Transcription
Information Services DivisionScottish HeartDisease StatisticsYear ending 31 March 2018Publication date29 January 2019A National Statistics publication for Scotland
Information Services DivisionThis is a National Statistics PublicationNational Statistics status means that the official statistics meet the highest standards oftrustworthiness, quality and public value. They are identified by the quality mark shownabove.They comply with the Code of Practice for statistics and are awarded National Statisticsstatus following an assessment by the UK Statistics Authority’s regulatory arm. The Authorityconsiders whether the statistics meet the highest standards of Code compliance, includingthe value they add to public decisions and debate.Find out more about the Code of Practice -of-practice/Find out more about National Statistics -statistician/types-of-official-statistics/1
Information Services DivisionContentsIntroduction . 3Main Points . 4Results and Commentary. 5Coronary Heart Disease (CHD) . 5Heart Attacks . 12Heart Failure . 16Angina. 20Operations . 21Cardiovascular Prescribing . 25Primary Care Activity . 28Ambulance Service Activity . 28Future potential analysis . 29Glossary . 30List of Tables . 36Contact. 38Further Information . 38Rate this publication . 38Appendices . 39Appendix 1 – Background information . 39Appendix 2 – Publication Metadata . 44Appendix 3 – Early access details . 49Appendix 4 – ISD and Official Statistics . 502
Information Services DivisionIntroductionDespite a substantial reduction in the rate of death from coronary heart disease (CHD) overthe last decade, it remains one of the leading causes of death in Scotland(Health of Scotland’s population - Mortality Rates) and was the largest contributor to theoverall burden of disease in 2016 (Scottish Burden of Disease study). In 2017, there were6,727 deaths in Scotland where CHD was the underlying cause. The disease is caused whenthe heart's blood vessels, the coronary arteries, become narrowed or blocked and cannotsupply enough blood to the heart.Scotland has a high prevalence of the immediate risk factors associated with heart disease,such as smoking, obesity and high cholesterol. These immediate risk factors are influencedin turn by the conditions in which people live including access to care. Overall, it is estimatedthat around 6.4% of men and 4.0% of women are living with CHD (Scottish Health Survey2017). Treating and preventing heart disease is a national clinical priority for Scotland.1The Scottish Heart Disease Statistics publication is produced annually to provide informationon a range of different heart conditions in Scotland including: Coronary heart disease (also referred to as ischaemic heart disease, a collective termthat includes angina, heart attack and heart failure) Acute myocardial infarction (a medical term for a heart attack) Heart failure Anginaand the different types of procedures used to diagnose and treat heart disease, including; Angiography: a procedure to examine the coronary arteries Angioplasty: or percutaneous transluminal coronary angioplasty, a procedure to widennarrowed coronary arteries Coronary artery bypass graft: a procedure to replace narrowed coronary arteries withgrafts.This update contains information on incidence (the occurrence of new cases) of heartdisease, hospital activity, 30 day survival following first emergency admission, operations, GPprescribing and ambulance service activity up to the period 1 April 2017 - 31 March 2018,and mortality up to the period 1st January - 31st December 2017.Information is presented at NHS Board level with some tables (activity and mortality) alsoavailable at Local Council Area level.1Heart Disease Improvement Plan, August 20143
Information Services DivisionMain Points There has been a steady downward trend in deaths from coronary heart disease inScotland and the rest of the UK over the last ten years. In Scotland, the mortality rate fellby 35.5% between 2008 and 2017. However, the rate of decline has slowed in the lastfive years. The rate at which new cases of coronary heart disease occur (the incidence) has fallen by21.7% over the last decade, but there was a small increase in age-standardised incidencerates among both males and females between 2016/17 and 2017/18. Both incidence rates and mortality rates for heart attacks have decreased over the last 10years, although the rate of hospital discharges has increased in this period. Thepercentage of people who survived 30 days or more following their first heart attackimproved over the period 2008/09 to 2017/18 from 88% to 93%. Since 2014 there appears to have been a flattening in the rate of decline in the incidenceof heart attacks. There were small increases in rates in 2016 and 2017, with increasesslightly higher in females than males. For heart failure, incidence and mortality rates decreased over the 10 year period whilethere was a 23% increase in the hospital discharge rate, from 276 per 100,000 populationin 2008/09 to 341 in 2017/18. The 30 day survival rate improved slightly over the sameperiod.4
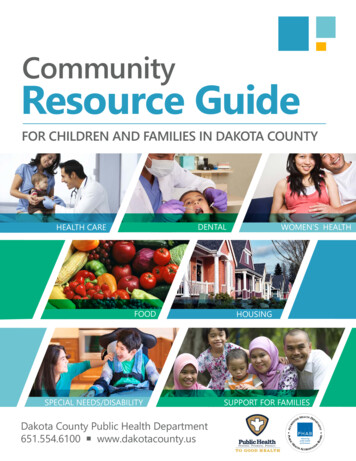
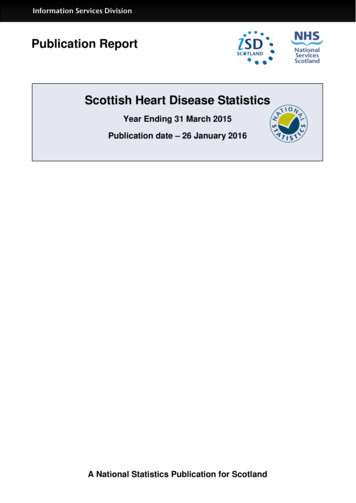
Information Services DivisionResults and CommentaryCoronary Heart Disease (CHD)CHD SummaryCHD is a collective term that includes angina, heart attack and heart failure. There was ageneral decrease in incidence, mortality and number of discharges from hospital for CHDover the last 10 years. However, there is evidence of a recent slowing in the decline ofincidence and mortality.IncidenceIncidence is the number of new cases in a defined population during a defined period of time.It reflects the risk of the disease. In the case of CHD, where incidence has been calculatedon the basis of hospital admission or death, it also reflects to some extent admission policiesand access to care. The number of new cases of CHD decreased over the past decade. Theage and sex adjusted incidence rate decreased by 21.7% from 458 per 100,000 population in2008/09 to 359 in 2017/18. There was a small increase in age-standardised incidence ratesamong both males and females between 2016/17 and 2017/18.The incidence of CHD increases sharply with age. The age and sex adjusted incidence ratefor the under 75 age group in 2017/18 was 230 per 100,000 population but for the over-75age group, it was 1,663 per 100,000 population (see Table IC1).Across all age groups presented in this publication, males were more likely than females tohave a new diagnosis of CHD. The adjusted incidence rate has fallen more for females(24.6%) over the last ten years than for males (20.1%) (Table IC1).Comparing mainland NHS Boards, in 2017/18 the adjusted incidence rate was lowest in NHSLothian (301 per 100,000 population) and highest in NHS Ayrshire & Arran (422 per 100,000population) (Table IC1).Heart disease varies greatly between areas of greater or less deprivation. In Scotland theScottish Index of Multiple Deprivation (SIMD) is used to measure area deprivation. It is ameasurement of multiple deprivation which combines information on income, employment,education, housing, health, crime and geographical access. More information is provided inthe glossary and on the Scottish Government website. For this publication, areas inScotland were divided into five equal groups (quintiles) with decreasing levels of deprivation.It can be seen from Figure 1 that all levels of deprivation show a decrease in incidence overthe last 10 years. However, the most deprived quintile shows a rate that is 76% higher at 480per 100,000 than that for the least deprived in 2017/18 (273 per 100,000). The incidence ratefor the most deprived quintile has increased slightly since 2015/16, while incidence rates inless deprived areas have continued to fall (Table DC8).5
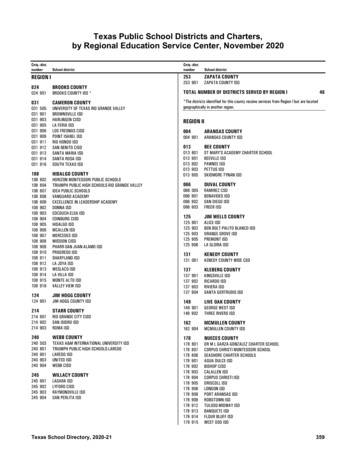
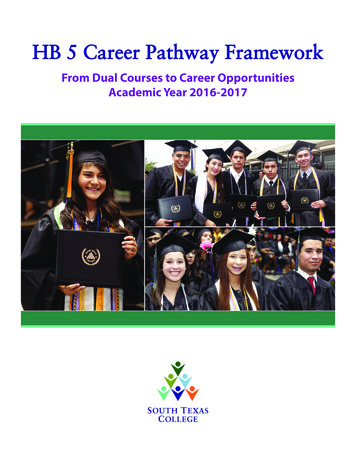
Information Services DivisionFigure 1: Coronary heart disease incidence in Scotland by deprivation quintile1Age-adjusted incidence rates per 100,000 population2Standardised Incidence rate per 100,000 population70060050040030020010002008/09 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16 2016/17 2017/18Most Deprived Quintile 1Quintile 2Quintile 3Quintile 4Least Deprived Quintile 5Notes: 1. Uses 2009, 2012 and 2016 version of SIMD, dependent on the year2. Rates are directly standardised to the 2013 European standard populationData Source: ISD SMR01 - discharges; National Records Scotland – PopulationFurther analysis of the gap in incidence rate between the most and least deprived ispresented in figure 2. This shows that, although the overall incidence rate has been fallingover time, the gap between the most and least deprived has remained fairly constant, andhas been trending upwards over the last two years for males. Over the whole periodstandardised incidence rates fell by 24% in the least deprived quintile, but by only 17% in themost deprived quintile.6
Information Services DivisionFigure 2: Gap1 in Coronary heart disease incidence in Scotland due to deprivation2Age and sex adjusted incidence rates per 100,000 population3350Gap in 112011/122012/13Female2013/142014/152015/16Both SexesNotes: 1. Calculated using the slope index of inequality method2. Uses 2009, 2012 and 2016 version of SIMD, dependent on the year3. Rates are directly standardised to the 2013 European standard populationData Source: ISD SMR01 - discharges; National Records Scotland – Population72016/172017/18
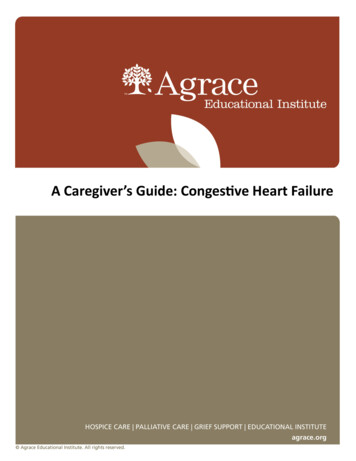
Information Services DivisionMortalityThe British Heart Foundation publishes comparisons of CHD mortality rates for the fourcountries of the UK (figure 3). The mortality rates in Scotland have been higher than England,Wales and Northern Ireland since 1985 but the absolute gap in mortality rates has narrowedover this time.Figure 3: Coronary heart disease mortality in United Kingdom, England, Wales,Scotland and Northern IrelandAge-adjusted mortality rates per 100,000 population1Age-adjusted rate per 100,000 dNorthern 619941991198719831979197519710UKNotes: 1. Rates are directly standardised to the 2013 European standard populationData Source: British Heart Foundation Cardiovascular Disease Statistics 2018,(available from ascular-disease-statistics-2017)8
Information Services DivisionIn Scotland the age and sex adjusted mortality rate for CHD fell from 214 per 100,000population in 2008 to 138 in 2017, a reduction of 35.5% over the last 10 years. The change inrate shows decreases in mortality rate each year since 2009 with the exception of 2015. Thefall in 2017 was the smallest in the preceding 10 years. (Table MC1 and figure 4).Figure 4: Coronary heart disease1: % change from previous year for all agesAge and sex adjusted mortality rates per 100,000 population2% change from previous 2011201220132014201520162017Notes: 1. Analysis uses ICD-10 codes I20-I252. Rates are directly standardised to the 2013 European standard populationData Source: National Records Scotland - Deaths and PopulationBetween 2008 and 2017 the reduction in adjusted mortality rates for CHD was higher forfemales (40.6%) than for males (32.7%). The difference in rates between men and womennarrowed from 124 deaths per 100,000 population in 2008 to 95 deaths per 100,000population in 2017.Of the mainland NHS Health Boards, NHS Lanarkshire had the highest age and sex adjustedmortality rate in 2017 (148 per 100,000 population) while NHS Borders and NHS Forth Valleyhad the lowest rates (125 per 100,000 population). NHS Forth Valley had the largestpercentage reduction in mortality rate among the mainland Health Boards between 2008 and2017 (45.5%), while NHS Ayrshire & Arran had the lowest percentage reduction in themortality rate between 2008 and 2017 (29.9%).The Scottish Government publish a report on the long-term monitoring of health inequalitiesin Scotland. The report contains data on the impact of deprivation on CHD mortality amongthose aged 45-74 years and shows that, in 2017, the CHD mortality rate was five timesgreater in Scotland’s most deprived areas compared to the least deprived in this age group.Furthermore, this gap has been increasing steadily over time. Further information can befound on the Scottish Government website.9
Information Services DivisionDischargesHospital discharge rates reflect both the occurrence of new cases and also the frequencywith which people are readmitted to hospital. It is a useful measure of the amount of NHShospital activity related to the condition. In the last decade, there was a decreasing trend inthe rate of discharges from hospital with CHD. Between 2008/09 and 2017/18, the age andsex adjusted discharge rate fell by 12.5% from 1,091 to 955 per 100,000 population. Theactual number of discharges remained fairly steady averaging at over 49,000 discharges peryear, reflecting the effect of an ageing population.The adjusted discharge rate for females was less than half that for males in 2017/18 andthere was a larger percentage decrease for males over the last decade (12.9% for malescompared to 11.5% for females).The percentage decrease in the rate was larger in the under-75 year age group (13.2%) thanin the over-75 group (11.2%).Comparing mainland NHS Boards, in 2017/18 the adjusted discharge rate was lowest in NHSLothian (574 per 100,000 population) and highest in NHS Lanarkshire (1,368 per 100,000population).There was considerable variation between NHS Boards in trends over time. Between 2008and 2017 discharge rates for CHD increased by 19.7% in NHS Ayrshire & Arran and by17.3% in NHS Greater Glasgow & Clyde, while in other boards there were falls of over 35%(see Figure 5 below). Over the last five years Greater Glasgow & Clyde has continued tohave a much larger rise in CHD discharge rate than other boards.10
Information Services DivisionFigure 5: Coronary heart disease1: % change from 2008/09 to 2017/18 in dischargesfrom NHS Boards with coronary heart disease1;Age and sex adjusted mortality rates per 100,000 population2% change over 10yr period3020100-10-20-30-40-50Notes: 1. Analysis uses ICD-10 codes I20-I25.2. Rates are directly standardised to the 2013 European standard populationData Source: ISD SMR01 - discharges; National Records Scotland – population estimates.Tables AC1 and AC4 provide more detail at NHS Board and Council level.11
Information Services DivisionHeart AttacksHeart Attacks SummaryMyocardial infarction (or heart attack) is a major cardiovascular event caused by suddenobstruction to coronary arteries. The incidence and mortality rates for heart attacks havedecreased over the last 10 years although the rate of discharges have increased in thisperiod. Furthermore, the percentage of people who survived 30 days or more following theirfirst emergency admission to hospital with a heart attack improved over the period 2008/09 to2017/18.IncidenceThe age and sex adjusted incidence rate for heart attacks (the frequency of new cases)decreased by 13.0% from 259 per 100,000 population in 2008/09 to 225 in 2017/18 (TableIC2 and figure 6). The incidence rate increased slightly between 2007/08 and 2010/11. Aspreviously noted, this is likely to be due to the introduction of more sensitive tests fordiagnosis (see Appendix A1 for more information).Figure 6: Heart attack1 Age and sex adjusted incidence rates per 100,000 population2Incidence rate per 100,000 16Both sexesNotes: 1. Analysis uses ICD-10 codes I21-I222. Rates are directly standardised to the 2013 European standard population.P. Data are provisional for 2017/18 and are subject to change in future analyses.Data Source: ISD SMR01 - discharges; National Records Scotland – Population122016/172017/18P
Information Services DivisionMortalityThe age and sex adjusted mortality rate for heart attacks decreased substantially over thelast ten years, falling by 34.7% from 121 per 100,000 population in 2008 to 79 in 2017 (TableMC1 and figure 7).Figure 7: Heart attacks1: all ages by sexAge and sex adjusted mortality rates per 100,000 population2180Mortality rate per 100,000 es2012Females20132014201520162017Both SexesNotes: 1. Analysis uses ICD-10 codes I21-I222. Rates are directly standardised to the 2013 European standard populationData Source: National Records Scotland - Deaths and PopulationSince 2014 there appears to have been a flattening in the rate of decline in the incidence ofheart attacks. There were small increases in rates in 2016 and 2017, with increases slightlyhigher in females than males.13
Information Services DivisionDischargesOver the last 10 years the age and sex adjusted rate for hospital discharges with heart attackhas increased by 15.9% from 425 per 100,000 population in 2008/09 to 493 per 100,000population in 2017/18. More recently the number of discharges has remained relativelystable, with a decrease in the latest year of 5.8% (Table AC1 and Figure 8).Figure 8: Discharges from hospital with a diagnosis of heart attack1;Age and sex adjusted discharge rates per 100,000 population2Discharge rate per 100,000 /162016/172017/18pBoth SexesNotes: 1. Analysis uses ICD-10 codes I21-I22.2. Rates are directly standardised to the 2013 European standard populationP. Data are provisional for 2017/18 and are subject to change in future analyses.Data Source: ISD SMR01 - discharges; National Records Scotland – population estimates.The increase in the number of discharges from hospital with a diagnosis of heart attack since2008/09 was likely to be due to a change in the way that heart attacks are diagnosed. Themore sensitive troponin blood test is now routinely used to diagnose heart attacks. Thismeans that some cases that might previously have been diagnosed as angina or anothersimilar condition may now be classified as a heart attack. It is not possible to calculate thenumber of additional cases diagnosed because of the use of the troponin test. Moreinformation on this test is provided in the background information in Appendix A1.SurvivalThe percentage of people who survived 30 days or more following their first emergencyadmission to hospital with a heart attack improved over the period 2008/09 to 2017/18(Figure 13). The percentage who survived 30 days for both sexes combined increased from14
Information Services Division88% in 2008/09 to 93% in 2017/18 (Table S1 and Figure 9). Although there has been noincrease over the last two years. Over the same period, there was a narrowing of the gap inthe survival between males and females from 7.1 to 2.9 percentage points.For those aged 75 and over, 30 day survival increased from 76.6% in 2008/09 to 84.4% in2017/18, although again there has been no increase over the last two years.Figure 9: Heart attack1;Percentage of patients surviving 30 days or more after first emergency admission210030 day survival th SexesNotes: 1. Analysis uses ICD-10 codes I21-I222. y-axis (percentage surviving 30 days) starts at 70% to enable clear comparison between sexes.P. Data are provisional for 2017/18 and are subject to change in future analyses.Data Source: ISD SMR01 - discharges; National Records Scotland – Population15
Information Services DivisionHeart FailureHeart Failure SummaryHeart failure occurs when the heart cannot provide sufficient pump action to meet demand.The incidence and mortality rates decreased over the 10 year period while there was anincrease in the discharge rate. The 30 day survival rate shows a slight increase over thesame period.Heart failure can be subdivided into two different types depending on what proportion ofblood the heart is able to pump out - the ejection fraction (EF). Heart failure can bediagnosed either with preserved EF - where this is within the normal range - or reduced EF.There is work underway to improve the clinical coding of the ejection fraction. Once thecoding is of a sufficient standard, information on ejection fraction will be included within thisreport.IncidenceThe age and sex adjusted incidence rate for heart failure decreased by 15.2% from 120 per100,000 population in 2008/09 to 102 in 2017/18 (Figure 10). The rate fell each year from2008/09 to 2014/15 before seeing a small increase in the latter three years. The 65 – 74 agegroup has the highest decrease in rate over the time period with a 25.7% fall.Figure 10: Heart failure1; Age and sex adjusted incidence rates per 100,000 population2Incidence rate per 100,000 oth sexesNotes: 1. Analysis uses ICD-10 code I502. Rates are directly standardised to the 2013 European standard population.P. Data are provisional for 2017/18 and are subject to change in future analyses.Data Source: ISD SMR01 - discharges; National Records Scotland – Population162016/172017/18P
Information Services DivisionMortalityThe age and sex adjusted mortality rate for heart failure decreased substantially over the lastten years, falling by 53.4% from 13 per 100,000 population in 2008 to 6 in 2017 (figure 11).Figure 11: Heart failure1: all ages by sexAge and sex adjusted mortality rates per 100,000 population2Mortality rate per 100,000 males20132014201520162017Both SexesNotes: 1. Analysis uses ICD-10 code I502. Rates are directly standardised to the 2013 European standard populationData Source: National Records Scotland - Deaths and PopulationDischargesThe age and sex adjusted discharge rate increased by 23.3%, from 276 per 100,000population in 2008/09 to 341 in 2017/18. The increase in the actual number of dischargesover the last ten years can be seen here. (Figure 12 and Table AC1).17
Information Services DivisionFigure 12: Number of discharges from hospital with a diagnosis of heart failure1;18000Number of 8/09 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16 2016/17 2017/18Both SexesNotes: 1. Analysis uses ICD-10 codes I50.Data Source: ISD SMR01 - discharges; National Records Scotland – population estimates.SurvivalIn the last ten years, there was a small increase in the number of people surviving 30 daysfollowing a first emergency admission to hospital for heart failure. The percentage surviving30 days increased from 86% to 87% during that time (Table S3 and figure 13). For thoseaged 75 and over, the percentage surviving 30 days increased from 82.5% to 84.5% over thesame period.18
Information Services DivisionFigure 13: Heart failure1;Percentage of patients surviving 30 days or more after first emergency admission210030 day survival rate959085802008/09 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16 2016/17 2017/18MalesFemalesBoth SexesNotes: 1. Analysis uses ICD-10 codes I502. y-axis (percentage surviving 30 days) starts at 80% to enable clearer comparison between sexes.P. Data are provisional for 2017/18 and are subject to change in future analyses.Data Source: ISD SMR01 - discharges; National Records Scotland – Population19
Information Services DivisionAnginaAngina SummaryAngina is chest pain on exertion as a result of CHD. There was a downward trend in thedischarge rate from 2008/09 to 2017/18, but little change in the percentage of peoplesurviving 30 days following admission to hospital.DischargesIn the period 2008/09 to 2017/18, there was a general downward trend in the adjusteddischarge rate for angina. The age and sex adjusted discharge rate was 278 per 100,000population in 2008/09 falling to 122 in 2017/18, a decrease of 56.1% (Figure 14).Figure 14: Discharges from hospital with a diagnosis of angina1;Age and sex adjusted discharge rates per 100,000 population2Discharge rate per 100,000 162016/172017/18pBoth SexesNotes: 1. Analysis uses ICD-10 code I20.2. Rates are directly standardised to the 2013 European standard populationP. Data are provisional for 2017/18 and are subject to change in future analyses.Data Source: ISD SMR01 - discharges; National Records Scotland – population estimates.Tables AC1 and AC4 provide more detail at NHS board and Council level.SurvivalIn the last ten years, the percentage of people surviving 30 days following a first emergencyadmission to hospital for angina has remained around the 98 to 99 mark.20
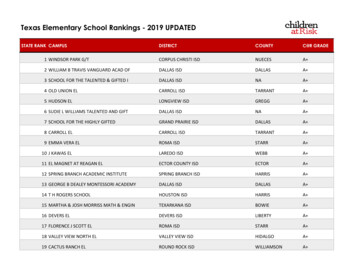
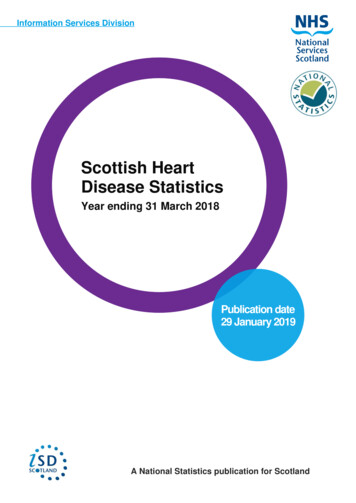
Information Services DivisionOperationsIn CHD, the blood supply to the heart is reduced or blocked. Two types of operation are usedto improve the flow of blood to the heart. These are Coronary Artery Bypass Grafts (CABG)and angioplasties (Percutaneous Transluminal Coronary Angioplasty - PTCA).A CABG is an operation in which a blood vessel from another part of the body or a syntheticgraft is grafted to the coronary artery or arteries, to bypass narrowed sections and restoreblood flow to the heart muscle. This involves a general anaesthetic and major open surgery.An angioplasty involves passing a thin, hollow tube into the coronary arteries from an arteryin the groin or arm. A device on the tube is then used to unblock the artery, and stretch theartery walls so that blood and oxygen can flow to the heart muscle. A small tube (or stent)may be left inside the vessel to ensure that it stays open. An angioplasty has the advantagethat it is generally regarded as a less major procedure than a CABG.Details of hospital activity for CABG, angioplasty, angiography and valve surgery by age,gender, type of admission and NHS board are given in Table OC1.Coronary Artery Bypass GraftsOver the last decade there was a decrease in the number of CABG operations. The age andsex adjusted hospital discharge rate decreased from 45 per 100,000 population in 2008/09 to27 per 100,000 population in 2017/18, a reduction of 39.6% (Table OC1).AngioplastiesThe general downward trend in the number of CABG operations reflects the increasing use ofangioplasties in the treatment of CHD. The age and sex adjusted hospital discharge rate forangioplasties increased from 135 per 100,000 population in 2008/09 to 161 in 2017/18, anincrease of 19.4% (Table OC1).CABG and angioplasty are collectively known as revascularisation procedures. The age andsex adjusted hospital discharge rate for revascularisation procedures as a whole increasedslightly over the last 10 years from 180 per 100,000 population in 2008/09 to 188 in 2017/18,an increase of 4.6% (Table OC1 and figure 15). However, this slight increase should be setin the context of the marked fall in CHD incidence shown in figure 1.21
Information Services DivisionDischarge rate per 100,000 populationFigure 15: Revascularisation1Age and sex adjusted incidence rates per 100,000 2016/172017/18pBoth SexesNotes: 1. Analysis uses OPCS codes K40-K46 (main A position only); K49, K50, K75 (any A position)2. Rates are directly standardised to the 2013 European standard populationP. Data are provisional for 2017/18 and are subject to change in future analyses
Treating and preventing heart disease is a national clinical priority for Scotland. 1. The Scottish Heart Disease Statistics publication is produced annually to provide information on a range of different heart conditions in Scotland including: Coronary heart disease (also referred to as ischaemic heart disease, a collective term