYNDROME, SLEEPAPNEA, HEARING LOSS, HIGH CHOLESTEROL, ADHD, OBSESSIVECOMPULSIVE DISORDER, DEPRESSION AND A HISTORY OF OTHERMEDICAL ISSUES.He continues to require multiplenot have experience caring forspecialists in addition to aindividuals with Down syndrome.primary care doctor to manageTherefore, John’s care hashis ongoing medical needs.become extremely fragmented.Although he is an adult, he stillHis mom must coordinate thissees a pediatrician and mostlycomplicated network of carepediatric specialty providerson her own, and faces not onlybecause his mom has beenadditional demands on herunable to get help in identifyingtime and resources, but also anadult providers who feelincreased sense of responsibilityequipped to provide his care.to monitor her son’s conditionsAlthough she managed to findand determine whether hean adult sleep physician, John’srequires medical attention.mom is usually told that theAt times, this has led toadult providers who participateunnecessary testing or lab workwith their insurance are notbecause there is no coordinationaccepting new patients or doaround holistic care.Challenges during this transition period can leadto lapses in health insurance coverage; reducedaccess to necessary health care services,medications and equipment; increased use of acutecare settings like the emergency department; andloss of independence or functioning.3Among adolescents with special health care needs:1 62% have difficulty with one or more of thefollowing: feeling anxious or depressed,acting-out, fighting, bullying or arguing,making and keeping friends 35% have three or more chronic conditions Nearly 30% miss one week or more of schooldue to their chronic conditionsPolicyLab researchers conducted a seriesof large surveys and interviewed providers,patients and families to understand the barriersto transitioning young patients with chronicillnesses or disabilities into adult health care,and whether there were any institutional orsystems supports in place to aid the process.In this Evidence to Action brief, we identify manyof these barriers and provide recommendationsfor pediatric and adult providers, health caresystems, and policymakers to ease the transitionprocess from pediatric to adult care for youth withspecial health care needs. These policy solutionswould help improve overall health outcomes,reduce health care costs and enhance the qualityof life for these vulnerable patients and families. 14% have developmental disabilities—including intellectual disabilities, cerebralpalsy and autism—that increase their lifelongdependence on family and caregivers 3% use or need regular physical, occupationalor speech therapyEVIDENCE TO ACTION BRIEF SPRING 20173
BACKGROUNDNearly one in five, or approximately 4.3 million, adolescents in the United States have a special health careneed, anything ranging from asthma to childhood cancer.1,4 At Children’s Hospital of Philadelphia (CHOP), morethan 44,000 patients are over the age of 18, many of whom are medically complex or have an intellectualdisability. While several factors can delay or prevent the transition of young patients—both those who aregenerally healthy and those who have special health care needs—into adult health systems, the process canbe much more difficult for individuals who need specialty care. Not only do these young adults need to seeappropriate providers who can adequately address all of their adult medical needs, but their continued useof services at CHOP means there are fewer resources available for babies, children and younger adolescents.Additionally, as researchers and scientists continue tomake lifesaving and life-extending advancements inmedicine, increasingly more children with serious andpreviously fatal conditions are living into adulthood.5For adult providers, these recent advancementshave increased the need for expertise in treatingconditions that were once exclusively seen in pediatricsettings, such as cystic fibrosis or sickle cell disease,but available training has not yet caught up with thedemand. For the patient, the transition from pediatricto adult health care can add stress to or complicate theother significant life changes they are concurrentlyexperiencing, such as graduating high school, enteringthe workforce or heading to college.Accessing appropriate medical services is complicatedfor youth with special health care needs. Many seemultiple specialists, sometimes in different healthcare systems. It takes time and resources to coordinatethe services received at all of these different points ofcare. There are often numerous office visits, telephonecalls, emails and hospitalizations that surroundthe transition of care, creating a complex web ofcommunication between providers, institutions andthe patient and family (Figure 2).In order to meet the need for this type of complicatedand costly care, most youth with very complexmedical needs rely on comprehensive, child-specificbenefits of Medicaid—either as the sole source ofinsurance coverage or to supplement limited privatecoverage. Medicaid benefits for children include Earlyand Periodic Screening, Diagnostic and Treatment(EPSDT) services—a federally mandated set ofbenefits that provides comprehensive coverage for allmedically necessary services to correct or amelioratedefects and physical and mental conditions for youthunder the age of 21.64TRANSITIONING TO ADULT CARE: SUPPORTING YOUTH WITH SPECIAL HEALTH CARE NEEDSIn addition, youth with special health care needsbenefit from Title V funding and services. Title V is afederal program that provides additional supports tothese families, complementing the Medicaid program.This program helps to facilitate the development ofcoordinated systems of care, as well as primary andpreventive care for nearly one million children withspecial health care needs. Unfortunately, youth ageout of these child-specific benefits when they turn 21,which further complicates the transition into adulthealth care.7In recognition of the importance of coordinatedtransition and transfer of care from pediatric toadult medical settings for young adults with medicalcomplexity, the National Center for Health CareTransition (Got Transition),8 the leading center ontransition from pediatric to adult health care, developeda national standard to help inform the process. Their“Six Core Elements of Health Care Transition”(Figure 3) identifies the most important componentsof the transition process, and offers guidelines forimplementation that providers can interpret and applyto meet the unique needs of each patient.Although this guidance is readily available, we knowthat it is not consistently implemented in pediatricand adult medical settings across the country. Manyyoung adults with special health care needs facepotentially life-threatening barriers to getting thecare they need, such as lapses in insurance coverage,not seeing appropriate providers, and losing accessto necessary medications and medical equipment,among many other issues. Little research has beendone to determine how the guidelines are being used inpractice or to identify the barriers to and facilitators ofsuccessful overall transition of care.
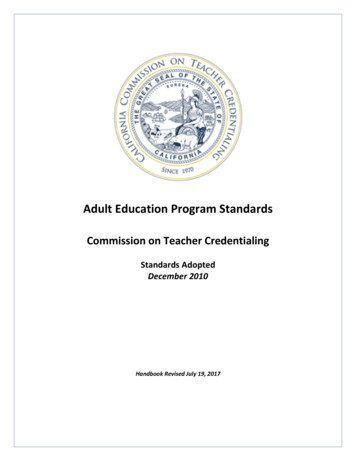
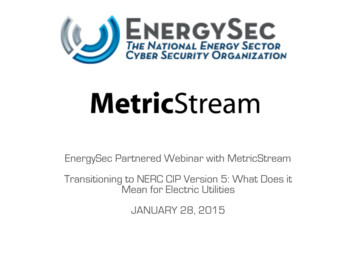
Figure 2COMPLEX WEB OF COMMUNICATIONThis complex web of communication illustrates the real-life experience of Michael, a 21-year-old with a complexmedical history. His transition from pediatric to adult care included both outpatient and hospital visits acrosspediatric and adult settings. Michael was born with a rare genetic condition that resulted in multiple birth defectsand has led to a lifetime of procedures and ongoing treatments. His experience transitioning from pediatric to adultcare represents the challenges that many individuals with complex medical needs face.ADULTHOSPITAL #1PEDGA S TI AT RR O ENT ER OCARADOIC PROVIDELO GISDIOL& EMPS ER VLOYMENICE COORS CHT SERVICEDIN ATO ROOLNURAdult PCPEmail or Phone CallID E RSTO GISATOLEUM RHBGIS T LAR O LOEN T EONS T ROURG EAG CIC SHOR ATIORD CAGIS TN O LOL MOUP ADULTHOSPITAL #2CHILDREN’SHOSPITALT ADULTPCPOOLOVLT P RRSL ES CO GISEN TT INTEPEDIARVENT RICTIONIA NAL R ADIOLOGISPUL MT ONOLO GIST SCHADUPATIENTLTADUPROVID E RSRED CAOUN WGIS TN O LOL MO PUEONRSU GA S T IC PLGEONRULSNN ER ARGEOEGIC SU ORACHTIORD CAPARENTHOMSRVE SEIC E STIERACISUPPLARMEN T S PHUIPMQELDIC AE MEH A IDA RE )E A LTND CME HOWOU( HESNURIT IN G V IS SE PatientHospitalizationOffice VisitParentEmail or Phone CallEVIDENCE TO ACTION BRIEF SPRING 20175
Figure 3GOT TRANSITION SIX CORE ELEMENTSTRANSITIONPOLICYRecognizing the challenges that youthwith special health care needs face asthey transition out of pediatric care, theMaternal and Child Health Bureau—partof the U.S. Department of Health andHuman Services’ Health Resourcesand Services Administration—and TheNational Alliance to Advance AdolescentHealth formed a cooperative agreementcalled Got Transition in 2005. Thiscollaborative aimed to break down these1barriers through innovative strategiesfor health professionals, youth andfamilies. Got Transition developed six coreprinciples to guide the transition process.THE DEVELOPMENT AND IMPLEMENTATION OF ATRANSITION POLICY. Health care systems, along with inputfrom families and youth, should develop a policy addressingthe system’s approach to the transition process. Health systemSource: GotTransition.org. About Got Transition. http://www.gottransition.org/about/index.cfm. Accessed January 5, 2017.staff should be educated on the policy and their roles intransition. The policy should be shared with youth and familiesbeginning at age 12 to 14.AGE12!2A SYSTEM OF TRANSITION TRACKING AND MONITORING.Health care systems should develop a process for identifyingpatients ready to begin at age 12 and follow them through thetransition process. A systematic transition registry shouldbe created to track transition progress. Integration with theelectronic medical record (EMR) is preferable.6TRANSITIONING TO ADULT CARE: SUPPORTING YOUTH WITH SPECIAL HEALTH CARE NEEDS
35ASSESSMENT OF TRANSITION READINESS. The providerTRANSFER OF CARE. Pediatric providers should confirm theshould conduct regular transition readiness assessments offirst adult provider appointment, transfer the patient when hepatients beginning at age 14. Patients and providers shouldor she is stable and prepare a transfer package, including thecommunicate about readiness and jointly develop transitionfinal transition readiness assessment, plan of care, medicalgoals that promote self-advocacy and self-care.summary and emergency care plan. The package should besent to the identified adult provider.TRANSITIONPL AN64TRANSITION PLANNING. Patients and providers shouldTRANSITION COMPLETION. Pediatric providers should follow-develop and regularly update the patient’s transition plan ofup with patients and caregivers three to six months after thecare. Providers should prepare patients for an adult approachlast pediatric visit to confirm transfer of care. Pediatric andto care at age 18. Patients, caregivers and providers shouldadult primary and specialty care doctors should continue todiscuss the need for decision-making supports for youthbuild collaborative partnerships.with intellectual disabilities, optimal time of transfer and theidentification of adult providers. Linkages to insurance andother resources should be provided.EVIDENCE TO ACTION BRIEF SPRING 20177
WHAT WE LEARNEDPolicyLab researchers and colleagues sought to betterunderstand the challenges of the transition process from theperspectives of patients and families, pediatric providers, andadult providers.In 2011, we conducted a national survey of adult providerswho frequently cared for adult patients with pediatric chronicconditions.9 Additional surveys and interviews between2014 and 2016 included CHOP pediatric providers, PennMedicine Health System (Penn) adult providers and patientswho had recently transitioned out of the CHOP network.10,11We compared the transition process experienced in thesesettings with Got Transition’s “Six Core Elements of HealthCare Transition” (Figure 3), and identified perceived challengesto successful transition into adult care. The barriers foundthrough the CHOP and Penn surveys were consistent with our2011 national survey, indicating that our key takeaways arelikely relevant for many providers across the country.8TRANSITIONING TO ADULT CARE: SUPPORTING YOUTH WITH SPECIAL HEALTH CARE NEEDSPATIENTPERSPECTIVESPEDIATRIC PROVIDERPERSPECTIVESADULT PROVIDERPERSPECTIVES
Figure 4KEY FINDINGS: CHALLENGES FOR PATIENTS AND PROVIDERS IN ADULT CARE SET TINGSRESOURCESWORKFLOWSTRUCTURAL & PHYSICAL SPACEAdult institutions often have lessFor patients who use medicalWhile pediatric outpatient facilitiesmultidisciplinary support staff intransport, there is a lack of flexibilityare built to have space for multipleoutpatient clinics, such as socialwhen the transport runs late, leavingfamily members in an exam room,workers, care coordinators andpatients to reschedule appointments.adult outpatient facilities can havenursing staff.Adult institutions often do not haveinadequate space for wheelchairsand other medical equipment.Adult receiving providers oftensedation services during medicalhave limited time to review thetests, which children’s hospitalsFor patients with autism orcomplete medical history of newroutinely provide when necessary.behavioral challenges who wouldyoung adult patients with specialbenefit from a quieter waiting area,health care needs, and pediatricadult outpatient facilities oftenproviders often don’t make suchlack the extra clinical space toa detailed summary available.accommodate these needs.PATIENT PERSPECTIVESThrough interviews conducted with 24 adult patients who transferred out of the CHOP network between 2013and 2015, we discovered the following common challenges that patients faced during their transition process:12Chaotic transfer and poor care coordination.Care coordination was the most commonly citedtransition concern, especially for patients thatrequired frequent visits with multiple specialists.By the time of transition to adult providers,patients and their pediatric caregivers hadlong-established routines that accommodatedthe patient’s clinical needs and caregiverlogistics, such as medical equipment, workschedules, office visit durations, and physicalaccommodations and transportation.When transferring to a new provider, new routinesneed to be established, and many adult caresettings lack the time and resources to coordinatewhat can be a complicated medical visit.“I’m trying to do at least two visits at one time[because I am wheelchair-bound and don’tlive in the city]. I would say that every weekI’ll have three different appointments backto back. People don’t understand how hard itis for me to even get to one doctor’s office.”EVIDENCE TO ACTION BRIEF SPRING 20179
Poor preparation.Children and adolescents are rarely expectedto recount their medical problems or nametheir medications and allergies in pediatricsettings without support from their parents.Consequently, they are often unpreparedto engage with adult health care systemsindependently as the primary medical decisionmakers. Patients who have transitioned toadult care often described being surprisedand unprepared for the level of autonomy andself-advocacy that adult institutions expectedthem to have.“I was highly used to having [the pediatrichospital] remind me you got to call this[doctor]. You got to call that [doctor]. So Ikind of lost that. The most eye openingthing about transition was that I had tocoordinate everything myself, like an adult.”Loss of comprehensive insurance coverage.Virtually all adolescents with the most complexmedical conditions are eligible for Medicaid tohelp cover the extraordinary cost and level ofcare they need, which often go beyond the limitsof private insurance coverage. Eligibility for thecomprehensive set of Medicaid benefits availableto children ends at age 21 (Figure 5). Additionally,the Social Security Administration redeterminesSocial Security Insurance (SSI) eligibility whena child turns 18 using adult disability standards;typically one in three such young adults lose their10TRANSITIONING TO ADULT CARE: SUPPORTING YOUTH WITH SPECIAL HEALTH CARE NEEDSSSI benefits13 and potentially Medicaid eligibility.Furthermore, young adult patients rarely receiveappropriate guidance on switching into anadult health insurance plan prior to losing theseservices and are often left scrambling for care.Loss of services.For certain conditions, such as cerebral palsy,most pediatric health care systems havemultidisciplinary clinics where a number ofdifferent specialists can evaluate a child at onetime, such as rehabilitation doctors, orthopedicsurgeons, physical therapists, occupationaltherapists, speech therapists and dietitians.This is generally not the case in adult healthcare settings that are not specially equipped tomanage patients with these complex conditions.“Once CP [cerebral palsy] clinic at thepediatric hospital is gone, then I no longerhave a feeding clinic. And I don’t have PT[physical therapy] or OT [occupationaltherapy], which I had at school.”Lack of adult providers.In transferring to adult health systems, patientsand families cite difficulty identifying adultproviders and are often left to make laboriousphone calls to provider locations. It can bechallenging to find a provider that takes theirinsurance, is accepting new patients and has anunderstanding of young adults with complexconditions that began in childhood.
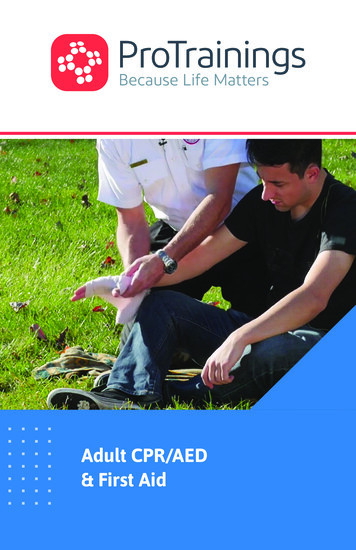
Figure 5FALLING OFF THE EPSDT AND SCHOOL SERVICES CLIFFAge:5101520SERVICES OFFERED UNDER AGE 21 REFERR AL S AND ASSISTANCE INSCHEDULING PHYSICAL EX A MS HEARING AND VISION TESTINGSERVICESOFFEREDAF TERAGE 21 GROW TH AND DEVELOPMENTALASSESSMENTS TR ANSPORTATION ASSISTANCETO AND FROM APPOINTMENTSDURING CHILDHOOD AND ADOLESCENCE, PATIENTS WITH SPECIAL HEALTH CARE NEEDS RELY HEAVILYON MEDICAID’S EARLY AND PERIODIC SCREENING, DIAGNOSIS AND TREATMENT (EPSDT) BENEFIT ANDACCOMMODATIONS PROVIDED IN THEIR SCHOOLS.Medicaid’s EPSDT benefit ensures that childrenchildren, reasonable accommodations include specialreceive screenings to catch potential healththerapies received during the school day.problems early, and guarantees coverage of allmedically necessary services, meaning those neededto support their development and address physicalAfter age 21, EPSDT is no longer federally mandated,and youth age out of their school systems.and mental conditions.Consequently, coverage and availability of servicesSchools must provide accommodations to help childrenspecial health care needs—namely physical therapy,with special health care needs participate in schooloccupational therapy and speech therapy—is oftenactivities at their full potential. For example, for somediscontinued when they reach adulthood.used to maintain function for individuals withEVIDENCE TO ACTION BRIEF SPRING 201711
PEDIATRIC PROVIDER PERSPECTIVESTo evaluate the policies, processes and obstacles surrounding the transfer of care process at CHOP,we conducted a survey of a total of 153 individuals in 201414 that compared CHOP transition of carepractices against the national standards established by Got Transition. The survey found the followingcommon challenges:Insufficient time and low adherence totransition guidelines.Participation in any one of Got Transition’s“Six Core Elements of Health Care Transition”(Figure 3) ranged from 47 percent (havinga transition policy) to 13 percent (follow-upafter transfer completion). Seven percent ofparticipants did not engage in any of the sixcore activities of transition. CHOP providersmost commonly cited inadequate time asthe main reason for not being able to follownational guidelines. Each of these activitiestake a considerable amount of time, suggestingthat additional staffing support is needed forsuccessful routine transition processes. Ourfinding is consistent with other nationalsurveys that also describe low rates ofcompleting transition activities.15,16Lack of consensus on transition policiesand procedures.Despite the existence of national guidelines,there was a lack of consensus across all of CHOP’spediatric primary care and specialty serviceson if, when and how to transfer patients toadult-focused care, particularly for youth withcomplex medical needs. Most participants saidthat the top barrier to transitioning patients waslack of agreement among providers about thetransfer process, either within one departmentor across different specialties. Very few hospitalshave transition policies that could address theseinconsistent practices and procedures.Poor documentation of transition discussionsor activities in the health record.Nearly two-thirds of participants did not updatethe patient’s electronic medical record (EMR)once care was transferred to an adult provider.Of the remaining one-third of participantswho did document the transfer in the EMR,few did so in one consistent location within the12TRANSITIONING TO ADULT CARE: SUPPORTING YOUTH WITH SPECIAL HEALTH CARE NEEDSrecord, making it difficult to track and monitortransition practices. Without consistentdocumentation of the status of transition, otherspecialty providers in the patient’s care teammay not know to also transfer their portionof the patient’s care to the adult providers,potentially further fragmenting the patient’scare. Poor documentation of whether patientshave transferred also creates confusion forpediatric emergency room staff, who may notknow whether a patient should be treated at thepediatric hospital or be transferred to the adulthospital for appropriate care.Inadequate access to adult providers withsufficient medical expertise.Pediatric providers were reluctant to transferpatients to adult providers because theyperceived a lack of adult providers who hadthe desire or expertise to take care of theirpatients. When adult providers were identified,access to these providers was partly limitedby restrictions in provider referral networksincluded by insurance. For patients withdisabilities severe enough to be eligible forSSI and consequently covered by Medicaid,many adult practices or hospital systemsdid not accept Medicaid or certain Medicaidmanaged-care products, or may cap the numberof patients on Medicaid in that practice,potentially limiting access.Failure to address medical decision making.As youth with intellectual disabilities enteradulthood, providers should assess theirability to make medical decisions on theirown in order to help them progress towardsmedical independence or to start the processof establishing a proxy in the form of a legalguardian or formal long-term caregiver.Pediatric providers in our survey reportedthat they did not conduct such an assessmentwith their patients about half of the time.
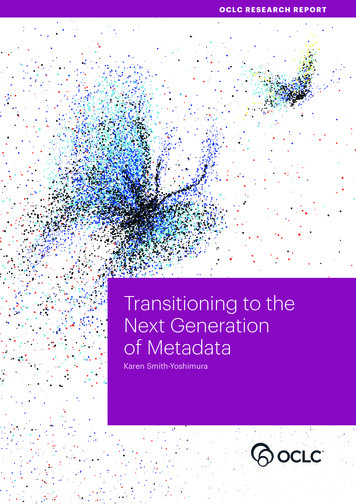
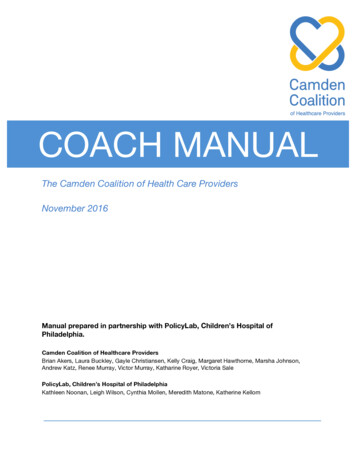
ADULT PROVIDER PERSPECTIVESIn 2011, we conducted 22 interviews9 with adult providers across the country who frequently cared foryoung adults with pediatric chronic conditions. Nearly all providers in this national study reported thatmajor challenges to caring for new young adult patients with special health care needs included notreceiving medical records from a pediatric provider; insufficient time and high administrative burdenleading to significant financial constraints; insufficient training and expertise in caring for young adultswith pediatric chronic conditions; and poor care coordination and an ill-defined medical team.In 2016, PolicyLab followed up on the 2014 pediatric provider study with a comparable survey of adultcare providers at Penn.11 Similar barriers to a patient’s transition from pediatric to adult care also emergedamong these adult providers.Inadequate time for office visits and carecoordination between visits.Approximately 60 percent of adult providersidentified the two largest barriers to taking careof young adults with childhood onset specialhealth care needs to be the amount of timeand level of care coordination required duringand between office visits. No mechanismcurrently exists to bill for non-face-to-face carecoordination for patients on Medicaid or privateinsurance, and providers are therefore notadequately compensated for the additional timeit takes to effectively manage their patients’ care.Lack of information on communityresources, care coordinationreimbursement and legal issues.Several adult providers echoed pediatric providerconcerns that many of them are neither trainednor have experience caring for adults withchronic conditions that begin in childhood.Adult providers regularly requested moreinformation on a variety of medical conditions,community resources, care coordination,enhanced reimbursement and legal issues, suchas guardianship, suggesting a need to educate andmap out non-medical resources for adult providersand for young adults with chronic disease.Inconsistent levels of communicationfrom pediatric providers.Adult providers indicated that certain typesof information from pediatric providers, suchas updated medical summaries and patientmedical records sent prior to the first adultvisit, were absolutely necessary to safely carefor a young adult patients with childhood-onsetchronic conditions (Figure 6). Only about onein four adult providers said this was always oralmost always provided. About 10 percent said itwas never available, indicating significant roomfor improvement in pediatric and adult providercommunication and handoffs.11Figure 6ADULT PROVIDER OPINION ON NECESSARY COMPONENTS OF PEDIATRIC-TO-ADULT PATIENT HANDOFFSUpdated Medical SummaryMedical Records Prior to the First VisitPediatrician Remains AccessibleAccess to Pediatric EMRVerbal Doc-to-Doc HandoffPediatric Visit After First Adult Visit0%10%20% Absolutely Necessary30%40%50% Helpful But Not Necessary60%70%80%90%100% Not HelpfulEVIDENCE TO ACTION BRIEF SPRING 201713
WHAT WE CAN DOFrom our surveys and interviews with patientsand providers, we have identified severalrecommendations that providers, healthsystems, policymakers and researchers canadopt to improve the outcomes of youth withspecial health care needs. Some of theseRECOMMENDATIONS FORPROVIDERS AND PRACTICESRECOMMENDATIONS FORHEALTH CARE SYSTEMSRECOMMENDATIONS FORPOLICYMAKERSsolutions directly address problems identifiedin the studies conducted above, and othershave been well defined in the literature aroundtransition to adulthood for young adults withchronic illness or disability.RECOMMENDATIONS FOR PROVIDERS AND PRACTICESHealth care providers are on the front lines caring for patients, and families of patients, with complex andchronic conditions. Right alongside families, they face the challenges and frustrations of coordinating care andworking to ensure that their patients are able to achieve the best possible outcomes. Transitioning care fromone network to another, particularly with young adult patients who are learning to manage their own health, isincredibly challenging. This section provides recommendations to address many of these challenges and ensure asmooth transition of care for everyone involved.14TRANSITIONING TO ADULT CARE: SUPPORTING YOUTH WITH SPECIAL HEALTH CARE NEEDS
P R O B L E M 1:Youth are unprepared to manage their own care, and many youthand their families are unaware of potential loss of services at age 21.CHOP’s MultidisciplinaryIntervention NavigationTeam (MINT)R E C O M M EN DAT I O N:Start early in preparing adolescents, or their proxy caregivers, to takeon the role of primary medical decision maker in managing their careonce they reach adulthood by:MINT is a novel clinical service Better educating youth with chronic illness on their own conditions,self-management and system navigation while still in pediatric settings.that provides comprehensive Regularly assessing transition readiness using the Transition ReadinessAssessment Questionnaire. This step is widely recommended by theAmerican Academy of Pediatrics and other professional societies, and isone of the Got Transition six core elements.17 The information from theassessment can be used to plan education for the patient and family, andcommunicate the patient’s current skills to other providers. Childrenand adolescents should be able to identify their medical problems,medications and allergies without support from their parents, or at leastknow how to access that information.transitioning from CHOP to adult Addressi
his ongoing medical needs. Although he is an adult, he still sees a pediatrician and mostly pediatric specialty providers because his mom has been unable to get help in identifying adult providers who feel equipped to provide his care. Although she managed to find an adult sleep physician, John's mom is usually told that the