Transcription
Fundamental Statistics &Epidemiology in Infection PreventionAbout APICAPIC’s mission is to create a safer world through prevention of infection. Theassociation’s more than 15,000 members direct infection prevention programsthat save lives and improve the bottom line for hospitals and other healthcarefacilities. APIC advances its mission through patient safety, implementationscience, competencies and certification, advocacy, and data standardization.
Fundamental Statistics & Epidemiology in Infection Prevention 2016, Association for Professionals in Infection Control and Epidemiology, Inc. (APIC)All rights reserved. Use of this APIC publication does not grant any right of ownership or license to any user.Published in the United States of AmericaFirst edition, June 2016Corrected for digital edition, August 2019ISBN: 978-1-933013-79-4All inquiries about this publication or other APIC products and services may be addressed to:APIC1400 Crystal Drive, Suite 900Arlington, VA 22202Phone: 202-789-1890Fax: 202-789-1899Email: info@apic.orgWeb: www.apic.orgDisclaimerThe Association for Professionals in Infection Control and Epidemiology, its affiliates, directors, officers, and/or agents (collectively,“APIC”) provides this publication solely for the purpose of providing information to APIC members and the general public.The material presented in this publication has been prepared in good faith with the goal of providing accurate and authoritativeinformation regarding the subject matter covered. However, APIC makes no representation or warranty of any kind regarding anyinformation, apparatus, product, or process discussed in this publication and any linked or referenced materials contained therein, andAPIC assumes no liability therefore.WITHOUT LIMITING THE GENERALITY OF THE FOREGOING, THE INFORMATION AND MATERIALS PROVIDEDIN THIS PUBLICATION ARE PROVIDED ON AN “AS-IS” BASIS AND MAY INCLUDE ERRORS, OMISSIONS, OROTHER INACCURACIES. THE USER ASSUMES THE SOLE RISK OF MAKING USE AND/OR RELYING ON THEINFORMATION AND MATERIALS PROVIDED IN THIS PUBLICATION. APIC MAKES NO REPRESENTATIONS ORWARRANTIES ABOUT THE SUITABILITY, COMPLETENESS, TIMELINESS, RELIABILITY, LEGALITY, UTILITY ORACCURACY OF THE INFORMATION AND MATERIALS PROVIDED IN THIS PUBLICATION OR ANY PRODUCTS,SERVICES, AND TECHNIQUES DESCRIBED IN THIS PUBLICATION. ALL SUCH INFORMATION AND MATERIALSARE PROVIDED WITHOUT WARRANTY OF ANY KIND, INCLUDING, WITHOUT LIMITATION, ALL IMPLIEDWARRANTIES AND CONDITIONS OF MERCHANTABILITY, FITNESS FOR A PARTICULAR PURPOSE, TITLE, ANDNON-INFRINGEMENT.IN NO EVENT SHALL APIC BE LIABLE FOR ANY INDIRECT, PUNITIVE, INCIDENTAL, SPECIAL, ORCONSEQUENTIAL DAMAGES ARISING OUT OF OR IN ANY WAY CONNECTED WITH THE USE OF THISPUBLICATION OR FOR THE USE OF ANY PRODUCTS, SERVICES, OR TECHNIQUES DESCRIBED IN THIS GUIDE,WHETHER BASED IN CONTRACT, TORT, STRICT LIABILITY, OR OTHERWISE.
AcknowledgmentsDevelopment of this resource required input and expertise from a broad array of experts from practiceand research settings, including chapters from Section 2 of the APIC Text of Infection Control andEpidemiology, 4th edition (2014). Original authors of those materials are listed below in addition to theauthors of new material prepared for this book. The Association for Professionals in Infection Controland Epidemiology acknowledges the valuable contributions from the following individuals.EditorMonika Pogorzelska-Maziarz, PhD, MPHAssistant ProfessorThomas Jefferson UniversityJefferson College of NursingPhiladelphia, PAAuthorsKathleen Meehan Arias, MS, MT, SM, CICDirectorArias Infection Control Consulting, LLCCrownsville, MDElizabeth A. Campbell, BS, RN, CICInfection Control CoordinatorReston Hospital CenterReston, VAMargaret A. Dudeck, MPH, CPHEpidemiologistSurveillance BranchDivision of Healthcare Quality PromotionCenters for Disease Control and PreventionAtlanta, GAJonathan R. Edwards, MStatResearch Mathematical StatisticianLead, Statistics TeamSurveillance BranchDivision of Healthcare Quality PromotionCenters for Disease Control and PreventionAtlanta, GACarolyn T. A. Herzig, PhD, MSProject DirectorColumbia University School of NursingNew York, NYEricka L. Kalp, MPH, CICDirector, Epidemiology and Infection PreventionSummit HealthChambersburg, PARobert R. Kelley, PhDAssistant Professor of MedicineAssistant Director of Data Management andAnalysisUniversity of Louisville School of MedicineDivision of Infectious DiseasesClinical and Translational ResearchSupport CenterLouisville, KYTimothy Landers, PhD, RN, CNP, CICAssistant ProfessorThe Ohio State UniversityCollege of NursingColumbus, OHElizabeth Monsees, RN, MSN, MBA, CICClinical Safety OfficerChildren’s Mercy Hospitals & ClinicsKansas City, MODeborah M. Nadzam, PhD, RN, FAANDirector, Healthiest Cities & Counties ChallengeCEOs for CitiesCleveland, OHArlene Potts, BA, MPH, CICResearch ScientistNew Jersey State Department of HealthTrenton, NJ
Barbara M. Soule, RN, MPA, CIC, FSHEAPrincipal, Infection Prevention and ControlJoint Commission ResourcesOak Brook, ILProduction TeamCaroline H. Fuchs, CAEVice President, Marketing and Practice ResourcesAPICS. Samantha M. Tweeten, PhD, MPHEpidemiologistEpidemiology and Immunization Services BranchHealth and Human Services AgencyCounty of San DiegoSan Diego, CAChristina James, MPAManager, Practice ResourcesAPICTimothy L. Wiemken, PhD, MPH, CICAssistant Professor of MedicineDirector, University of Louisville HospitalEpidemiology ProgramAssistant Director of Epidemiology andBiostatisticsUniversity of Louisville School of MedicineDivision of Infectious DiseasesClinical and Translational ResearchSupport CenterLouisville, KYSarah VickersArt Director (cover art)APICJames Ebersole, MAAssistant Editor, Practice ResourcesAPICText Design and LayoutProject Design CompanyWashington, DCPrintingModern LithoJefferson City, MOReviewersPatti G. Grota, PhD, CNS-M-S, CICAssistant Professor of NursingInfection Prevention and Patient SafetyConsultant Department ofHealth Restoration and Care SystemsManagement University of TexasHealth Science Center at San AntonioSan Antonio, TXDaniel Bronson-Lowe, PhD, CICSenior Clinical ManagerBaxter Healthcare CorporationUrbana, ILManaging EditorSusan F. SandlerAssociate Director, Practice ResourcesAPICChapter 8: Evaluating Research Studies wasexpanded from "An infection preventionist's guideto evaluating research studies," by Timothy Landersand Monika Pogorzelska-Maziarz, PreventionStrategist, fall 2015.
DisclosuresOnly individuals who have made disclosures of potential conflicts of interest have been listed here.Patti G. Grota, PhD, CNS-M-S, CIC is a Board Member for TNA District #9, San Antonio, TX;President-elect, APIC Chapter 71, San Antonio, TX; Counselor, Sigma Theta Tau Delta Alpha Chapter, SanAntonio, TX; and an Editorial Board Member for the American Journal of Infection Control, 2016-2017.
Table of ContentsIntroduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2SECTION 1: STATISTICS AND EPIDEMIOLOGYChapter 1: General Principles of Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Chapter 2: Use of Statistics in Infection Prevention. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Chapter 3: Risk-Adjusted Comparisons. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54Chapter 4: Surveillance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65Chapter 5: Outbreak Investigation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101SECTION 2: RESEARCH DESIGN AND EVALUATIONChapter 6: Qualitative Research Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118Chapter 7: Overview of Study Designs for Clinical Research. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133Chapter 8: Evaluating Research Studies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143SECTION 3: STATISTICS AND PERFORMANCE IMPROVEMENTChapter 9: Patient Safety. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152Chapter 10: Quality Concepts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182Chapter 11: Performance Measures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197Chapter 12: Process Control Charts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218
2Fundamental Statistics & Epidemiology in Infection PreventionIntroductionWelcome to the first edition of Fundamentals in Statistics and Epidemiology for Infection Prevention. Thisbook is an introduction to statistics and epidemiology and their application to the practice of infectionprevention and control.Infection Prevention & Control is a core domain within the APIC Competency Model for theInfection Preventionist (IP). Included in this domain are competencies in the areas of epidemiology andsurveillance, risk assessment and reduction, and research. This book serves as a resource for the noviceand intermediate IP to develop understanding and knowledge of these areas.The book is divided into three sections: Section 1: Statistics and Epidemiology presents the general principles of infectious disease epidemiology,surveillance, and outbreak investigations. In addition, this Section provides an introduction to basicstatistical knowledge and use of risk adjusted comparisons in infection prevention. Section 2: Research Design and Evaluation provides information on qualitative and quantitativeresearch methods, as well as a guide to evaluating the quality of research studies. Section 3: Statistics and Performance Improvement focuses on the patient safety science and qualityimprovement methods as they apply to the field of infection prevention.Much of this book has been adapted from the materials previously published in the APIC Text of InfectionControl and Epidemiology, 4th Edition. Some sections have been expanded, some have added content,and revisions have been made to present the information in a practical format. I greatly appreciate theefforts of the chapter authors in developing these materials.Fundamentals in Statistics and Epidemiology for Infection Prevention should provide the IP with a deeperunderstanding of basic conceptual and methodological underpinnings of epidemiology and statistics asthey apply to the practice of infection prevention. It is my hope that the information provided in thisbook will help the IP to guide their practice.Monika Pogorzelska-Maziarz, PhD, MPHAssistant ProfessorThomas Jefferson University, Jefferson College of NursingPhiladelphia, PA
SECTION 1:STATISTICS AND EPIDEMIOLOGY
4Fundamental Statistics & Epidemiology in Infection PreventionCHAPTER 1General Principles of EpidemiologyS. Samantha M. Tweeten, PhD, MPHEpidemiologistEpidemiology & Immunization Services BranchHealth and Human Services AgencyCounty of San DiegoSan Diego, CAAbstractEpidemiology, the study of the frequency, distribution, cause, and control of disease in populations, forms thebasis of all health-related studies. It provides the background for interventions to reduce transmission of infectingorganisms, reduce the number of healthcare-associated infections, and protect healthcare providers from infection.Understanding the relationships of host, environment, and organism will aid the infection preventionist in designingstudies to determine the cause of healthcare-associated infections and design interventions.BACKGROUNDT he purpose of this chapter is to provide information about the epidemiological principles andmethods used in the practice of infection surveillance, prevention, and control and to show thatthey are an important part of the discipline known as epidemiology.The infectious disease process is a set of complex interrelationships of agent, host, and environment thathas been studied by epidemiologists for more than a century. One goal of epidemiology is to understandthe natural history of diseases and conditions to develop strategies for their prevention and control.Three closely interrelated components—distribution, determinants, and frequency—are integral tothe principles and methods of epidemiology. By becoming familiar with these concepts, the infectionpreventionist will begin to develop and expand a knowledge base for interpreting data gathered withinand outside the healthcare facility and for understanding the associations between risk factors andinfection in different settings and how these findings can be used to reduce infection risks for patientsand healthcare workers. The Supplemental Resources cited at the end of this chapter reflect the breadthand depth of the discipline.Although information is provided about the theoretical basis for epidemiology and statistics, the principalgoal of this chapter is to present practical information that will allow the infection preventionist to useepidemiological skills in day-to-day practice. Following completion of this chapter, it is hoped that thelearner will have a better understanding of epidemiology and how principles of epidemiology can beapplied to many practice issues in infection prevention and control.
Fundamental Statistics & Epidemiology in Infection PreventionBASIC PRINCIPLESEpidemiology is the study of the distribution and determinants of disease and other conditions in humanpopulations, both a body of knowledge and a method of study. Epidemiology encompasses the study ofmany factors that are detrimental to human health, including infectious diseases, chronic diseases such ascancer or heart disease, drug or alcohol abuse and their sequelae, violence, injury, and others.Epidemiology, unlike clinical medicine, is population-based and is useful for describing health-relatedphenomena in groups of people. Epidemiological methods are used in the measurement of a disease,its determinants, and its distribution in a particular population in question before, during, and after anintervention. Epidemiology provides information for community and preventive medicine, analysis ofhealth assessments, safety programs, utilization review and management of resources, and health planningand forecasting. As an applied science, epidemiology is a professional discipline that encompasses allacademic fields of study.Epidemiological Study DesignThe primary purpose of epidemiology is to aid in the understanding of the cause of a disease byknowing its distribution, determinants in terms of person, place, and time, and natural history.This information is also used in epidemiology to plan and evaluate interventions and preventionefforts more effectively. To this end, several approaches, or methodologies, are used in obtainingepidemiological information. These include observational studies, in which the natural course of eventsis observed. Observational studies may be either descriptive, in which events are described in termsof person, place, or time, or analytical, in which risk factors and trends are observed and compared.The three main types of analytical observational studies are cross-sectional, cohort and case-controlstudies. In a cross-sectional study, data on risk factors (exposures) and outcomes are collected at onepoint in time and these studies provide a snapshot of a sample population at one point in time. Ina cohort study, a group of subjects with a known exposure status for the risk factor(s) of interest arefollowed over time to determine which of the subjects develops disease. These subjects form a cohortgoing through time together. In contrast, case-control studies move backward from the disease stateto risk factor by first identifying persons with and without the disease (cases and controls) and thenmeasuring and comparing their degree of exposure to the risk factor(s) of interest in the past.In experimental studies the investigator actively intervenes to modify one or more factors. Experimentalstudies are prospective in nature: data are gathered as subjects move from the present into the future, whilebeing followed up by the researcher. These methodologies are described in greater detail in Chapter 7.Association Versus CausationAssociation occurs if, as one variable changes, there is a concomitant or resultant change in the quantityor quality of another variable. When a statistical association between an exposure (or risk factor) andan outcome (e.g., disease) has been demonstrated, it may be of three types: artifactual (or spurious),indirect or noncausal, or causal. A certain number of associations will simply occur by chance, with thenumber of associations rising as a greater number of factors or variables are studied. This is known asrandom error. Random error refers to the probability that the observed results are likely due to chancealone. Different statistical tools allow evaluating the degree to which random error is likely to explain theobserved results (see Chapter 2).5
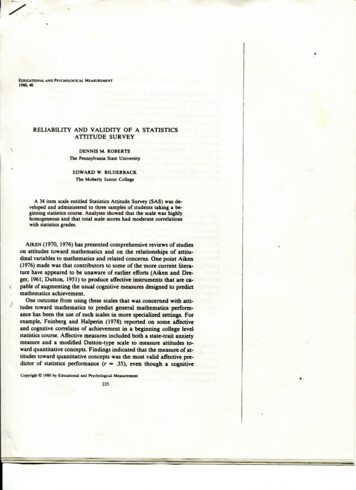
6Fundamental Statistics & Epidemiology in Infection PreventionArtifactual associations may also be caused byFigure 1.1errors in study design or analysis, leading to theConfounding variableintroduction of systematic error or bias. Bias instudy design refers to a systematic error in the wayConfounderthat the study was designed or conducted whichresults in incorrect estimates of the associationExposureOutcomebetween the exposure and the outcome. Bias maybe caused by instrument, observer, data collectionmethod, case and control group selection (selectionbias resulting in subject groups not being comparable), or other errors and can arise in all types of studydesigns. Errors in analysis, including inappropriate choice of statistical test and under-powering ofstudies, may also lead to bias. Bias may result in no association being seen when one actually exists orcreating the appearance of an association when there is none.Failure to control for confounding in the study design or analysis may also result in artifactualassociations. Confounding is the mixing of effect between the exposure, outcome and a third variable. Aconfounder is a variable that is an independent cause or predictor of the exposure and the outcome andis not on the path between the exposure and the outcome (Figure 1.1). Indirect or noncausal associationsmay result from confounding variables and can lead to the assumption that there are differences that donot really exist or to the observation that there is no difference when one truly exists.Causal associations exist when evidence indicates that one factor is clearly shown to increase theprobability of the occurrence of a disease. In a causal relationship, the reduction, or diminution, of afactor decreases the frequency of the disease being studied. This should not be confused with causality,which requires the presence of a number of conditions including causal association.When conducting an epidemiologic study, the potential sources of errors described above must beinvestigated and described in order to estimate the effect that error may have played in the observed results.A study is considered to have internal validity (i.e., the observed result is likely to be true) if these alternativeexplanations or sources of error are explored and ruled out. Importantly, a study must have internal validitybefore the results of the study can be generalized from the study subjects to a larger population. Evaluatingthe generalizability or external validity of a study is based on a review of the specific study population,research methodology, and the specific aspects of the outcome or disease under study.Scientific Criteria for Disease CausationThe scientific criteria for disease causation have their roots in Koch’s postulates (Robert Koch, 1843–1910). Koch’s postulates consist of four points:1. The organism must always be found with the disease, in accordance with the clinical stage observed.2. The organism must then be grown in pure culture from a diseased host.3. The same disease must be reproduced when a pure culture of the organism is inoculated into ahealthy susceptible host.4. The organism must then be recovered from the experimentally infected host.
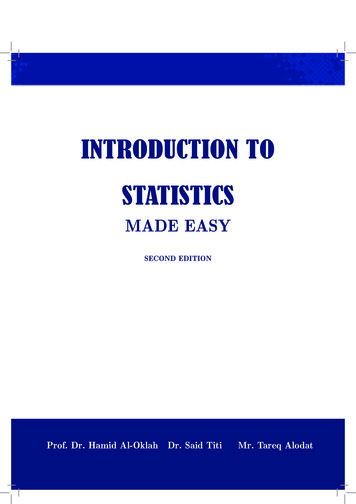
Fundamental Statistics & Epidemiology in Infection PreventionThese postulates were originally accepted as anattempt to establish a causal relationship betweenmicroorganisms and disease processes. Althoughhistorically significant, as we have learned moreabout disease causation, it has become apparent thatKoch’s postulates cannot always be fulfilled (e.g.,multicausal diseases, chronic diseases, some viraldiseases). Koch himself accepted that not all of hiscriteria would be met in each case.Table 1.1Hill's criteria for causationThe currently used criteria for causality weredeveloped by Austin Bradford Hill (1897–1991)and are known as Hill’s criteria. These criteria use modern epidemiological methods to determine whethera factor is causal for a given disease and are listed in Table 1.1. These criteria are equally applicable toinfectious and noninfectious diseases.1. Strength of association is the first criterion: The incidence of disease should be higher in those whoare exposed to the factor under consideration than in those who are not exposed; that is, the strongerthe association between an exposure and a disease, the more likely the exposure is to be causal. Forexample, lung cancer is common in those who smoke.2. Consistency means that the association should be observed in numerous studies, preferably bydifferent researchers using different research methodologies.3. Specificity refers to an association between one factor and one disease, and this association is morelikely to be causal. This criterion also refers to the extent to which the occurrence of one factor can beused to predict the occurrence of another (disease). In reality, such a one-to-one relationship is raredue to the multifactorial causes of most diseases and because, sometimes, the same factor(s) can causemore than one disease.4. Temporality must also be addressed when determining cause of disease. Essentially, exposure to thehypothesized causal factor must precede the onset of disease.5. The biological gradient is a dose-response relationship between increased exposure to a factor andincreased likelihood of disease. For example, the longer one smokes, the more likely one is to developlung cancer. If the association demonstrates a biological gradient between the factor (exposure) andeffect (disease), the relationship is more likely to be causal.6. The association in question should also be biologically plausible in light of current knowledge. Thiscriterion may be the most elusive and variable of the nine. Because biological knowledge is everexpanding, lack of biological plausibility does not necessarily disprove a theoretical association.7. There should be coherence between known information about the biological spectrum of the diseaseand the associated factor; that is, the association should be in accordance with other facts knownabout the natural history of the disease.8. Associations derived from experiments add considerable weight to evidence supporting causalassociations. These experiments can be animal model studies or clinical trials; although animalmodels may be helpful, many diseases do not manifest the same way in animals and humans.7
First edition, June 2016 Corrected for digital edition, August 2019 ISBN: 978-1-933013-79-4 All inquiries about this publication or other APIC products and services may be addressed to: APIC 1400 Crystal Drive, Suite 900 Arlington, VA 22202 Phone: 202-789-1890 Fax: 202-789-1899 Email: info@apic.org Web: www.apic.org Disclaimer