Transcription
Coding Clinic UpdateJames S. Kennedy, MD, CCS, CDIP, CCDSPresidentCDIMD – Physician ChampionsThisis the Full Title of a SessionSmyrna, TennesseeAdditional slides added July 31, 20181
PresenterJames S. Kennedy, MD, CCS, CDIPPresident – CDIMD (near Nashville, TN)Credentials: Internal medicine – the University of Tennessee AHIMA CCS – 2001 AHIMA CDIP – 2012Contact: jkennedy@cdimd.com (615) 479-70212
Learning Objectives At the completion of this educational activity, thelearner will be able to:– Provide an overview on structure of ICD-10-CM/PCS codingconventions, guidelines, and official advice essential tounderstanding Coding Clinic advice– Outline the history, authority, and utility of the Coding Clinicfor ICD-10-CM/PCS in promoting documentation and codingcompliance– Explore recent Coding Clinic advice and concepts affectingCDI practice– Develop strategies that engages Coding Clinic to help ussolve challenges with ICD-103
Foundations of Coding Clinic4
The AHA Central OfficeOrigins and Goals Created through a written Memorandum of Understanding betweenthe American Hospital Association (AHA) and the National Center forHealth Statistics (NCHS) in 1963 to:– Serve as the U.S. clearinghouse for issues related to the use of ICD-10CM/PCS– Work with NCHS, the Centers for Medicare & Medicaid Services (CMS),and AHIMA (American Health Information Management Association)—known as the Cooperating Parties—to maintain the integrity of theclassification system– Recommend revisions and modifications to the current and futurerevisions of the ICD– Develop educational material and programs on ICD-10-CM/PCS5
The AHA Central OfficeCoding Clinic for ICD-10-CM/PCS In concert with Cooperating Parties, publishes the CodingClinic for ICD-10-CM/PCS– CMS' affirmation of the Coding Clinic as the official source of codinginformation is noted in the Federal Register, Vol. 74, No. 165, Thursday,August 27, 2009 - https://tinyurl.com/ybxeq78h– Most advice published in Coding Clinic has been vetted by theirEditorial Advisory Board– No advice can be published unless unanimously agreed upon bythe four Cooperating Parties In essence, the Supreme Court in coding issues– Used by the Department of Justice and HHS OIG in judging codingcompliance Coding Clinic (CC), 1st Quarter 2011, p. 19Changes in the ICD-9-CM classification supersede previouslypublished Coding Clinic advice6
Obtaining Coding Clinic AdviceSubscribing Subscriptions available:AHA– Paper– Electronic– On many encoders (e.g. 3M,TruCode, Optum, Nuance)Coding Clinic for ICD-10-CMA quarterly publication of theCentral Office on ICD-9-CM.Get your own subscription at:http://www.codingclinicadvisor.com7
Send Your Own Questions toCoding Clinic AdvisorAnyone can send in questions and do it online– They are now accepting ICD-10 questionshttp://www.codingclinicadvisor.comIt’s FREE!8
Foundations – Coding 1019
DiagnosesICD-10-CM Hierarchy1. ICD-10-CM Index to Diseases The term must be looked up here first2. ICD-10-CM Table of Diseases– Offers additional instructions, such as “code first”, “code inaddition”, “in diseases classified elsewhere”, “Excludes1”,“Excludes2”, and others3. ICD-10-CM Official Guidelines for Coding andReporting‒May add or subtract codes or influence sequencing4. Advice from the Coding Clinic for ICD-10-CM/PCS‒‒May add or subtract codes or influence sequencingOccasionally can overrule the Index, Table, and Guidelines5. Court opinions or other payer-specific regulations10
How to Look Up a Diagnosis CodeChronic Kidney DiseaseDiseaseIndexTableEssential to use both the Index (first) and then the Table when looking up a code!11
Exception to the RulePatient presents with ascites due to cirrhosis due toHepatitis CK71.51 Toxic liver disease with chronicactive hepatitis with ascitesAssign codes B18.2, Chronic viral hepatitis C, K74.60, Unspecified cirrhosis ofliver, and R18.8, Other ascites, to capturethese conditions.Coding Clinic, 1st Quarter, 2018, pages 4-512
Exception to the Rule Although the Index entries for these conditions maybe confusing, a basic rule of coding is that furtherresearch/review may be required, if the code indexeddoes not identify the condition correctly. While the ascites is due to the cirrhosis, and thecirrhosis is due to the chronic viral hepatitis C (HCV),ascites is not always present with these conditions, so itis appropriate to convey the full clinical picture andassign an additional code for the ascites.– Essence of what’s integral and what’s not w/symptom codesCoding Clinic, 1st Quarter, 2018, pages 4-513
DiagnosesICD-10-CM Official Guidelines An essential reference that must be read over and over andover again. Available for free at: http://www.tinyurl.com/2019ICD10CMguidelines14
2018 ICD-10-CM Official GuidelinesExcludes1 Note Excludes1 A type 1 Excludes note is a pure excludesnote. It means “NOT CODED HERE!”– An Excludes1 note indicates that the code excluded shouldnever be used at the same time as the code above theExcludes1 note. An Excludes1 is used when two conditionscannot occur together, such as a congenital form versus anacquired form of the same condition. An exception to the Excludes1 definition is thecircumstance when the two conditions are unrelatedto each other. If it is not clear whether the twoconditions involving an Excludes1 note are related ornot, query the provider.15
16
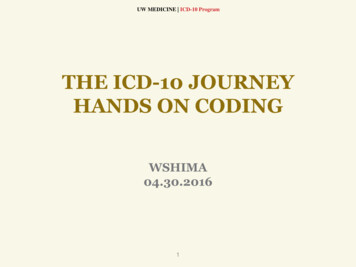
Chapter 16 Excludes2 NotesIncludes E00-E88, Endocrine/Nutritional/Met. Diseases17
Personal Opinion of Dr. Kennedy - Not Necessarily Mayo PolicyNotice the conflict between these Excludes1 and Excludes2 notes18
Coding Clinic 2nd Q 2018, p.6Neonatal Sodium Disorders Question: Please clarify the appropriate code assignmentfor an infant in the perinatal period, who develops eitherhyponatremia or hypernatremia.– There is an Excludes2 note at the beginning of Chapter 16, Certainconditions originating in the Perinatal Period (P00-P96), indicatingthese codes can be assigned with a code from Chapter 4,Endocrine, nutritional and metabolic disease (E00-E89).– However, at the beginning of Chapter 4 there is an Excludes1 notethat does not allow assigning codes in categories E00-E89 withcodes in categories P70-P74. Based on these conflicting Excludes notes, would codeP74.2, Disturbances of sodium balance of newborn, beassigned with either code E87.0, Hyperosmolality andhypernatremia, or code E87.1, Hypo-osmolality andhyponatremia, to further specify the condition?19
Personal Opinion of Dr. Kennedy - Not Necessarily Mayo PolicyCoding Clinic 2nd Q 2018, p.6Neonatal Sodium Disorders Answer: Assign only code P74.2, Disturbances ofsodium balance of newborn, when the newborn isdiagnosed with a disturbance of sodium balance, suchas hypernatremia or hyponatremia.Take home lessons If there are conflicting Excludes1 and Excludes2 notes,the Excludes1 note trumps the Excludes2 note20
New ICD-10-CM CodesEffective October 1, 201821
2018 ICD-10-CM Official GuidelinesThe word “With” or “In” “With” The word “with” or “in” should be interpreted tomean “associated with” or “due to” when it appears in acode title, the Alphabetic Index, or an instructional note inthe Tabular List.– The classification presumes a causal relationship between the twoconditions linked by these terms in the Alphabetic Index orTabular List.– These conditions should be coded as related even in the absenceof provider documentation explicitly linking them, unless thedocumentation clearly states the conditions are unrelated orwhen another guideline exists that specifically requires adocumented linkage between two conditions (e.g., sepsisguideline for “acute organ dysfunction that is not clearlyassociated with the sepsis”).22
Sepsis “with” organ dysfunctionIndex and Table say that sepsis and organ dysfunctionare automatically linkedThe Guidelines state: An acute organ dysfunction must be associatedwith the sepsis in order to assign the severe sepsis code.If the documentation is not clear as to whether an acute organdysfunction is related to the sepsis or another medical condition, querythe provider.23
ProceduresICD-10-PCS Hierarchy1. ICD-10-PCS Index–The purpose of the alphabetic index is to locate the appropriatetable that contains all information necessary to construct aprocedure code. The PCS Tables should always be consulted tofind the most appropriate valid code.2. ICD-10-PCS Table–It is not required to consult the index first before proceeding tothe tables to complete the code. A valid code may be chosendirectly from the tables.3. ICD-10-PCS Official Guidelines for Coding and Reporting‒May add or subtract codes or influence sequencing4. Advice from the Coding Clinic for ICD-10-CM/PCS‒‒May add or subtract codes or influence sequencingSometimes can overrule the Index, Table, and Guidelines5. Court opinions or other payer-specific regulations24
ICD-10-PCS Root OperationFusionFusion: Joining together portions of an articular bodypart rendering the articular body part immobile25
Spinal FusionCC, 2nd Quarter, 2017, pages 23-24The health record documentation states that the patientunderwent laminectomy C3 through C7, decompression ofthe spinal cord, placement of posterior instrumentation andspinal fusion, due to cervical spondylosis.– After decompression of the spinal cord, lateral mass screws wereplaced from C3-C6 bilaterally with connecting rods.Questions: Would placement of instrumentation be coded as a pediclebased stabilization device? What device value is assigned for the spinal fusion? Would the decompression of the spinal cord be codedseparately or is it considered inherent to the total surgery?26
Spinal FusionCC, 2nd Quarter, 2017, pages 23-24 In this case, a spinal fusion was not carried out.– There was no documentation of bone graft or a bone graftsubstitute being utilized; only spinal cord decompression andinsertion of rods and screws (instrumentation) wereaccomplished. Instrumentation alone does not constitute a spinal fusion.– Spinal fusion involves the use of bone graft or bone graftsubstitute, which can be done with or without instrumentation. Further, the insertion of rods and screws is not the same asthe placement of a pedicle based stabilization device.27
Spinal FusionCC, 1st Quarter, 2018, pages 23-24 Question: This advice of CC 2017, 2nd Quarter,appears to conflict with the root operationexplanation, which states, “The body part is joinedtogether by fixation device, bone graft, or othermeans.” Could you provide an explanation? Answer: The previously published advice is accurate.– There is no discrepancy in the case of spinal fusion, becausethere is a specific guideline for spinal fusion that goesbeyond the basic root operation definition of “Fusion.”– While the root operation of “fusion” does not require theuse of bone graft, the spinal fusion guideline indicates that aspinal fusion requires bone graft.28
2018 and 2019 ICD-10-PCS Official Guidelines29
2018 and 2019 ICD-10-PCS Official Guidelines30
Questions Sent To Coding ClinicAbout ICD-10-PCS Guidelines31
Spinal Fusion Procedure CodesDeleted Due To Lack of Device RG13Z0Code DescriptionFusion of Occipital-cervical Joint, Anterior Approach, Anterior Column, Open ApproachFusion of Occipital-cervical Joint, Posterior Approach, Posterior Column, Open ApproachFusion of Occipital-cervical Joint, Posterior Approach, Anterior Column, Open ApproachFusion of Occipital-cervical Joint, Anterior Approach, Anterior Column, Percutaneous ApproachFusion of Occipital-cervical Joint, Posterior Approach, Posterior Column, Percutaneous ApproachFusion of Occipital-cervical Joint, Posterior Approach, Anterior Column, Percutaneous ApproachFusion of Occipital-cervical Joint, Anterior Approach, Anterior Column, Percutaneous EndoscopicApproachFusion of Occipital-cervical Joint, Posterior Approach, Posterior Column, PercutaneousEndoscopic ApproachFusion of Occipital-cervical Joint, Posterior Approach, Anterior Column, Percutaneous EndoscopicApproachFusion of Cervical Vertebral Joint, Anterior Approach, Anterior Column, Open ApproachFusion of Cervical Vertebral Joint, Posterior Approach, Posterior Column, Open ApproachFusion of Cervical Vertebral Joint, Posterior Approach, Anterior Column, Open ApproachFusion of Cervical Vertebral Joint, Anterior Approach, Anterior Column, Percutaneous Approach32
High Prevalence ofInvalid Spinal Fusion CodesGiven Coding Clinic’s and Medicare’s emphasis on spinalfusions, the speaker believes that inpatient codingpractices for spinal fusions must be addressed,particularly regarding the use of bone grafting33
Coding RulesCDI Lessons Learn how to use theIndex, Table, Guidelines,and Coding Clinic advice– Great bridge buildersbetween CDI teams andcoders Coding Clinic is availableto all invested indocumentation integrity– Must be advocated in lightof the patient’s clinicalindicators, the provider’sdocumentation, andofficial coding rulesPhoto credit: Wikipediahttp://en.wikipedia.org/wiki/Bridge34
COPD and Asthma35
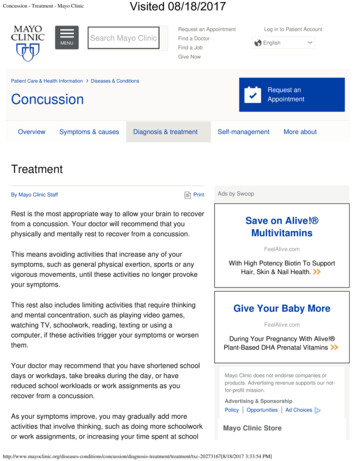
COPD – Asthma Overlap d-overlap-syndrome/Permission given to reproduce this graphic.36
Key Clinical Indicators Approximately 20% of patients with COPD have asthma asan overlap– Onset after age 40, but may have had symptoms in childhood COPD symptoms– Airflow limitations not fully reversible between exacerbations– Hyperinflation on CXR Asthma symptoms– Usually childhood symptoms, MD-diagnosed asthma, history ofallergies or noxious exposures– Significant improvement with treatment– Eosinophils in sputumGibson PG, McDonald VM. Asthma–COPD overlap 2015: now we are six. Thorax 2015;70:683-691.37
Coding Clinic, 1st Quarter, 2017, page 25 Paraphrased question – If someone has COPD andasthma together, should only the COPD code beassigned? Paraphrased answer – If no asthma specificity isdocumented, then only code the COPD code. If aspecified form of asthma is documented, then codethe specified form of asthma. Options include: Mild intermittentMild persistentModerate persistentSevere persistent38
J44 – Code Also Note for AsthmaThe key phrase is “type of asthma”Unspecified asthma is not a “type of asthma”39
Exacerbated Asthma with COPD Coding Clinic, 1st Quarter, 2017 Page: 26– Exacerbation of COPD does not necessary mean that anycoexisting asthma is also exacerbated Requires documentation that both are exacerbated atthe same time. Coding Clinic, 4th Quarter, 2017, pp. 96-97– While exacerbated asthma is not a “type” of asthma, it doesadd additional information about the type of asthma. As such, if exacerbated asthma coexists with COPD, itmay be coded without the specified type40
DRG ImpactMS-DRGAPR-DRGExacerbated COPDAsthmaMS-DRG 192COPD w/o CC/MCC0.7265APR DRG 140COPDSOI 1 (0.493) ROM 1Exacerbated COPDA specified type of asthma(e.g. mild intermittent)MS-DRG 192COPD w/o CC/MCC0.7265APR DRG 140COPDSOI 1 (0.493) ROM 1Exacerbated COPD (PDx)Exacerbated AsthmaMS-DRG 191COPD w/CC0.9176APR DRG 140COPDSOI 2 (0.6227) ROM 1Exacerbated COPD (PDx)Exacerbated specific typeof asthmaMS-DRG 191COPD w/CC0.9176APR DRG 140COPDSOI 2 (0.6227) ROM 1Exacerbated Asthma (PDx)Exacerbated COPDMS-DRG 202Asthma w/CC/MCC0.9260APR DRG 141AsthmaSOI 2 (0.5467) ROM 141
Exacerbation of COPDin the Setting of EmphysemaDisease-pulmonary -see also Disease, lung- - artery I28.9- chronic obstructive J44.9- - with- - - acute bronchitis J44.0- - - exacerbation (acute) J44.1- - - lower respiratory infection (acute) J44.0- - decompensated J44.1- - - - with- - - exacerbation (acute) J44.1Emphysema (atrophic) (bullous)(chronic) (interlobular) (lung)(obstructive) (pulmonary) (senile)(vesicular) J43.9- centrilobular J43.2- panacinar J43.1- panlobular J43.1- specified NEC J43.8unilateral J43.0Note there is no code for“decompensated emphysema”COPD is APR-DRG SOI of 2COPD is MS-DRG CC only if decompensatedNot a CC in MS-DRGsSOI of 2 in APR-DRGs42
Can Emphysema and COPDBe Coded Together? The term, “COPD”, isan overarching termthat encompassesSmall wayfibrosisCOPD– Small airway disease– Lung destruction Emphysema refersonly to the pathologythat occurs with COPD.Others may bepresent, such as– Bronchiectasis– Pulmonary fibrosis– Others43
EXCLUDES1 NOTE: NOT CODED HERE!44
ICD-10-CM’s ApproachEXCLUDES1 NOTE: NOT CODED HERE!45
Coding Clinic, 4th Quarter, 2017, page 98 With the documentation of emphysema anddecompensated COPD, only code the emphysema code,NOT the decompensated COPD code– Coding Clinic (in my opinion, erroneously) opined thatemphysema is a subset of COPD– Consequently, J44.1 cannot be coded, losing a MS-DRG CC Suggestions:– Read the Global Initiative for Chronic Obstructive Lung Disease(GOLD) Global Strategy for the Diagnosis, Management andPrevention of COPD, available at:https://tinyurl.com/2017GOLDemphysema– Encourage physicians not to use the word “emphysema” unlessthey are absolutely sure that the patient does not have some formof obstructive bronchiolitis.– Write Coding Clinic to tell them what you think of this advice.46
Encephalopathy47
MDC 1 – EncephalopathyGlobal Disease or Dysfunction Adams and Victor Neurology, 10e - Global disturbance ofcerebral function NIH – any diffuse disease of the brain that alters brainfunction or structure.– May be caused by infectious agent (bacteria, virus, or prion),metabolic or mitochondrial dysfunction, brain tumor or increasedpressure in the skull, prolonged exposure to toxic elements(including solvents, drugs, radiation, paints, industrial chemicals,and certain metals), chronic progressive trauma, poor nutrition, orlack of oxygen or blood flow to the brain.– The hallmark of encephalopathy is an altered mental ncephalopathy.htm48
Delirium vs. Encephalopathy Delirium - Manifestation– Acute change or fluctuation inmental status and inattention,accompanied by eitherdisorganized thinking or analtered level of consciousnessArousable to VoiceAcute mentalstatus changeInattentionFluctuatingmental organizedthinkingAltered level ofconsciousnessUnarousableto VoiceCOMA Encephalopathy –Underlying Cause– Global brain dysfunction Dr. Kennedy’s personalopinion– If the global brain dysfunctioncan be explained by a namedbrain disease or itsexacerbation, then the term“encephalopathy” is integral– As such, the term“encephalopathy” is integralto defined neurodegenerativeillnesses that tend to wax andwane.49
MDC 1 – EncephalopathyMultiple Options in ICD-10-CMEncephalopathy (acute) G93.40- acute necrotizing hemorrhagicG04.30- - postimmunization G04.32- - postinfectious G04.31- - specified NEC G04.39- alcoholic G31.2- anoxic —see Damage, brain, anoxic- arteriosclerotic I67.2- centrolobar progressive (Schilder)G37.0- congenital Q07.9- degenerative, in specified disease NECG32.89- demyelinating callosal G37.1- due to- - drugs (see also Table ofDrugs and Chemicals) G92- in (due to) (with)- - birth injury P11.1- - hyperinsulinism E16.1 [G94]- - influenza —see Influenza, with,encephalopathy- - lack of vitamin (see alsoDeficiency, vitamin) E56.9 [G32.89]- - neoplastic disease (see alsoNeoplasm) D49.9 [G13.1]- - serum (see also Reaction, serum)T80.69- - syphilis A52.17- - trauma (postconcussional) F07.81- - - current injury —see Injury,intracranial- - vaccination G04.02- lead —see Poisoning, lead- metabolic G93.41- hepatic —see Failure, hepatic- hyperbilirubinemic, newborn P57.9- - drug induced G92- - due to isoimmunization (conditions- - toxic G92in P55) P57.0- myoclonic, early, symptomatic —- hypertensive I67.4see Epilepsy, generalized, specified- hypoglycemic E16.2NEC- hypoxic —see Damage, brain, anoxic- hypoxic ischemic P91.60- - mild P91.61- - moderate P91.62(Acute) Encephalopathy is unspecified- - severe P91.63- necrotizing, subacute (Leigh) G31.82- pellagrous E52 [G32.89]- portosystemic —see Failure, hepatic- postcontusional F07.81- - current injury —see Injury,intracranial, diffuse- posthypoglycemic (coma) E16.1[G94]- postradiation G93.89- saturnine —see Poisoning, lead- septic G93.41- specified NEC G93.49- spongioform, subacute (viral) A81.09- toxic G92- - metabolic G92- traumatic (postconcussional) F07.81- - current injury —see Injury,intracranial- vitamin B deficiency NEC E53.9[G32.89]- - vitamin B1 E51.2- Wernicke's E51.2– warrants queryRed MCC Green Special Emphasis – G94 code50
Coding Clinic, 2nd Q, 2017, pp 8-9 Dr. Kennedydisagreed with thisadvice andregistered hiscomplaint to theCoding Clinic51
ICD-10-CM GuidelinesB. General Coding Guidelines 5. Conditions that are an integral part of a diseaseprocess– Signs and symptoms that are associated routinely with adisease process should not be assigned as additional codes,unless otherwise instructed by the classification. 6. Conditions that are not an integral part of a diseaseprocess– Additional signs and symptoms that may not be associatedroutinely with a disease process should be coded whenpresent.52
ClarificationCoding Clinic, 2nd Quarter, 2018 Question: Coding Clinic Second Quarter 2017, pages 8-9,G93.49, Other encephalopathy, was assigned forencephalopathy secondary to an acute stroke.– Please clarify the appropriate code assignment forencephalopathy when it is caused by some other condition andthe encephalopathy is not specified. Answer: The advice provided in Coding Clinic SecondQuarter 2017, pages 8-9 is accurate.– When encephalopathy is linked to a specific condition, such asstroke or urinary tract infection, it is appropriate to use the codedescribing “other encephalopathy.”– Therefore, assign code G93.49, Other encephalopathy, whenencephalopathy is linked to a condition, but a specificencephalopathy (e.g., metabolic, toxic, hypertensive, etc.) is notdocumented.53
(Acute) Encephalopathy “in” a Disease(e.g. UTI) Not Classified In the Index}A MCCNOT A MCC54
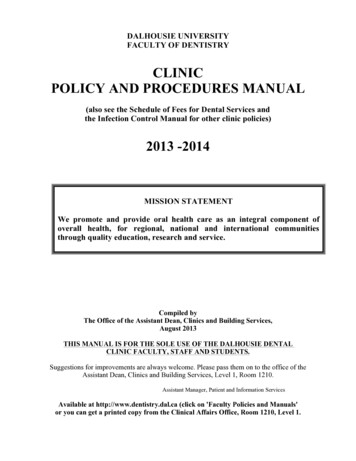
Coding Clinic, 2nd Quarter, 2017, pp 8-9Appropriate use of G94 Question: Patient admitted with septic-associatedencephalopathy. Which code do I use, G93.41,Metabolic encephalopathy, or G94 for Encephalopathyin Diseases Classified Elsewhere (per the Excludes1note) Answer:1. First use the Index to Diseases – Septic Encephalopathygoes to G93.41.2. Second, while there is an Excludes1 note for G93.4x, G94should only be used if it is referenced in the Index.If no specified type of encephalopathy is documented, useG93.4055
Where Does the Index Use G94? Cyst (colloid) (mucous)(simple) (retention)– brain (acquired) G93.0 hydatid B67.99 [G94]– hydatid -see also EchinococcusB67.90 brain B67.99 [G94] Disease, diseased -see alsoSyndrome– brain G93.9 parasitic NEC B71.9 [G94]– parasitic B89 cerebral NEC B71.9 [G94]One has to pay special attention tothe encephalopathy inhyperinsulinism andposthypoglycemic encephalopathy Encephalopathy (acute)G93.40– in (due to) (with) hyperinsulinism E16.1 [G94]– posthypoglycemic (coma)E16.1 [G94] Epilepsy– parasitic NOS B71.9 [G94] Hyperinsulinism– with encephalopathy E16.1 [G94] Malaria– cerebral B50.0 [G94]– falciparum B50.9 with complications NEC B50.8– cerebral B50.0 [G94] Typhus (fever) A75.9– brain A75.9 [G94]– cerebral A75.9 [G94]56
Acute Metabolic Encephalopathy due toHypoglycemia Question: Acute metabolic encephalopathy due tohypoglycemia in a patient with diabetes Answer:– PDx: E11.649, Type 2 diabetes mellitus with hypoglycemiawithout coma– SDx: G93.41, Metabolic encephalopathy (Not G94)NOTE: I16.1 or I16.2 is for hypoglycemia not related to diabetesDiabetes, diabetic (mellitus) (sugar) E11.9- with- - hypoglycemia E11.649- - - with coma E11.641Coding Clinic, 3rd Quarter,2015, page 21Coding Clinic, 3rd Quarter,2016, page 4257
Toxic EncephalopathyClinical versus Coding DefinitionsClinical Definition Brain dysfunctioncaused by toxicexposureCoding – ICD-10-CM Index to DiseasesEncephalopathy (acute) G93.40- due to- - drugs - -see also Table of Drugs andChemicals G92- metabolic G93.41- - drug induced G92Note: The review cited below- - toxic G92focuses on the most- toxic G92significant occupational- - metabolic G92causes of toxicJamaicanencephalopathy, but does not- neuropathy G92address iatrogenic(pharmaceutical) causes orLeukoencephalopathy -see alsothe neurotoxic effects of illicitEncephalopathy G93.49recreational drugs or alcohol- Binswanger's I67.3- heroin vapor G92Kim Y, Kim JW. Toxic Encephalopathy. Saf Health Work. 2012 Dec; 3(4): /PMC3521923/58
Toxic Encephalopathy Code59
Coding Clinic AdviceToxic Encephalopathy 2⁰ Cipro Question: Final diagnostic statement listed,"Toxic encephalopathy due to ciprofloxacin”with the antibiotic properly administered. Answer:– G92, Toxic encephalopathy, as the principaldiagnosis.– T36.8X5A, Adverse effect of other systemicantibiotics, initial encounter, as an additionaldiagnosis.Coding Clinic, 1st Quarter, 2017, page 3960
Coding Clinic AdviceToxic Encephalopathy 2⁰ Lithium ODAssign Code T43.592A, Poisoning by other antipsychotics andneuroleptics, intentional self harm, initial encounter, asthe principal diagnosis. Code G92, Toxic encephalopathy, should be assigned asan additional diagnosis.The code first note is intended to provide sequencingguidance when coding toxic effects, and does not precludeassigning code G92 along with poisoning codes.Coding Clinic, 1st Quarter, 2017, page 4061
Tips on Toxic EncephalopathyCoding – ICD-10-CM There must be an altered mentalIndex to Diseasesstatus of some sortEncephalopathy Both the altered mental status and(acute) G93.40- due tothe underlying brain disease must be- - drugs - -see alsodiscussedTable of Drugs and– Delirium is the manifestation– Toxic encephalopathy due to drug is theunderlying cause There must be some sense that thealtered mental status is an adverseeffect or that the patient has beenoverdosed, especially with legalmood-altering chemicals.Chemicals G92- metabolic G93.41- - drug induced G92- - toxic G9262
Diabetes or Other Conditions“With” or “In” NEC Diseases63
The Words “With” or “In”When Used in the Index or Table“With” The word “with” or “in” should be interpreted to mean“associated with” or “due to” when it appears in a codetitle, the Alphabetic Index, or an instructional note in theTabular List.– The classification presumes a causal relationship between the twoconditions linked by these terms in the Alphabetic Index orTabular List.– These conditions should be coded as related even in the absenceof provider documentation explicitly linking them, unless thedocumentation clearly states the conditions are unrelated orwhen another guideline exists that specifically requires adocumented linkage between two conditions (e.g., sepsisguideline for “acute organ dysfunction that is not clearlyassociated with the sepsis”).64
Not Elsewhere Classifiable (NEC) vs.Not Otherwise Specified (NOS)65
DiabetesIndex to Diseases- with- - amyotrophy E11.44- - arthropathy NEC E11.618- - autonomic (poly) neuropathy E11.43- - cataract E11.36- - Charcot's joints E11.610- - chronic kidney disease E11.22- - circulatory complication NEC E11.59- - complication E11.8- - - specified NEC E11.69- - dermatitis E11.620- - foot ulcer E11.621- - gangrene E11.52- - gastroparalysis E11.43- - gastroparesis E11.43- - glomerulonephrosis, intracapillaryE11.21- - glomerulosclerosis, intercapillaryE11.21- - hyperglycemia E11.65- - hyperosmolarity E11.00- - - with coma E11.01- - hypoglycemia E11.649- - - with coma E11.641- - ketoacidosis E11.10- - - with coma E11.11- - kidney complications NEC E11.29- - Kimmelsteil-Wilson disease E11.21- - loss of protective sensation (LOPS) -seeDiabetes, by type, with neuropathy66
DiabetesIndex to Diseases- With- - mononeuropathy E11.41- - myasthenia E11.44- - necrobiosis lipoidica E11.620- - nephropathy E11.21- - neuralgia E11.42- - neurologic complication NECE11.49- - neuropathic arthropathy E11.610- - neuropathy E11.40- - ophthalmic complication NECE11.39Note how NEC designation islaced throughout thediabetes codes- - oral complication NEC E11.638- - osteomyelitis E11.69- - periodontal disease E11.630- - peripheral angiopathy E11.51- - - with gangrene E11.52- - polyneuropathy E11.42- - renal complication NECE11.29- - renal tubular degenerationE11.29- - skin complication NECE11.628- - skin ulcer NEC E11.62267
NEC in Association with “With” and “In”Coding Clinic, 2nd Quarter, 2018, page 7 The “with” guideline does not apply to “not elsewhereclassified (NEC)” index entries that cover broad categoriesof conditions.– Specific conditions must be linked by the terms “with,” “due to” or“associated with.” For example, arthropathy is a general term for anycondition that affects the joints, and there are differenttypes of arthropathic conditions that are not necessarilyrelated to diabetes.– In order to link diabetes and arthritis, the provider would need todocument the condition as a diabetic complication.– Coding professionals should not assume a causal relationshipwhen the diabetic complication is “NEC.”68
Diabetes With CellulitisCoding Clinic, 4th Quarter, 2017, pp 100-101 Question: A 79-year-old male with type 2 diabetesmellitus presented due to acute cellulitis of the leftlower leg. The patient was admitted and started onbroad-spectrum antibiotics.– When assigning the diabetes code, would it be appropriateto report the code for diabetes “with skin complicationNEC?”– What is the appropriate code assignment for cellulitis in apatient with type 2 diabetes?69
Diabetes With CellulitisCoding Clinic, 4th Quarter, 2017, pp 100-101 Answer: In order to link the diabetes and the cellulitis, theprovider would need to document
Editorial Advisory Board -No advice can be published unless unanimously agreed upon by the four Cooperating Parties In essence, the Supreme Court in coding issues -Used by the Department of Justice and HHS OIG in judging coding compliance Coding Clinic (CC), 1st Quarter 2011, p. 19 Changes in the ICD-9-CM classification supersede .