Transcription
ALUMNIMAYO CLINIC ISSUE 2 2018 DEEP SPACEMEDICINERESEARCHPROGRAMPET PROJECTNEURO THENAND NOW
LETTER FROM THESECRETARY-TREASURERI remember when I was a young surgeon navigating theresearch waters. It helps to have strong mentors whoserve as role models, provide encouragement and support, and help you identify and manage your strengthsand weaknesses. It also is critically important to work atan institution that supports research endeavors. Havingone and not the other is a formula for frustration, asI discovered at some other institutions when I wasstarting out. I was very fortunate to land at Mayo earlyin my career and be blessed with kind, generous andwise mentors in a rich research environment. Mayoexcels at fostering young investigators because theMayo environment nurtures mentoring and allowsus the time to talk, teach and share. Mayo Clinic’sYoung Investigators Research Symposium (page 40) isa wonderful forum for young researchers across ourschools to share their work with the Mayo communityand get experience and feedback presenting it to seniorinvestigators, some of whom may become futurementors. I served on the Advisory Committee for theevent so I may be biased, but I feel strongly that thisbiennial event is invaluable in reinforcing the cultureof scholarly investigation, sharing and teamwork thatare the hallmarks of the Mayo research community.Diversity also is a hallmark of a rich researchcommunity; I strongly believe that a diverse staff ismore creative, open and inquisitive. Yet there arechallenges in creating a diverse faculty. The storyabout two people I admire greatly, Drs. NiluferErtekin-Taner and Rosa Rademakers at Mayo Clinicin Florida (page 24), discusses some of the uniquechallenges women investigators face. I know we cando better to support our women colleagues. Pleasetake note of the query on page 31 asking for yourfeedback about our forming a subgroup of the AlumniAssociation for women physicians and scientists.PETER AMADIO, M.D. (OR ‘83) Secretary-Treasurer, Mayo Clinic Alumni AssociationLloyd A. and Barbara A. Amundson Professor of OrthopedicsBe sure to read the story on page 42 about one of ourrecent medical student graduates and his young facultymember mentor. It’s a reminder that you don’t have to begray-haired and nearing retirement to be a life-changingmentor to a student or trainee. Having the opportunityto mentor others has been a wonderful part of my careerat Mayo. Be sure to sign up for Alumni Connect, theAlumni Association’s mentorship program, to share yourexperience and insights with a Mayo medical student.Alumni Connect is one tiny portion of what theAlumni Association does for students, trainees and30,000 alumni around the world. I’d like to thankthose of you who donated more than 39,000 aboveand beyond annual dues payments in 2017. Yourgenerosity helps us do more to strengthen our alumnicommunity and nurture Mayo’s many trainees, whowill become our future Alumni Association leaders.
NEURO FEATURES02Neuro then and now32 Mayo Clinic Alumni AssociationDonald C. Balfour Award forMeritorious ResearchA look back at the origins of neurologicsurgery and neurology at Mayo Clinicand the standouts they are todayYogesh Reddy, M.B.B.S. — Translatingideas into clinical practice “is whatresearch is all about”08 Deep space medicineresearch programShooting to facilitate missions to Marsand improve health on Earth12Pet projectUsing artificial intelligence to forecastand prevent epileptic seizures20MS or not MS?Mayo Clinic Neuroimmunology Labanswers the question24Edward C. Kendall Award forMeritorious ResearchCREST reduxMayo Clinic leads the way in investigatingoptimal treatment for carotid stenosis1636 Mayo Clinic Alumni AssociationNeuroscience powerhousesRosa Rademakers, Ph.D., and NiluferErtekin-Taner, M.D., Ph.D., share space,support and successPengfei Song, Ph.D. — Building bettereyes to help radiologists see more clearly40 Mayo Clinic Young InvestigatorsResearch SymposiumYoung investigators get their feet wet42On the shoulders of giantsMentor helps med student find his nicheand realize his dreams44Know your boardThomas Smith, M.D.MAYO CLINIC UPDATE46 Mayo Clinic news and obituariesAbout the cover: Alejandro Rabinstein, M.D., leads MayoClinic’s deep space medicine research program.ISSUE 220181
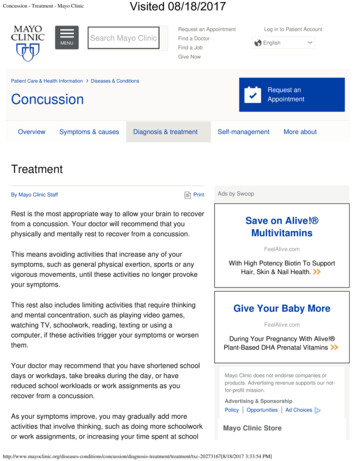
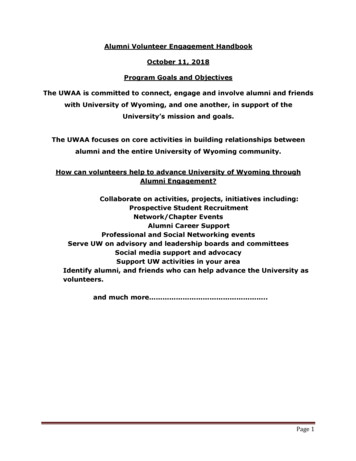
NEURO THEN AND NOWMayo Clinic’s departments of Neurology and Neurosurgeryrepresent one of the largest and most comprehensiveneurological practices in the world. Mayo Clinic Alumni looksat the origins of these departments and the physicianswho blazed trails to advance them.Throwback neurologic surgeryEmil Beckman, M.D. (back to camera), performssurgery before visiting neurosurgeons around 1915.2MAYO CLINIC ALUMNINeurologic surgery at Mayo Clinic began with earlyefforts by Charles H. Mayo, M.D., and Emil Beckman,M.D. (S ‘07), including procedures for trauma,infection, tumor, epilepsy and hemorrhage.In 1891 Dr. Mayo published an article in whichhe described two neurosurgical cases: drainageof an intracranial epidural abscess and ligation ofthe common carotid artery for a traumatic carotidcavernous fistula. In 1906 he published an article onsurgery for tic douloureux. He continued to expandbeyond a busy general surgical practice to includeprocedures for epilepsy and “spasmodic wry-neck.”Dr. Beckman joined the practice in 1907, becomingthe fourth surgeon at Mayo Clinic. Neurosurgerywas not held in high esteem at the time. Dr. Beckmanwas the first member of the surgical staff to developa major interest in neurologic surgery. He wrote29 papers on facial paralysis, trigeminal neuralgia,removal of spinal cord tumors, decompression ofthe spinal cord and repair of spina bifida. He diedunexpectedly in 1916 at age 44.
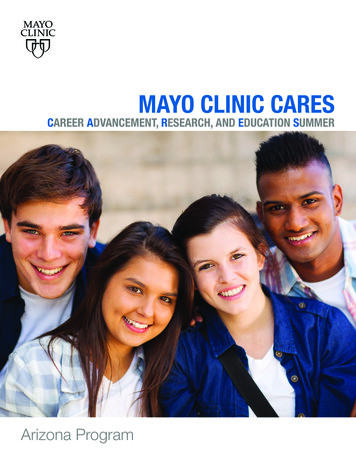
Early Mayo Clinic surgeons Emil Beckman, M.D.(left), and Alfred Adson, M.D.Alfred Adson, M.D. (S ’17), came to MayoClinic as a surgical fellow in 1914 and worked as anassistant to the Mayo brothers, E. Starr Judd, M.D.(S ‘04), and Dr. Beckman. He’d assisted for only fivemonths when Dr. Beckman died:“I suddenly found myself without a chief and withouta surgical service, with eight months of my three-yearfellowship to complete ”On Nov. 9, 1916, after the memorial service forDr. Beckman, Dr. Adson was summoned to thewaiting room of Drs. William (Dr. Will) and CharlesMayo. They asked him to join the Mayo Clinic staffas a junior surgeon. Dr. Will told him, “You will, ofcourse, be expected to look after the few neurologicalcases that will come to the Clinic. Feel free to refercases to Doctors (Harvey) Cushing (of Baltimoreand Boston), (Charles) Frazier (of Philadelphia) and(Charles) Elsberg (New York City) unless you feelqualified to handle them yourself.”In the next few years, Dr. Adson told his colleagues:“Dr. Will wants me to cut out all general surgery anddo nothing but brain surgery. I don’t want to do that.The future of brain surgery is so uncertain, everybodyis doing it. There are so few patients you can really help.The mortality is terrible. If I limit myself to this field andit continues the way it has, I’ll be out of general surgeryand may not be able to get back in. I told Dr. Will Iwanted to keep my fingers in general surgery for at leastthree years. If the prospects in brain surgery becomebrighter I’ll be willing to drop general surgery and limitmyself to brain surgery.”Eventually Dr. Adson agreed to devote his surgicalefforts to neurologic surgery and to developing thespecialty at Mayo Clinic as long as Dr. Will wouldmeet his demands: that neurosurgery encompassall facets of surgery related to the nervous system,that neurosurgery be an independent division andnot a section of the Department of Surgery, and thatneurosurgeons have the same financial benefits asgeneral surgeons.Dr. Will agreed, and the Department of Neurosurgery was established as a separate entity in 1921with Dr. Adson as chair.He became a leading neurosurgeon and pioneerin the surgery of the autonomic nervous system,development of the upright position for certainprocedures, vertical incision for the temporalextradural approach to the gasserian ganglion, anddiagnosis and alleviation of some of the “outletsyndromes” of the upper extremities. He describedthe transcranial approach for repair of cerebrospinalfluid rhinorrhea and the straight lateral incision forunilateral suboccipital craniectomy. He also designedmany instruments for neurosurgical procedures.In 1949 Dr. Adson was selected as one ofMinnesota’s 100 living distinguished citizens. He waspresident of the Minnesota Medical Society and afounding member of the American Board of Surgery,Society of Neurological Surgeons, and AmericanBoard of Psychiatry and Neurology. He co-sponsoredthe formation of the American Board of NeurologicalSurgeons and became its chair.Throwback neurologyDr. Will also was a force behind the development ofMayo’s neurology practice. In 1913 he asked WalterShelden, M.D. (N ’13), an internist-neurologist,to start a neurology section. From the start, theMayo Clinic’s first neurology section head Walter Shelden,M.D. (left), and subsequent chair Henry Woltman, M.D.ISSUE 220183
From its humble beginnings, the Department of NeurologicSurgery has grown to become one of the largest in North America,with more than 10,000 procedures performed by a staff of about45 neurosurgeons across all three Mayo Clinic campuses.section was aligned with internal medicine, givenDr. Shelden’s background, with neurology officeslocated near internists and ophthalmologists andclose relationships fostered with pathology andneurosurgery. Dr. Shelden wanted separationfrom psychiatry, unlike some contemporaryneuropsychiatrists.Dr. Shelden was head of the neurology sectionuntil 1930. He was nicknamed Pop because of hisfatherly attitude toward trainees and associates. Hetaught approximately 45 neurology residents between1919 and 1943.One of his students, Henry Woltman, M.D. (N ’17),joined the section in 1917 and chaired neurology from1930 to 1954. Dr. Woltman brought neurology at MayoClinic to national prominence. He conducted researchon the neurologic manifestations of pernicious anemia,peripheral neuropathy and diseases of the spinalcord. In 1929 he and pathologist James Kernohan,M.D. (PATH ’26), described notching of the cerebralpeduncle due to contralateral brain tumor, which wassubsequently named the Kernohan-Woltman notch.Edward Lambert, M.D., in the EMG labhe founded in 1947.4MAYO CLINIC ALUMNIOther Dr. Woltman eponyms include Woltman’s signof myxedema and Moersch-Woltman syndrome.Clinical neurophysiology played an important rolein the early history of neurology at Mayo Clinic. Thefirst electroencephalogram (EEG) at Mayo Clinic wasperformed by Edward (E.J.) Baldes, M.D. (BPHY ’34),in 1936. Edward Lambert, M.D. (PHYS ’43), foundedthe electromyography (EMG) lab in 1947, the sameyear he was awarded the U.S. President’s Certificateof Merit for his work on the effects of acceleration inman. Dr. Lambert was a pioneer in nerve conductionand EMG approaches to neurology. With colleaguesLealdes Eaton, M.D. (I ’34, N-PSY ’36), and E. DouglasRooke, M.D. (I ’41, N ’49), Dr. Lambert describedmyasthenic syndrome — later named Lambert-Eatonmyasthenic syndrome — in 1956.Neuro nowFrom its humble beginnings, the Department ofNeurologic Surgery has grown to become oneof the largest in North America, with more than10,000 procedures performed by a staff of about45 neurosurgeons across all three Mayo Cliniccampuses. Similarly, neurology thrives at MayoClinic because of an intense focus on the needs ofthe patient, collaboration with other specialties,dedication to research, faculty member commitmentto education, and outstanding residency andfellowship training programs.At campuses in Arizona, Florida and Minnesota,Mayo Clinic’s top-ranked neurologists and neurosurgeons diagnose and treat more than 500conditions, including many rare or complex disorders.Neurologic services are provided to children at MayoClinic in Rochester. The departments’ scholarlyproductivity rate averages five publications per facultymember per year. The departments have 37 activebasic science labs, and their researchers have 80 NIHgrants as well as other sources of funding.
NEURO LEADERSDepartment of Neurologic Surgery enterprisechair: Fredric Meyer, M.D. (NS ’88), the AlfredUihlein Family Professor of Neurologic Surgery Rochester chair: Robert Spinner, M.D.(MDPH ’89, NS ’00), the Burton M. Onofrio,M.D. Professor of Neurosurgery Arizona chair: Bernard Bendok, M.D.(NS ’15), a William J. and Charles H. MayoProfessor Florida chair: Alfredo Quinones-Hinojosa,M.D. (NS ’16), a William J. and Charles H.Mayo ProfessorDepartment of Neurology enterprise andRochester chair: Claudia Lucchinetti, M.D.(N ’94, NIMM ’95), a Eugene and Marcia(Clockwise from upper left) Fredric Meyer, M.D., Robert Spinner, M.D.,Bernard Bendok, M.D., and Alfredo Quinones-Hinojosa, M.D.Applebaum Professor of Neurosciences Arizona chair: Dean Wingerchuk, M.D.(I-1 ’94, N ’97, NIMM ’98) Florida chair: James Meschia, M.D. (N ’97)Department of Neuroscience Florida chair:Leonard Petrucelli, Ph.D. (NSCI ’03), theRalph B. and Ruth K. Abrams ProfessorLeonard Petrucelli, Ph.D.See page 24 for neurosciences story.Dean Wingerchuk, M.D., Claudia Lucchinetti, M.D.,and James Meschia, M.D.ISSUE 220185
Mayo Clinic’s neuro programsSpine 50,000 spine patients per year Informatics and electrophysiologic diagnostictools to select patients who will benefit fromsurgical interventions Advanced preoperative imaging combined withminimally invasive approaches enhance planning,surgical safety and outcomesBrain and central nervous system tumors One of highest patient caseloads in U.S.; 3,000 adult cases per year in highly integrated braintumor clinics Research leader in advanced imaging (FDOPAPET and 7-Tesla MRI), molecular diagnostics,and biologic therapies including pioneeringexperimental trials for vaccines that engage theimmune system Surgery significantly less likely to result inmortality than anywhere else in U.S.; enterprisesurvival rate for brain tumors 200 percent abovenational averageCerebrovascular diseases Leader in diagnostic and therapeutic managementof cerebrovascular disease including CT perfusion,advanced brain MRI, diffusion- and perfusionweighted MRI, MRA, carotid plaque imaging,transcranial Doppler, intracranial vessel wallimaging and genetics Leader in advanced endovascular interventions,radiation therapy and surgery for cerebrovasculardisease with 1,000 procedures annually Certified comprehensive stroke centers in Minnesotaand Florida; primary stroke center in Arizona Telestroke network of 30 hospitals in sixstates served by 17 physicians who respond toemergencies in minutes via robotic technologyEpilepsy (page 16) 700 procedures per year including vagus nervestimulation, responsive neurostimulation, deep brainstimulation, resection, laser ablation and chronicsub-threshold stimulation (not available elsewhere) All three campuses rated as Level 4 epilepsy centers6MAYO CLINIC ALUMNIWorld-leading neuroimmunology lab fordiagnosis and treatment of autoimmune epilepsysyndromes, with multiple clinical trials includingcannabidiol studies and fenfluramine study forDravet syndrome World-class imaging including first clinicallyavailable 7-Tesla MRI in North America todetect previously unidentified structural brainabnormalities as source of epilepsy
Headache/migraine Cutting-edge integrated translational researchincluding basic science, imaging science and drug/device/biologics development, and largest registryand biobank for migraine research Discovery of genetic, brain imaging, blood andclinical biomarkers to facilitate accurate diagnosisand identify predictors of response to treatment,risk factors for progression and remission, andfactors that predict risk of adverse outcomes andside effects to medications Identification of markers to distinguish posttraumatic headache from other headachedisorders, novel treatment options for posttraumatic headache, and one of country’s onlymultidisciplinary pain rehabilitation clinicsMultiple sclerosis and autoimmune neurology(page 20) Highly experienced clinicians for accuratediagnosis; cutting-edge, individualized treatmentand differentiating from mimickers of MS; highestquality MRI, neuroradiologic interpretation andexpert neuro-ophthalmology Clinicians highly regarded in diagnosis andtreatment of autoimmune neurologic diseasesincluding optic neuritis, encephalitis, dementia,epilepsy, movement disorders, transverse myelitisand dysautonomia Mayo Clinic Neuroimmunology Laboratory toevaluate patients suspected to have neuromyelitisoptica or other autoimmune neurologic diseasesPeripheral neuropathy and nerve pain Electromyography, autonomic reflex testing,thermoregulatory sweat testing, quantitativesensory testing; peripheral nerve, root andfascicular biopsies; peripheral nerve pathology lab;skin biopsy for epidermal nerve fiber testing; andgenetic testing One of largest peripheral nerve pathology labs inthe world; advanced techniques including teasedfiber analysis Electromyography and autonomic labs withadvanced methods to evaluate large and smallfiber peripheral neuropathiesISSUE 220187
ALEJANDRO RABINSTEIN, M.D.8MAYO CLINIC ALUMNI
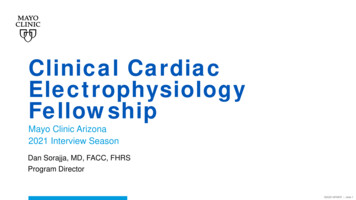
DEEP SPACE MEDICINERESEARCH PROGRAMSHOOTS TO FACILITATE MISSIONS TO MARS AND IMPROVE HEALTH ON EARTHAfull year before Alejandro Rabinstein, M.D. (CCMN ’02),was born in Cordoba, Argentina, Apollo 11 made the firstsuccessful landing on the moon and U.S. astronaut NeilArmstrong became the first person to set foot on another planet.That was the summer of 1969. Forty-eight years later, Dr. Rabinsteinhas become Mayo Clinic’s expert on deep space travel medicine — arole he never anticipated.“I wasn’t interested in space as a kid, and I’m not a sci-fi buff,”says Dr. Rabinstein, a consultant in the Department of Neurologyat Mayo Clinic in Rochester. “I am, however, intellectually curious.I have the mindset of a clinician. I believe deep space medicinecan be transformative and transcendent and can only enrich ourknowledge about Earthbound human health. While I understandthe allure of space travel, my fascination isn’t with the stars. Rather,my hope is that this work will spill over into patient care.”Dr. Rabinstein is the energy behind Mayo Clinic’s nascentdeep space medicine research program. Mayo hopes to lend itswidespread multidisciplinary expertise to the medical challengesastronauts face.On long space flights, astronauts experience health-relatedproblems including visual and sleep disturbances, a vertical brainshift, a narrowing of the central sulcus, behavioral problems andradiation exposure. So when NASA sends humans hurtling on ayearlong mission into deep space in the 2020s to test readiness forMars and, ultimately, on a three-year round trip to Mars in the2030s, what can space travelers expect? Based on experience withastronauts, experts expect Mars travelers will undergo physiologicchanges due to microgravity and ionizing radiation duringprolonged space travel.ISSUE 220189
“I believe deep space medicinecan be transformative andtranscendent and can onlyenrich our knowledge aboutEarthbound human health.”– Alejandro Rabinstein, M.D.Specifically, these changes may include: Intracranial hypertension and visual impairment Sleep disturbances Vestibular dysfunction Orthostatic intolerance Decompressive sickness Behavioral changes Burnout Reduced aerobic capacity Reduced muscle mass Inadequate nutrition Bone loss and fractures Intervertebral disc damage Cardiac rhythm problems Renal stone formation Radiation exposure — acute radiation sickness,carcinogenesis, cataracts, cardiac damage,delayed degeneration of other organs/tissues,impaired wound healing, infertility, DNAdamage and inheritable disorders, deleteriouseffects on nutrients and medications Altered immune response Host-microorganism interactions Pharmacokinetic changesWhat can medical science do to prevent, ameliorateand treat these myriad anticipated problems?Mayo Clinic hopes to collaborate with federalentities, industry, space travel and flight operationsafety experts, and physicists to solve the medicalchallenges of space missions and, equally important,make discoveries that are useful for clinicalapplications in patient care. To aid in this effort,Mayo is bringing together team members fromneurology, neurosurgery, neuro-ophthalmology,neuroradiology, neuro-otology, sleep medicine,10MAYO CLINIC ALUMNIpsychology, psychiatry, cardiology, pulmonology,physiatry, radiology, oncology, genetics, nutrition,endocrinology, nephrology, pharmacy, physiology,biomedical engineering, telemedicine and research.Mayo anticipates the major themes of its researchwill be: Discovery science aimed at understanding howmicrogravity, ionizing radiation and prolongedspace travel adversely affect organ physiology On-Earth models to explore the complex physiologic and psychologic effects of space travel Technologic innovations for physiologicmonitoringFiguring out the unknownsDr. Rabinstein was thrust into the lead on MayoClinic’s deep space medicine research effortsbecause of his involvement with NASA on anotherendeavor. SpaceWorks, an aerospace engineeringfirm and vendor to NASA, took note of his wellpublished research in therapeutic hypothermia(page 11) and enlisted his help. For several yearsDr. Rabinstein has assisted SpaceWorks on a NASAgrant to study hypothermia as a way to mediate thechallenges of deep space travel, including protectingspace travelers’ health by inducing a state ofhibernation for a portion of their trip.“Hypothermia reduces metabolic demand andputs the brain in a state of rest, which could giveastronauts a physical and psychological break,” saysDr. Rabinstein. “It’s likely this will become a part ofthe deep space travel protocols.“There’s great interest in and excitement aboutthis kind of travel. But before people venture intodeep space, they want to know that the unknownsrelated to their health have been figured out. Wehave a lot of work to do before that’s the case.Mayo Clinic has an illustrious history in aerospacemedicine during World War II, and we think wecan create a new history to help make it possiblefor humans to safely travel into deep space. Whenwe bring to bear the vast resources and mindsat Mayo Clinic, we can accomplish great things.We’re confident that includes solving the vexingphysiological and psychological challenges of deepspace travel and applying what we learn to helppatients whose feet are firmly on the ground.”
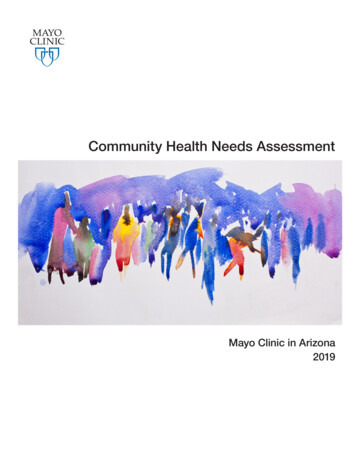
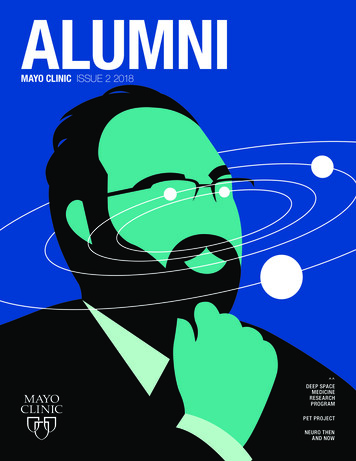
TORPOR TECHNOLOGY — INDUCING HYPOTHERMIA IN MARS-BOUND ASTRONAUTSMuch of Alejandro Rabinstein, M.D.’s, body of workinadequate nutrition to meet metabolic needs, and reduce thehas focused on clinical uses of hypothermia — a bodychances of burnout and interpersonal conflicts by promotingtemperature lower than 95 degrees. Mild therapeuticsufficient rest.hypothermia protects the brain and improves short-termneurologic recovery and survival in cardiac arrest patients.Inducing hypothermia in astronauts to minimize metabolicdemands and make travel more tolerable — calledResearchers are considering strategies to induce hypothermia. Astronauts probably would take mild sedatives toease this transition and minimize discomfort. They wouldrotate between two-weeks-long periods of hypothermiatorpor technology — is being explored as away to simplify travel to Mars and is thefocus of Dr. Rabinstein’s research withSpaceWorks.Maintaining a low bodytemperature can substantially reducemetabolic rate and facilitate rest.In addition to decreasing cerebralenergy demands, hypothermia hasbeen shown to have neuroprotectiveeffects including preservation of theand wakefulness, alternating with otherA missionto Mars will take aslong as three years:180–250 days intransit each way andapproximately500 days onMars.blood-brain barrier integrity, ameliorationwould be ensured through a gastric tube.Inducing and maintaining hypothermia in deep space presents manychallenges, including shivering. Thisnatural reaction to cold expendssignificant energy and defeats thegoal of reducing metabolic output.Also, even in a hospital setting, hypothermia presents risks when patientsare returned to a normal body temperature.of toxicity from excitatory neurotransmittersand modulation of inflammatory responses. Duringastronauts on the same mission. NutritionFor instance, fluctuating potassium levels cantrigger cardiac arrhythmia. Astronauts preparing tolong-term space missions, periods of hypothermia couldundergo this process would require careful preparation beforeprevent the occurrence of visual impairment that may resultthe mission.from vertical brain shifts and changes in the regulation of“We don’t have every facet of torpor technology for deepintracranial pressure, diminish the deleterious effects ofspace travel figured out yet,” says Dr. Rabinstein. “But we areradiation in the brain and other organs, lessen the problem ofwell on the road to paving the way to make this first step viable.” 2014 Mark Elwood / SpaceWorks Enterprises, Inc.This artist’s rendering showshow torpor technologycould be used for the transitphases of human explorationmissions to Mars.ISSUE 2201811
CREST REDUXANSWERING QUESTIONS ABOUT OPTIMAL TREATMENT FOR CAROTID DISEASEAlmost two decades ago, Mayo Clinicbegan a landmark study, CREST (CarotidRevascularization Endarterectomyversus Stenting), that changed neurology practice.Now Mayo Clinic is halfway through recruitmentfor CREST-2, a trial that’s expected to be just assignificant. Physicians who treat carotid stenosis withsurgery, minimally invasive stenting and medicationare on tenterhooks waiting for the results and hopingto answer questions including: Is medication as safe and effective as surgeryor stenting in preventing stroke caused by thebuildup of plaque in the carotid artery? Are physicians doing more harm than good withinterventions? Does surgery or stenting help cognitiveperformance in a subset of patients?Whatever the results, patients around the world willbenefit. The study’s outcome will help determine thebest treatment of asymptomatic carotid disease, whichaffects 80,000 to 100,000 people annually in the U.S.According to co-principal investigator of CREST-2James Meschia, M.D. (N ’97), Department of12MAYO CLINIC ALUMNINeurology at Mayo Clinic in Florida, Mayo is one offew centers with the infrastructure and resources toconduct these trials.“The collegial and collaborative spirit of team careacross disciplines for the betterment of the patient isfundamental to the Mayo Model of Care and is justas fundamental to a complex interventional trial likeCREST-2,” says Dr. Meschia. All three Mayo Clinicsites are involved, with specialists in neurology,neurosurgery, vascular surgery, brain and plaqueimaging, and clinical trials management.CRESTIn the later years of the first millennium, smokingwas more prevalent than it is today and statinshadn’t been introduced. Carotid endarterectomywas the most widely used invasive treatment forsignificant carotid stenosis and was considered tobe superior to medical therapy in stroke preventionof symptomatic carotid stenosis. Treatment ofasymptomatic stenosis was controversial; severaltrials found higher rates of stroke and deathassociated with carotid artery stenting.In successive years, stenting evolved.
THOMAS BROTT, M.D., AND JAMES MESCHIA, M.D.The first CREST trial was designed in the late1990s and commenced in 2000 at a time when noadequate randomized comparisons of carotidendarterectomy and carotid artery stenting existed.Mayo Clinic succeeded Rutgers University as theleader of the CREST multicenter trial to determinethe safer treatment: stenting or endarterectomy. With2,522 patients, CREST was the largest randomizedprospective study to compare carotid artery stentingand carotid endarterectomy in a patient populationsimilar to that seen in everyday practice — bothsymptomatic and asymptomatic patients. The trialwas supported by the National Institutes of HealthNational Institute of Neurological Disorders andStroke and involved 108 sites in the U.S. and Canada.Results of the trial, led by Thomas Brott, M.D. (N ’98),and Dr. Meschia, were published in 2010 and concludedthat, in general, carotid artery stenting is as good ascarotid endarterectomy for patients with carotidartery stenosis. Both procedures were shown to beequivalent in major perioperative morbidity andmortality and long-term stroke prevention, andISSUE 2201813
were good options for patients — the choice ofmanagement should be individualized.CREST was considered transformative becausethe results led directly to the FDA certifyingcarotid stenting as a safe and effective treatmentfor carotid artery stenosis, providing patients andtheir physicians with an alternative to surgery or tomedical treatment alone.“Trials such as this one form the basis for treatmentguidelines, which helps to explain why their resultsare met with anticipation and anxiety by the medicalcommunity,” says Dr. Meschia.“Regardless of the outcome of the study, whichwill determine the best treatment of carotid disease,patients win,” says Dr. Brott. “Patients at all centersin the study will receive the highest-quality medicalmanagement possible along with best practicesin surgery and stenting. CREST-2 should offer usthe definitive answer to what works best in whichpatients to treat carotid disease. We hope vascularsurgeons, neurosurgeons, interventionists andneurologists will embrace the results and focus effortson providing the very best care for every patient.”CREST-2In recent decades, medications to treat stroke riskfactors including hypertension and high cholesterolhave improved, smoking rates have declined and therate of stroke has been halved.Dr. Meschia says it’s high time for medicalmanagement of carotid artery
wise mentors in a rich research environment. Mayo excels at fostering young investigators because the Mayo environment nurtures mentoring and allows us the time to talk, teach and share. Mayo Clinic's Young Investigators Research Symposium (page 40) is a wonderful forum for young researchers across our