Transcription
CHAPTER 3THE PATHOGENESIS,PATHOLOGY A N DIMMUNOLOGY OF SMALLPOXA N D VACCINIAContentsIntroductionThe portal of entry of variola virusThe respiratory tractInoculation smallpoxThe conjunctivaCongenital infectionThe spread of infection through the bodyMousepoxRabbitpoxMonkeypoxVariola virus infection in non-human primatesSmallpox in human subjectsThe dissemination of virus through the bodyPage122123123123123123124124126126127127129The rash129ToxaemiaPathological anatomy and histology of smallpoxGeneral observationsThe skin lesionsLesions of the mucous membranes of the respiratory anddigestive tractsEffects on other organsThe histopathology of vaccinia and vaccinia1complicationsNormal vaccinationPostvaccinial encephalitisViral persistence and reactivationPersistence of variola virus in human patientsPersistence of orthopoxviruses in animalsEpidemiological significanceThe immune response in smallpox and after vaccinationProtection against reinfectionHumoral and cellular responses in orthopoxvirusinfectionsMethods for measuring antibodies to orthopoxvirusesThe humoral response in relation to 4146146146148149152
SMALLPOX AND ITS ERADICATION122PageThe immune response in smallpox and after vaccination(cont.)Methods for measuring cell-mediated immunityCell-mediated immunity in relation to pathogenesisThe immune response in smallpoxThe immune response after vaccinationCells involved in immunological memoryReducing the risks of vaccinationInactivated virus vaccinesNon-specific mechanisms involved in host defenceBody temperatureNutritionAgeHormonal effectsInterferonGenetic aspects of resistance to smallpoxNatural selection for resistance to smallpoxSummary : the pathogenesis of smallpoxViral entry and infectionSpread through the bodyThe immune responseDeath or recoveryINTRODUCTIONThe term pathogenesis is used to describethe mechanisms involved in the productionof disease, including the spread of virusthrough the body and the physiologicalresponses of the host organism to the infection, of which the most important is theimmune response. The pathogenesis of smallpox could be studied in three ways: (1) byusing material from human patients, whichhad the advantage of direct relevance but thedisadvantage that planned experiments werenot possible; (2) by conducting experimentswith variola virus infections of non-humanprimates; and (3) by conducting experimentswith “model” infections-ectromelia (mousepox) in mice, vaccinia (rabbitpox strain) inrabbits, and monkeypox in monkeys. Each ofthese approaches had advantages and disadvantages. With human subjects, investigationduring life was limited to the sampling ofbody fluids, skin biopsy (rarely), and theexamination of postmortem material. Noinvestigations were possible during the incubation period, when most of the criticalevents in the spread of the virus through thebody and the initiation of the immuneresponse occurred. Monkeys that developed arash after infection with variola virus by therespiratory route probably provided the bestmodel system, but monkeys are 5165166166167167167animals and such experiments could onlybe undertaken in microbiologically highlysecure laboratories. For want of a better alternative, therefore, most investigations thatare relevant to an understanding of thepathogenesis of smallpox have been carriedout with other orthopoxviruses, especiallymousepox virus, since so much is known ofthe genetics and immune response in mice.But mice are not men and mousepox is notsmallpox. Arguments by analogy must therefore be developed cautiously. The results ofthese diverse investigations will be summarized in this chapter, and the informationcollated to provide an integrated picture ofthe pathogenesis and immunology ofsmallpox.Following the analysis of the pathogenesisof smallpox, we proceed to a description of thepathology and histopathology of smallpoxand vaccinia, which have been studied withmaterial from autopsies on fatal cases and, in afew cases, by taking biopsies from skin lesions.Most of this work was carried out early in thiscentury; the most recent and most comprehensive descriptions of the pathology andhistopathology of smallpox were publishedby Bras (1952a,b).Finally, this chapter presents an account ofthe immune responses in smallpox and vaccinia, which provides the rationale of the useof the tool that made the eradication of
3. PATHOGENESIS. PATHOLOGY AND IMMUNOLOGYsmallpox possible-Jennerianvaccination.Immunological intervention designed to prevent human diseases began in the 10thcentury, with variolation, and entered a new“scientific” phase when vaccination againstsmallpox was introduced in 1798 (see Chapter6). Over the past three-quarters of a centuryan enormous literature has accumulated describing the mechanisms by which vaccination induced immunity to smallpox. Unfortunately, because methods of studying cellularaspects of immunity were developed relatively recently, most of these investigations wereconcerned only with humoral immunity. Inspite of its long history, the immunology ofboth smallpox and vaccination against it arestill imperfectly understood.THE PORTAL OF ENTRY OFVARIOLA VIRUSInfection with variola virus occurred viathe respiratory tract, by inoculation throughthe skin, or, rarely, via the conjunctiva or theplacenta.The Respiratory TractEpidemiological evidence indicates thatthe usual mode of entry of variola virus wasvia the respiratory tract and that excretionsfrom the mouth and nose, rather than scabmaterial, were the most important source ofinfectious virus. In theory, infection by inhaled virus could have occurred via themucous membranes of the mouth, the nasalcavity, or the oro- or nasopharynx; or via thealveoli of the lungs. However, careful study ofthese sites in fatal cases of smallpox failed todisclose any evidence of a “primary lesion”there. Nor were patients infectious before theenanthem appeared, at the end of the incubation period. It seems, therefore, that theprimary infection in the mouth, pharynx orrespiratory tract did not produce a sizeablelesion nor did the lesion of infection ulcerateand release virions on to the surface.In the absence of data from human smallpox it is pertinent to look at an animal model.Observations by Roberts (1962a) on mousepox suggest a possible sequence of events.Fluorescent-antibody staining of sectionstaken after exposure of mice to aerosol infection showed that the first cells to be infectedwere mucosal cells of the upper and lowerrespiratory tract and alveolar macrophages.123Virus did not spread beyond the respiratorytract until the 3rd day after infection, when itwas found in free macrophages in the draining lymph nodes. At no stage did a substantial“primary lesion” develop in the respiratorytract, like that found, in both mousepox andsmallpox, after infection by cutaneousinoculation.Inoculation SmallpoxThe clinical picture of inoculation smallpox, which sometimes occurred accidentallybut was usually due to variolation by thecutaneous route, is described in Chapters 1and 6 (see Plates 6.1-6.3). A local skin lesionappeared by the 3rd or 4th day. Fever andconstitutional symptoms began on the 8thday, and the rash, which was usually much lesssevere after variolation than in naturallyacquired smallpox, appeared on the 10th or11th day. Thus the incubation period appeared to be 2-3 days shorter than in “natural” smallpox (see Chapter 1, Fig. 1.3). Observations on mice infected with mousepox byscarification (Roberts, 1962b) suggest that theshorter incubation period may have been dueto the fact that after dermal infection infectedmacrophages were transported to the locallymph nodes and thus to the circulationwithin the first 24 hours, whereas afterrespiratory infection viral dissemination bymacrophages was delayed until the 3rd day.Viraemia and rash would therefore occur afew days earlier after dermal infection.The ConjunctivaIf infection via the conjunctiva occurred a tall in smallpox, it was very rare (Rao, 1972).However, Kempe et al. (1969) noted thatoccasionally variolous conjunctivitis, confirmed by viral isolation, occurred at or evenbefore the onset of the pre-eruptive fever. Inno case was the interval between conjunctivitis and rash as long as that found betweenthe appearance of the primary lesion and therash in inoculation smallpox, which makes itdifficult to decide whether the conjunctivawas actually the portal of entry.Congenital InfectionVariola major was always severe in pregnant women (see Chapter 1). In Rao’s (1972)series, abortions or stillbirths occurred in
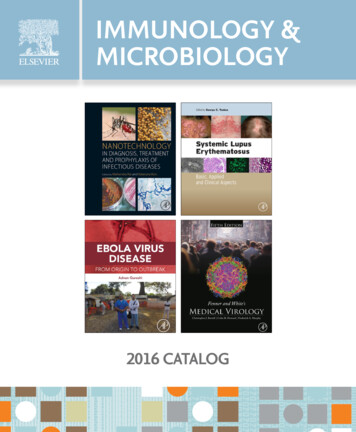
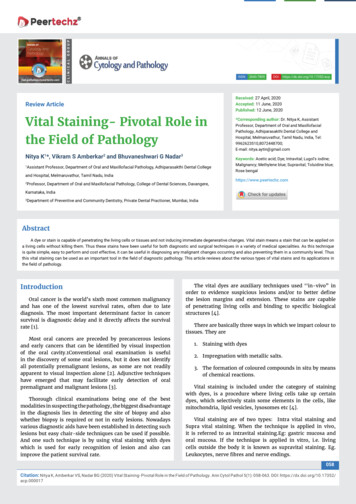
124SMALLPOX AND ITS ERADICATION35% of those in whom pregnancy terminatedand observations were possible. The majority(55 yo)of 113 babies born in hospital diedwithin 15 days, usudly within 3 days. Congenital smallpox was recognized in only 10 ofthese, but some children may have died beforea rash appeared. Nevertheless, at least half ofthe babies did not acquire infection in utero.Being so much milder than variola major,cases of variola minor in pregnant womenprovided better data on congenital infections.There were 150 pregnant women in Marsden’s (1936) series of 13 686 cases of variolaminor. Only 6 abortions are known to haveoccurred, but Marsden thought that smallpoxsometimes played a part in the induction oflabour during the last 2 months of pregnancy.Sixteen women were confined in the smallpoxhospital and bore 16 live infants (including 1pair of twins) and 1 stillborn fetus with apapulo-vesicular eruption. Twenty-sevenwomen were delivered of live infants justbefore admission to hospital, labour havingbegun at the time of the pre-eruptive fever.Marsden & Greenfield (1934) reported ananalysis of 34 of the cases concerned. In 17cases the baby escaped in utero infection. In 2 ofthese babies, born during the mother’s convalescence, the vaccination did not take; therest were successfully vaccinated, but 4 ofthem later contracted smallpox. Only 2 of the17 babies who contracted variola minor inukro died. The course of the disease was nevercoincident in mother and baby; symptoms inthe baby usually occurred 9-11 days afterthose in the mother, an interval similar to theincubation period of inoculation smallpox.The fetus was presumably infected by thegrowth of virus in the placenta, which wouldhave been infected during the stage of secondary viraemia (see below).Observation of a laboratory model (pregnant mice infected with an attenuated strainof mousepox virus) revealed that the placentas were infected and the virus grew extensively in the fetuses (Mims, 1969). Some livebirths occurred, but all such mice had widespread lesions which proved lethal, althoughthe mothers had suffered only a mild disease.THE SPREAD OF INFECTIONTHROUGHTHEBODYThe only sources of virus accessible forstudy in human smallpox during the incubation period were various secretions ofcontacts of cases, some of whom ultimatelygot smallpox, so that in order to study thespread of infection through the host it wasnecessary to use animal models. Four suchmodels have been studied : mousepox in mice,rabbitpox in rabbits, and monkeypox andsmallpox in monkeys and apes.MousepoxThe pioneering work on the pathogenesisof generalized orthopoxvirus infections,which provided a model that proved useful inunderstanding the pathogenesis of chickenpox (Grose, 1981) as well as that of smallpox,was carried out with mousepox (Fenner,1948a,b). Mice that did not die from acuteviral hepatitis developed a generalized pustular rash (Fenner, 1 9 4 8 and) the symptoms ofthe naturally occurring disease could bereproduced by the footpad inoculation ofmice with a small dose of virus.The course of events after footpad inoculation was followed by sacrificing mice atfrequent intervals and titrating the viralcontent of certain organs-theinoculatedfoot, the regional lymph node, the spleen, theskin, and the blood. The results indicated thatthe sequence of events during the incubationperiod in mousepox followed a consistentpattern (Fig. 3.1). If the appearance of theprimary lesion was taken as the end of theincubation period, it was evident that thissymptom-free period was occupied by acomplex series of events in which the viruspassed in a stepwise fashion through thebody: infection, replication, and liberation-usually accompanied by cell necrosis-first at the site of inoculation, then in theregional lymph node, and then in the deeperlymph nodes or perhaps directly into thebloodstream. It seems from the work of Mims(1964), who used fluorescent-antibody staining to identify virus-infected cells, that in theliver and spleen the phagocytic cells were thefirst infected. When infection had breachedthe macrophage barrier the virus replicatedvery extensively in the parenchymal cells ofthe liver and in the spleen, both of whichusually showed semiconfluent necrosis. A dayor so after infection of the spleen and liver,large amounts of virus were liberated into thebloodstream, and during this secondary viraemia focal infection of the skin, kidneys, lungs,intestines and other organs occurred. Therewas again an interval during which the virusreplicated to reach a high titre before visible
1253. PATHOGENESIS, PATHOLOGY AND IMMUNOLOGYVacciniaEctromelia(in m i c e )DaysdRegionalI-Regional lymphnode2-3-"3.Swelling of foot:primary lesionG10 -@;eneralized rash(very rare)03.3.0-:*:Replicationilymphoid organs.13.@Seneralized rash(common)0\ # I- 0 -@Local012 -0ulceratioi1111-Variolasecondarlesions0Days\I I-,,.Early rash papule')k!Legional lymphnode/iraemiafocal ViraemiainfecI1 -1403.6-I3 -4Replication -;*:in lymphoid organsliver5-89-,3.4-7(I-V a r i o l a byinoculationqs-IUpper o r lowerrespiratory tract-23.-3Regional lymph node-4.1-5Replicationin lymphoid organs.1Viraemia-83.3.Flat andhaemorrhagic-9-10Ordinary- - 1 Itype-12rash-I3- 140IS--7-IS--1617 --I71618 19-180-\lopermanent Always20 -scar21 -a scarI,.\'-,'IVariablescarring- I90- 20Alwaysa scar-21- 2222 23 24 -- 23Macule25 -;:: Papule26 -@Vesicle@Pustule- 24\ ' I27 -28 29 -30 31-32 -- 25-26-27- 28- 29Scab0- 30Scar0- 31- 32Fig. 3. I. The spread o f virus around the body and the evolution and healing o f skin lesions in a model system(ectrornelia. after Fenner. I948b), and in vaccinia, inoculation smallpox, and "natural" smallpox in man. Forvaccinia and inoculation smallpox, the right-hand column represents lesion at site o f inoculation, left-handcolumn represents generalized skin lesions. (Based on Dixon. 1962.)
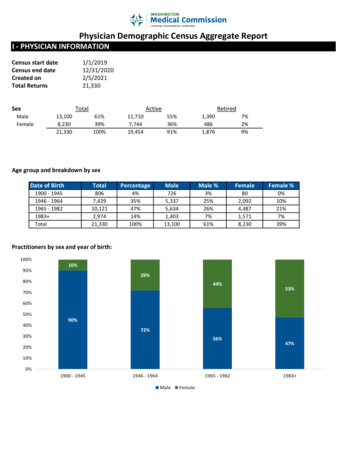
126SMALLPOX AND ITS ERADICATIONchanges were produced, so that a period ofabout 2 or 3 days usually elapsed between theappearance of the primary lesion and the focallesions of the secondary rash (Fig. 3.1). Thesecondary viraemia was mainly cell-associatedand only small amounts of virus could berecovered from plasma or serum. Mims (1964)demonstrated by fluorescent-antibody staining that circulating lymphocytes and monocytes contained viral antigen.Although this work provided a generalexplanation of what happened during thelong incubation period of the generalizedexanthemata (Fenner, 1948b), mousepox isnot a satisfactory model for smallpox. Apartfrom the difficulty of comparing events inmice and men, the usual mode of infection inmousepox is via skin abrasions (it is thusanalogous to inoculation smallpox), ratherthan by the oropharynx or respiratory tract.More important, mousepox appears to beunusual among the generalized orthopoxvirus infections, and certainly different fromhuman smallpox, in that the spleen and liverare major target organs for viral replication. In mousepox these organs are clearlythe “central foci”, established during the incubation period, from which virus is continually released into the bloodstream, withPlate 3.1. Frank Fenner (b. I 9 14). Formerly Professor of Microbiology in the John Curtin School ofMedical Research of the Australian National University, Canberra. H e is shown here inoculating eggson the chorioallantoic membrane, a method used forassays of orthopoxviruses and neutralizing antibodiesto them, and for the differentiation of variola virusfrom other poxviruses.ensuing infection of the skin and other organsand tissues.Subsequent research into the pathogenesisof smallpox was carried out with otherlaboratory models-rabbitpox and monkeypox in rabbits and monkeys respectively, andnon-human primates experimentally infectedwith variola virus.RabbitpoxStudies on the pathogenesis of rabbitpox, asevere disease of rabbits produced by certainstrains of vaccinia virus, did not add much tothe picture that had emerged from experiments with mousepox. After rabbits wereinfected by the respiratory route (Bedson &Duckworth, 1963 ; Westwood et al., 1966),virus spread through the body in a stepwisemanner. Viral isolations could always be madefrom the lungs, and very high titres occurredin the gonads and the adrenal glands. Theincubation period, from infection until theonset of fever, was 4-6 days. A rash usuallyappeared on about the 6th day, although oftenrabbits died before the rash became evident(“pockless” rabbitpox ; Christensen et al.,1967).In spite of the early replication ofrabbitpox virus in the lung, rabbits were notinfectious until nasal and conjunctival discharges appeared, and environmental contamination appeared to be maximal 6-7 daysafter infection. Examination by fluorescentantibody staining revealed that after aerosolinfection primary lesions developed at twodistinct sites in the respiratory tract-thebronchioles and the alveoli. It was also foundthat as well as being spread to the bloodstreamvia the lymphatics, rabbitpox virus couldspread directly from the bronchiolar or alveolar lesions to adjacent blood vessels.Viraemia was mainly leukocyte-associated.Animals that died early, before the rashappeared, had viraemias which increasedexponentially to reach very high titres a t thetime of death ;those that died later had muchlower titres (Westwood et al., 1966). Thissituation invites comparison with the levelsof viraemia in haemorrhagic-type and discrete ordinary-type smallpox respectively (seebelow).Monkey poxCynomolgus monkeys are highly susceptible to monkeypox and usually develop a
3. PATHOGENESIS, PATHOLOGY AND IMMUNOLOGYgeneralized rash (Magnus et al., 1959).Wenner and his colleagues (review: Cho &Wenner, 1973) studied the pathogenesis ofmonkeypox in cynomolgus monkeys infectedby intramuscular inoculation. These investigations confirmed that in orthopoxvirus infections of primates, as well as in those of miceand rabbits, there was a stepwise progressionof infection, a generalized rash developingafter viraemia had been established owing tothe replication of virus in the internalorgans. Prior to the development of the rashthe virus replicated in the spleen, tonsils andlymph nodes, without producing extensive orsevere lesions. Generalized lymphadenopathydeveloped in the 1st week after infection andpersisted until the end of the 3rd week.Enlargement of the cervical and inguinallymph nodes is a feature of monkeypoxinfections in chimpanzees (McConnell et al.,1968) and humans (see Chapter 29).Variola Virus Infection in Non-humanPrimatesThe monkey was the first animal to whichvariola virus was transmitted (Zuelzer, 1874)and monkeys were extensively used in earlystudies of cross-immunity between variolaand vaccinia (Brinckerhoff & Tyzzer, 1906 ;Horgan & Haseeb, 1939). Experimentalstudies of the pathogenesis of smallpox in thecynomolgus monkey ( M a m a irus) were carried out by Hahon & Wilson (1960) andNoble & Rich (1969). After an incubationperiod of about 6 days, inoculated animalsusually developed a generalized rash that wassparse on the face, hands and feet-siteswhere the rash was usually more intense inhuman smallpox. After infection by aerosol,variola virus replicated in the lung, andsecondary sites of replication were established in the lymph nodes before viraemiaoccurred. Although the study was complicated by pre-existing bronchopneumonia, Hahon & Wilson (1960) failed to demonstrateany major focus of local viral replicationin the lungs even though they yielded asubstantial amount of virus during the incubation period. Natural transmission to othermonkeys could occur by the airborne route,with an incubation period of 8-16 days (seeChapter 30, Fig. 30.1).Only 2 out of 109 rhesus monkeys ( M a m amulatta) infected by aerosol with variola major127virus died, but all developed fever on the 5thday and a rash between the 6th and 11t h days(usually on the 7th or 8th day). Assay ofvarious organs revealed high titres in thelungs and skin, with occasional isolationsfrom the blood and spleen. Large amounts ofvirus were recovered from all organs tested ina monkey that died on the 11th day.Rao et al. (1968b) showed that cortisonegreatly increased the severity of smallpox inbonnet monkeys ( M a m a radiata) inoculatedintradermally with variola virus. None of 14controls died, whereas 12 of the 16 animalsgiven cortisone and 1 pregnant monkey diedafter suffering from a much more severeprimary lesion and generalized rash than wereseen in the control animals. Virus could bereadily recovered from most of the internalorgans of the cortisone-treated animals at thetime of their death. This increased severity iscomparable to that seen in pregnant womenwho contracted variola major (Chapter 1).Orang-utans (Gispen, 1949) and chimpanzees (Kalter et al., 1979) can be naturallyinfected with variola virus (see Chapter 30),and may suffer a severe disease with anextensive rash (see Plate 30.1). Baboons (papi0gnocephalus) inoculated with variola virus byscarification developed a rather “dry” locallesion but no rash; virus was recovered fromthe blood, throat swabs and rectal swabsbetween the 4th and the 7th days afterinfection (Heberling et al., 1976).Smallpox in Human SubjectsThe 4th and 5th columns of Fig. 3.1illustrate diagrammatically, on the basis ofavailable data, the sequence of events inhuman smallpox after intradermal inoculation and after infection via the respiratorytract. Investigations in human subjects relevant to the pathogenesis of smallpox havebeen limited to virological and serologicaltests carried out in hospitalized patients orcase contacts. Such studies were limited to theexamination of blood, urine, and throatwashings in cases after the onset of fever andthroat washings from case contacts duringwhat was potentially the incubation period.These investigations were important becausethey provided information that permittedarguments about the pathogenesis based onmodel systems to be developed with moreconfidence.
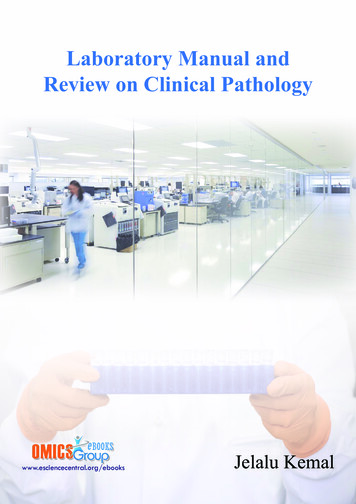
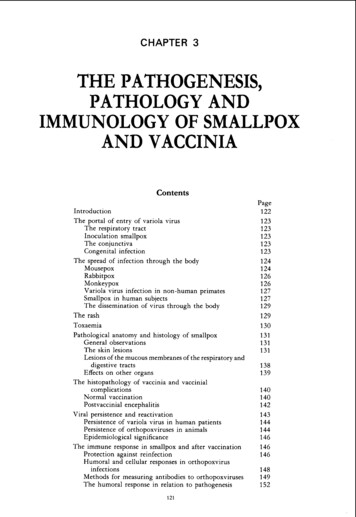
128SMALLPOX AND ITS ERADICATIONViraemzaNo precise observations have been made onthe distribution of variola virions among thevarious components of the blood in cases ofsmallpox ; by analogy with other poxvirusinfections viraemia would have been expectedto be primarily cell-associated. Most assays ofviraemia in smallpox were made with serumor lysed whole blood, the material beingassayed on the chorioallantoic membrane ofchick embryos (Downie et al., 1950, 1953,1969b; Mitra et al., 1966).Although viraemia must always have occurred, virus was only rarely recovered fromthe blood or serum from cases of ordinarytype smallpox. Downie et al. (1950, 1953)and Mitra et al. (1966) recorded one or twopositive results out of many attempts in suchcases and then only in the first few days of thedisease. The picture in haemorrhagic-typesmallpox was quite different. Virus was readily recovered from the blood of all cases andthe titres were usually high, as determined byconfluent lesions on the membrane (Downieet al., 1953,1969b) or by titration (Mitra et a].,1966; Sarkar et al., 1969). In these patientsviraemia usually persisted until the patientdied. Downie et al. (1969b) noted that viraemia was consistently much higher in cases ofearly than of late haemorrhagic-type smallpox. They also examined the serum by gelprecipitation and complement-fixation testsfor the presence of soluble antigens of variolavirus ; cases of haemorrhagic-type smallpoxusually had an antigenaemia (Fig. 3.2). Complement-fixation tests revealed antigenaemiain 31 out of 46 sera tested, the level being, ingeneral, proportional to the extent of theviraemia. The gel-precipitation test was lesssensitive, revealing antigen in only 16 out of45 sera tested, all from cases of early haemorrhagic-type smallpox with severe viraemia.Thus haemorrhagic-type smallpox appearsto have been associated with overwhelminginfection and the continued release of virusinto the bloodstream ; in ordinary-type smallpox demonstrable viraemia was usually restricted to the pre-eruptive and early eruptivestages of the disease.Oral and pharyngeal secretionsBecause there is no tough stratum corneumon the oral and pharyngeal mucosae, thelesions of the enanthem ulcerated very soonafter their formation (see Plate 3.7), releasing. .160 70 l2486. .:@.em&. ."1210o0It -Iox.-mE%. - -xx024&.:m.6m8Lm010x12Day of illnessFig. 3.2. Antigenaemia and viraemia in haemorrhagic-type smallpox. 0 early haernorrhagic type:x late haemorrhagic type; 0, @ vaccinated;S survived (all other cases died). (From Downiee t al., I969b.).large amounts of highly infectious virus intothe saliva. The viral titres in throat swabs wereat their maximum on the 3rd and 4th days ofthe disease (i.e., at the onset of the rash) andwere highest, and persisted for the longestperiod, in the most severe cases (Sarkar et al.,1973a ; see Chapter 4). In fatal cases virus wasusually still present in the throat swabs at thetime of death ; in non-fatal cases it was foundfor 7-9 days after the onset of fever in discreteordinary-type smallpox and sometimes for aslong as 13 days in non-fatal confluent ordinary-type smallpox.More important, from the point of view ofpathogenesis, are reports of the recovery ofvirus in throat washings taken from casecontacts who developed smallpox. Carefullaboratory studies by Sarkar and his colleaguesshowed that household contacts of cases ofsmallpox sometimes harboured detectableamounts of variola virus in their throats.Using a single throat swab, Sarkar et al.(1973b) isolated variola virus in 34 out of 328subjects who had been in close householdcontact with 52 index cases of smallpox forperiods of between 4 and 8 days. Only 4 of the
1293. PATHOGENESIS, PATHOLOGY AND IMMUNOLOGY34 contacts with positive throat swabs subsequently developed smallpox, the symptomsappearing 5-6 days after virus was isolated. Ina follow-up study (Sarkar et al., 1974), positive results were reported in 5 out of 51 closefamily contacts examined, only 1 of whomsubsequently developed smallpox (Table 3.1).Serial testing showed that virus could sometimes be recovered from the throats of vaccinated contacts, most of whom did not developclinical smallpox, for as long as 10 days.F. Huq (personal communication, 1982)confirmed Sarkar’s findings, but recorded amuch smaller proportion of positive results.Using a similar laboratory procedure, shefound 3 positives (all in unvaccinated subjects, and all of whom subsequently developedsmallpox) among 168 contacts who wereexamined within a week of the developmentof rash in the index subjects.The finding of virus in throat swabs ofcontacts of acute cases is not altogethersurprising ; presumably virus replicating inan asymptomatic “primary lesion” in thefauces or elsewhere in the oropharynx wasreleased into the oral secretions or could beobtained by swabbing the fauces. However,such virus as was present in the oral secretionsduring the incubation period was of little orno epidemiological importance. The onset ofinfectivity in the vast majority of casescoincided with the development of the rashand was due to the release of virus from theulcerated surfaces of the lesions of the enanthem.bloodstream as cell-associated particles, although some virus was always found free inplasma. In cell cultures, enveloped forms ofvaccinia virus were more important thannon-enveloped forms in the dissemination ofvirions over a distance (Boulter & Appleyard,1973), as shown by the “anti-comet’’ test (seePlate 3.10). Payne (1980) showed that thecapacity to spread to distant cells in monolayer cultures and to distant organs in themouse was correlated with the production ofenveloped virions (Table 3.2).Unfortunately, no observations were evermade to determine whether enveloped virions occurred in infections of monkeys orhuman beings with variola virus, nor havesuch observations been reported with ectromelia or monkeypox viruses.THE RASHThe primary event for the production ofthe focal lesions of the rash in orthopoxvirusinfections is the localization, in the smallblood-vessels of the dermis, of virus particlesthat circulate in the bloodstream, either freelyin the plasma or more commonly within virus-infected leukocytes. Subsequently,adjacent epidermal cells are infected and theskin lesion develops as described below.In the infection of laboratory animals withorthopoxviruses, skin areas so treated as topromote a local inflammatory response areassociated with an increased density of skinlesions (vaccinia in rabbits : Camus, 1917 ;ectromelia in mice : Fenner, 1948a). Numerous observations (Ricketts, 1908 ; MacCallum& Moody, 1921) attest to the effect of mildtrauma leading to local vasodilatation on thedensity of skin lesions in different parts of theThe Dissemination of Virus throughthe BodyOrthopoxvirions were principally disseminated through the body in the lymph andTable 3. I. Prolonged presence of variola virus in throat swabs from contacts of cases of smallpox (dataexpressed as log pock-forming units per swab)Serial no. of earsyearsVaccinationscar Days after onset of fever in index cased4610II.4.0.2.02.0.1.800-3.0 . .I21417Developed smallpoxDeveloped smallpox1.91.91.83.02.92.9.3.32.91.7.a . . data not recorded.Sarkar et al.
the genetics and immune response in mice. But mice are not men and mousepox is not smallpox. Arguments by analogy must there- fore be developed cautiously. The results of these diverse investigations will be summar- ized in this chapter, and the information collated to provide an integrated picture of the pathogenesis and immunology of