Transcription
BRUCELLOSIS REFERENCE GUIDE:EXPOSURES, TESTING, AND PREVENTION
CONTACT INFORMATIONBacterial Special Pathogens Branch (BSPB)Division of High-Consequence Pathogens and PathologyNational Center for Emerging and Zoonotic Infectious DiseasesCenters for Disease Control and Prevention1600 Clifton Rd MS C–09, Atlanta, GA 30329-4027(404) 639-1711, BSPB@cdc.govDivision of Select Agents and Toxins (DSAT)Centers for Disease Control and Prevention1600 Clifton Rd MS A–46, Atlanta, GA 30329-4027Fax: (404) 718-2096, lrsat@cdc.govhttp://www.selectagents.gov/Emergency Operations Center (EOC)Office of Public Health Preparedness and ResponseCenters for Disease Control and Prevention(770) 488-7100Laboratory Preparedness and Response Branch (LRN)Division of Preparedness and Emerging InfectionNational Center for Emerging, Zoonotic and Infectious DiseaseCenters for Disease Control and Prevention1600 Clifton Rd MS C–18, Atlanta, GA 30329-4027LRN@cdc.govUpdated February 2017Brucellosis Reference Guide: Exposures, Testing, and Prevention
TABLE OF CONTENTSContact Information.inside coverDescription.1Clinical Description.1Case Classification1, 2.1Human Pathogens and Select Agent Reporting.2Select Agent Designation.2Laboratory Response Network (LRN) 6.3Reportable and Nationally Notifiable Disease Classification and Requirements 7.3Case Report Form.4Diagnostic Testing.4CDC/CSTE Laboratory Criteria for Diagnosis1.4Testing performed at CDC.5Diagnostic Difficulties.6Treatment13, 14.7Laboratory, Surgical, and Clinical Exposures.8Laboratory Exposures4, 15.8Clinical Exposure. 12Surgical Exposure22, 23. 12Veterinary Exposures. 14Vaccine Exposure. 14Clinical Exposure. 15Marine Mammal Exposure28, 29. 15Foodborne Exposure. 16Recreational Exposure. 17Feral Swine Hunting. 17Brucellosis in Pregnant Women. 17Person-to-Person Transmission. 18Neonatal Brucellosis36–40. 18Sexual Transmission41-48. 19Organ Donations and Blood Transfusions. 19Prevention. 19Occupational Exposures. 19Recreational Exposures (Hunter Safety). 20Travel to Endemic Areas. 20Brucellosis Reference Guide: Exposures, Testing, and Prevention
References. 21Additional Sources of Brucellosis Information:.24Appendix 1: Specimen Submission.26Submission of Serum for Brucella Serology. 26Submission of Brucella Isolate(s). 27Appendix 2: Post-Exposure Monitoring.28Follow-up of Brucella occupational exposure. 28Symptom Monitoring. 28Appendix 3: Interim Marine Mammal Biosafety Guidelines. 32Brucellosis Reference Guide: Exposures, Testing, and Prevention
DESCRIPTIONClinical DescriptionCouncil of State and Territorial Epidemiologists (CSTE)1 2010 Case DefinitionAn illness characterized by acute or insidious onset of fever and one or more of the following: night sweats,arthralgia, headache, fatigue, anorexia, myalgia, weight loss, arthritis/spondylitis, meningitis, or focal organinvolvement (endocarditis, orchitis/epididymitis, hepatomegaly, splenomegaly).Incubation Period Highly variable (5 days–6 months) Average onset 2–4 weeksSymptoms/Signs Acute Non-specific: Sub-clinicalFever, chills, sweats, headache, myalgia, arthralgia, anorexia, fatigue, weight lossinfections are common Lymphadenopathy(10–20%), splenomegaly (20–30%) Chronic Recurrentfever Arthritisand spondylitis Possiblefocal organ involvement (as indicated in the case definition)Case Classification1, 2Probable—A clinically compatible illness with at least one of the following: Epidemiologically linked to a confirmed human or animal brucellosis case Presumptive laboratory evidence, but without definitive laboratory evidence, of Brucella infectionConfirmed—A clinically compatible illness with definitive laboratory evidence of Brucella infectionPlease refer to the CSTE Laboratory Criteria for Diagnosis section for specifications regarding “presumptive”and “definitive” laboratory evidence of a Brucella infection.Brucellosis Reference Guide: Exposures, Testing, and Prevention1
HUMAN PATHOGENS AND SELECT AGENT REPORTINGSelect Agent DesignationSelect agents and toxins are a subset of biological agents and toxins that may pose a severe threat to publichealth.3 Brucella species are easily aerosolized and have a low infectious dose, cited at levels between 10 and100 microorganisms. These organisms also have a prolonged incubation period with the potential to inducea broad range of clinical manifestations, and therefore generate challenges for prompt diagnosis. The abovefactors have contributed to a select agent designation for B. suis, B. melitensis, and B. abortus.4, 5Clinical or diagnostic laboratories and other entities that have identified B. suis, B. melitensis, or B. abortusare required to immediately (within 24 hours) notify the Division of Select Agents and Toxins (DSAT) at CDC(fax: 404-718-2096; email: lrsat@cdc.gov).Facilities that use or transfer B. suis, B. melitensis, or B. abortus must immediately (within 24 hours) notify DSATvia phone, fax, or e-mail if they detect any theft, loss, or release of these select agents. The initial report shouldinclude as much information as possible about the incident, including the type of incident, date and time,agent and quantity, and a summary of the events (location of the incident, number of individuals potentiallyexposed, actions taken to respond, etc.). Additionally, appropriate local, state, or federal law enforcementagencies should be contacted of a theft or loss, and appropriate local, state, and federal health agenciesnotified of a release.3Forms for Reporting to CDC’s Division of Select Agents and Toxins (DSAT)Form 4, Report of the Identification of a Select Agent or Toxin: Clinical or APHIS/CDC Form 4A should besigned and submitted after a facility has identified B. suis, B. melitensis, or B. abortus contained in a clinical/diagnostic specimen. Entities must submit Form 4 to DSAT within 7 calendar days of identification. Forassistance with the completion of this form, please contact CDC’s Division of Select Agents and Toxins viaemail at lrsat@cdc.gov.Form 3, Report of Theft, Loss, or Release of Select Agents and Toxins: The APHIS/CDC Form 3 should besubmitted by facilities reporting a theft, loss, or release (laboratory exposure or release of an agent outsideof the primary barriers of the biocontainment area) of B. suis, B. melitensis, or B. abortus within 7 calendar daysof the event. For reporting of a theft or loss, complete sections 1 and 2 of Form 3; for reporting a release,complete sections 1, 2, and 3. With questions regarding the Form 3, please send an e-mail to form3@cdc.gov.Exclusions from Select Agent ReportingSelect agents in their naturally occurring environment are not subject to regulation and may include animalsthat are naturally infected with a select agent or toxin (e.g., milk samples that contain B. abortus). However, aselect agent or toxin that has been intentionally introduced (e.g., animal experimentally infected with B. suis,B. melitensis, or B. abortus), or otherwise extracted from its natural source (e.g., blood from a culture bottle isplated onto agar and grows B. suis) is subject to select agent regulation.3Attenuated vaccine strains of B. abortus Strain 19 live vaccine and B. abortus Strain RB51 are excluded fromselect agent reporting requirements, unless there is any reintroduction of factor(s) associated with virulence.3Visit the Select Agents and Toxins Exclusions site for a comprehensive list of attenuated Brucella strainexclusions. Please refer to the APHIS/CDC Form 5, Request for Exemption of Select Agents and Toxins foran Investigational Product, to request an exemption from the select agent regulations.Brucellosis Reference Guide: Exposures, Testing, and Prevention2
Laboratory Response Network (LRN) 6The LRN is a national network of local, state, federal, military, and international public health, food testing,veterinary diagnostic, and environmental testing laboratories that provides laboratory infrastructure andcapacity to respond to biological and chemical public health emergencies.Upon obtaining high confidence presumptive or confirmatory Brucella spp. results, LRN laboratories arerequired to follow notification and messaging procedures.Notification: Within 2 hours of obtaining high-confidence presumptive or confirmatory result, a LRNLaboratory Director or a designee must notify: their State Public Health Laboratory Director, the State Epidemiologist, the Health Officer for the State Public Health Department, the CDC Emergency Operations Center (EOC), and the FBI Weapons of Mass Destruction (WMD) POC.Messaging: For emergency and non-emergency situations, LRN laboratories will submit data for all samples,including positive and negative results related to the event within 12 hours of obtaining each result.Please refer to Table 1 below for information regarding personnel who should be contacted, along with atimeline for notification and messaging communication.Reportable and Nationally Notifiable Disease Classification and Requirements 7Brucellosis is a reportable disease in all 57 states and territories; it is mandatory that disease cases be reportedto state and territorial jurisdictions when identified by a health provider, hospital, or laboratory. Reportingrequirements vary by jurisdiction.Brucellosis is also a nationally notifiable condition. Notification of brucellosis cases (without direct personalidentifiers) to CDC by state and territorial jurisdictions is voluntary for nationwide aggregation and monitoringof disease data. The case definition for confirmed and probable brucellosis can be found on page 3 under theCase Classification section.Immediate, Urgent Notification Status: For multiple confirmed and probable cases, temporally or spatiallyclustered, notify EOC within 24 hours of a case meeting the notification criteria, followed by submission ofelectronic case notification in the next regularly scheduled electronic transmission.Standard: For confirmed and probable cases that are not temporally or spatially clustered, submit electroniccase notification within the next reporting cycle.Brucellosis Reference Guide: Exposures, Testing, and Prevention3
Table 1: Reporting Known Brucella spp. Human PathogensReporting Notification StatusDSATSelect AgentDesignationBrucella speciesBrucella melitensisSelect AgentBrucella suisIdentification(Form 4)24 hours7 daysFor a abortusExposure(Form 3)LRNNationallyNotifiableCondition7 days2 hours24 hours or 7 days7 days2 hours24 hours or 7 days7 days2 hours24 hours or 7 daysNot a Select AgentN/AN/A2 hours24 hours or 7 daysBrucella ceti, pinnipedialis Not a Select AgentN/AN/A2 hours24 hours or 7 daysBrucella canisCase Report FormHealth departments and providers are strongly encouraged to use the approved case report form to reportbrucellosis cases to the Bacterial Special Pathogens Branch. This mechanism will ensure improved collectionof standardized data needed to assess risk factors and trends associated with brucellosis, so that targetedpreventive strategies can be implemented. Patient identifiers such as full name, address, phone number,hospital name, and medical record number should not be included in forms sent to CDC. Instructions forcompletion and submission are included in pages 1 and 2 of the form.DIAGNOSTIC TESTINGCDC/CSTE Laboratory Criteria for Diagnosis1Definitive Culture and identification of Brucella spp. from clinical specimensEvidence of a four-fold or greater rise in Brucella antibody titer between acute and convalescent phaseserum specimens obtained greater than or equal to 2 weeks apartPresumptive Brucella total antibody titer of greater than or equal to 1:160 by standard tube agglutination test (SAT)or Brucella microagglutination test (BMAT) in one or more serum specimens obtained after onset ofsymptomsDetection of Brucella DNA in a clinical specimen by PCR assayNOTE: Evidence of Brucella antibodies by nonagglutination-based testsDOES NOT meet the current CDC/CSTE case definition for aPresumptive Diagnosis of brucellosis. However, ANY quantitative test can be used for confirmation ifthere is a four-fold or greater rise in Brucella antibody titer.Brucellosis Reference Guide: Exposures, Testing, and Prevention4
Testing Performed at CDCThe Zoonotic and Select Agent Laboratory (ZSAL) at CDC performs CLIA-approved Brucella spp. diagnostictesting on human and animal samples.Table 2: Diagnostic Testing Provided by onsCultureTissue, wholeblood, sera,plasmaGold standard; allowsfor genotypingmolecular epidemiologyRequires BSL-3See Appendix 1:Submission ofBrucella IsolatesLRN PCR(for suspectBT andresponse use)Environmentalsamples, swabs,powders, wholeblood, sera, tissueRapid detection; canbe used on isolates andclinical specimensRequires technical expertiseto perform assay; reagentsand equipment can becostly; optimal specimentype not clearSee Appendix 1:Submission ofBrucella IsolatesSeraCheap, assay ofchoice in acute noncomplicated cases; onlyequipment needed isreading apparatusMay not diagnose chronicor complicated cases;subjectiveSee Appendix 1:Submission of Serumfor Brucella SerologyMAT(serology)Not available forB. canis or RB51Results and Notification BMAT results take 2 to 3 weeks, depending on when your sample was received at CDC’s Zoonotic andSelect Agent Laboratory (ZSAL), which is part of the Bacterial Special Pathogens Branch (BSPB). Our labwill generally test your sample within 1 week; however, it can take longer to report results. Results will besent to your State Laboratory.After checking with your State Laboratory, you can contact ZSAL or the BSPB epidemiology team if resultsare not received within 2 to 3 weeks.PCR results from primary specimens can be obtained within 24 hours.Testing Performed Elsewhere CDC does not provide medical consultation on individual patients, and cannot comment on results fromlaboratory assays that we have not performed.We recommend that you consult both with an infectious disease specialist assigned to the patient and themedical director for the diagnostic laboratory that ran the tests for interpretation of results, as they havethe available parameters for the specific assay used.Brucellosis Reference Guide: Exposures, Testing, and Prevention5
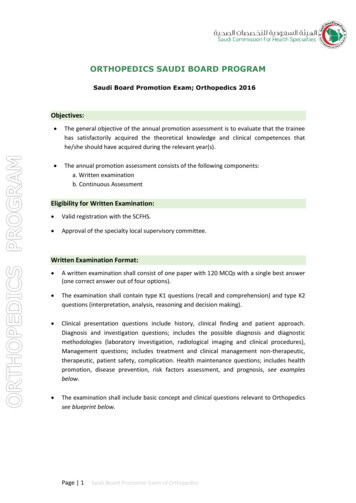
Diagnostic DifficultiesWhile culture is the gold standard, Brucella spp. can be fastidious, slow growers. Culture from primaryspecimens may require up to 21 days of incubation. Bone marrow culture is more sensitive than blood;however, the invasiveness of the procedure should be considered. Persons with chronic infections are less likelyto be culture-positive.Agglutination is a confirmatory serological test to diagnose brucellosis. The standard tube agglutination test(SAT) is the reference method, of which BMAT is a modified format. Brucella-specific agglutination tests involve direct agglutination of bacterial antigens by specific antibodies.Agglutination tests detect antibodies of IgM, IgG, and IgA classes.IgM antibodies are predominant in acute infection but decline within weeks. Relapses are accompanied bytransient elevations of IgG and IgA antibodies but not IgM.PositiveBloodCulturesAcute ting IgGIgAAcute(up to 3 mo.)nonagglutinating IgASubacute(3 mo. - 1 yr)Chronic(1 yr. onward)Stage of BrucellosisFigure 1: Antibody Responses in Untreated Brucellosis.8IgM detection sensitivities using other EIA formats have been reported between 67% to 100% with limitedspecificity data.9, 10 Such tests are qualitative, making them difficult to interpret in a clinical setting, and mighthave different performance characteristics and utility when used in areas with low disease prevalence, such asthe United States. Results of EIA tests must be confirmed by a quantitative reference method such as BMAT.BMAT Testing DrawbacksCross-reactions and false-positive test results can occur in Brucella antibody tests, mainly with IgM.10The primary immunodeterminant and virulence factor for Brucella species is smooth lipopolysaccharide (S-LPS)on the outer cell membrane, which is antigenically similar to the lipopolysaccharide of other gram-negativerods. False-positive Brucella test results can be caused by cross-reactivity of antibodies to Escherichia coli O157,Francisella tularensis, Moraxella phenylpyruvica, Yersinia enterocolitica, certain Salmonella serotypes, and from personsvaccinated against Vibrio cholerae.BMAT tends to perform better for diagnosing acute cases rather than chronic cases.11 Additionally, BMAT isnot as useful in detecting chronic brucellosis cases or neurobrucellosis. In a suspected chronic case, an IgGELISA would be more informative.12Brucellosis Reference Guide: Exposures, Testing, and Prevention6
Treatment 13, 14The table below provides a summary of the Red Book treatment recommendations, as well as severalrecommended treatment documents. Information about post-exposure prophylaxis is provided below in thesection titled “Laboratory, Surgical, and Clinical Exposures.”Table 3: Brucellosis Treatment OptionsSubjectSummaryCombination therapy to decrease the incidence of relapse: Adults,Children 8 yearsOral doxycycline (2–4 mg/kg per day, maximum 200 mg/day, in 2 divided doses) or oraltetracycline (30–40 mg/kg per day, maximum 2 g/day, in 4 divided doses) -and- Rifampin (15–20 mg/kg per day, maximum 600–900 mg/day, in 1 or 2 divided doses). Recommended for a minimum of 6 weeks.Combination therapy with trimethoprim-sulfamethoxazole (TMP-SMZ) can be used iftetracyclines are contraindicated. Children 8 yearsPregnancyCombination therapy: consider adding rifampin. Consult physician for dosing or ifrifampin is contraindicated. Tetracyclines (such as doxycycline) should be avoided inchildren less than 8 years of age.Tetracyclines are contraindicated for pregnant patients. Consult obstetrician regardingspecific antimicrobial therapy instructions. Complicated Cases(endocarditis,meningitis,osteomyelitis, etc.)Oral TMP-SMZ (trimethoprim, 10 mg/kg per day, maximum 480 mg/day; and sulfamethoxazole,50 mg/kg per day, maximum 2.4 g/day) divided in 2 doses for 4 to 6 weeks. Streptomycin* or gentamicin for the first 14 days of therapy in addition to atetracycline for 6 weeks (or TMP-SMZ if tetracyclines are contraindicated).Rifampin can be used in combination with this regimen to decrease the rate of relapse.For life-threatening complications, such as meningitis or endocarditis, duration oftherapy often is extended for 4 to 6 months.Case-fatality rate is 1%.Surgical intervention should be considered in patients with complications such asdeep tissue abscesses.*May not be readily available in the U.S. Referencesfor TreatmentRecommendations Ariza J et al. 2007. Perspectives for the Treatment of Brucellosis in the 21st Century:The Ioannina Recommendations. PLoS Med. 4(12): e317. 71/journal.pmed.0040317Al-Tawfiq JA. 2008. Therapeutic options for human brucellosis. Expert Rev Anti InfectTher. 6(1): 109-120. http://www.ncbi.nlm.nih.gov/pubmed/18251668Solera J. 2010. Update on brucellosis: therapeutic challenges. Intl J Antimicrob Agent.36S, S18–S20. http://www.ncbi.nlm.nih.gov/pubmed/20692127Note: The B. abortus strain used in the RB51 vaccine was derived by selection in rifampin-enriched media and is resistant to rifampin in vitro.This strain is also resistant to penicillin. If infection is due to this vaccine strain, treatment should be determined accordingly (example:doxycycline and TMP/SMX in place of rifampin). Specifics on the regimen and dose should be established in consultation with the person’shealth care provider in case of contraindications to the aforementioned.Brucellosis Reference Guide: Exposures, Testing, and Prevention7
LABORATORY, SURGICAL, AND CLINICAL EXPOSURESLaboratory Exposures4, 15Once a potential exposure is recognized, the first task is to determine the activities performed that may haveled to the exposure. Then identify:1. who was in the laboratory during the suspected time(s) of exposure2. where they were in relation to the exposure3. what they did with the isolatesThe identified individuals should be assessed for exposure risk using the descriptions in Table 4.Table 4. Laboratory Risk Assessment and Post-Exposure Prophylaxis (PEP): Minimal (but not zero) RiskSpecimenhandlingRoutine clinicalspecimen (e.g.,blood, serum,cerebrospinalfluid)Exposure scenarioPEPFollow-up/monitoringPerson who manipulates a routineclinical specimen (e.g., blood, serum,cerebrospinal fluid) in a certified ClassII biosafety cabinet, with appropriatepersonal protective equipment (i.e.,gloves, gown, eye protection).N/APerson present in the lab while someonemanipulates a routine clinical specimen(e.g., blood, serum, cerebrospinal fluid)in a certified Class II biosafety cabinet,or on an open bench where manipulationdid not involve occurrence of aerosolgenerating events (e.g., centrifugingwithout sealed carriers, vortexing,sonicating, spillage/splashes).May consider symptom watch forfollowing scenarios: NoneEnriched material(e.g., a Brucellaisolate, positiveblood bottle)or reproductiveclinical specimen(e.g., amnioticfluid, placentalproducts)Person who manipulates enriched material(e.g., a Brucella isolate, positive bloodbottle) or reproductive clinical specimen(e.g., amniotic fluid, placental products)in a certified Class II biosafety cabinet,with appropriate personal protectiveequipment (i.e., gloves, gown, eyeprotection).Person present in the lab while someonemanipulates enriched material (e.g., aBrucella isolate, positive blood bottle)or reproductive clinical specimen (e.g.,amniotic fluid, placental products) ina certified Class II biosafety cabinet.Brucellosis Reference Guide: Exposures, Testing, and Prevention Person who manipulates a routineclinical specimen (e.g., blood,serum, cerebrospinal fluid) onan open bench with or withoutappropriate personal protectiveequipment (i.e., gloves, gown,eye protection), or in a certifiedClass II biosafety cabinet withoutappropriate personal protectiveequipment.Person present in the lab whilesomeone manipulates a routineclinical specimen (e.g., blood,serum, cerebrospinal fluid) onan open bench, resulting inoccurrence of aerosol-generatingevents (e.g., centrifuging withoutsealed carriers, vortexing,sonicating, spillage/splashes).8
Table 4. Laboratory Risk Assessment and Post-Exposure Prophylaxis (PEP): Low RiskSpecimenhandlingEnriched material(e.g., a Brucellaisolate, positiveblood bottle)or reproductiveclinical specimen(e.g., amnioticfluid, placentalproducts)Exposure scenarioPerson present in the lab at a distanceof greater than 5 feet from someonemanipulating enriched material (e.g., aBrucella isolate, positive blood bottle)or reproductive clinical specimen (e.g.,amniotic fluid, placental products),on an open bench, with no occurrenceof aerosol-generating events (e.g.,centrifuging without sealed carriers,vortexing, sonicating, spillage/splashes).Brucellosis Reference Guide: Exposures, Testing, and PreventionPEPMay consider ifimmunocompromisedor pregnant.Discuss with healthcare provider (HCP).Note: RB51 isresistant to rifampinin vitro, and thereforethis drug should notbe used for PEP ortreatment courses.Follow-up/monitoringRegular symptomwatch (e.g., weekly)and daily self-feverchecks through24 weeks postexposure, after lastknown exposure.Sequentialserologicalmonitoring at 0(baseline), 6, 12, 18,and 24 weeks postexposure, after lastknown exposure.Note: no serologicalmonitoringcurrently availablefor RB51 and B.canis exposures inhumans.9
Table 4. Laboratory Risk Assessment and Post-Exposure Prophylaxis (PEP): High RiskSpecimenhandlingRoutine clinicalspecimen (e.g.,blood, serum,cerebrospinalfluid)Exposure scenarioPEPPerson who manipulates a routine clinicalspecimen (e.g., blood, serum, cerebrospinalfluid), resulting in contact with broken skin ormucous membranes, regardless of workingin a certified Class II biosafety cabinet, withor without appropriate personal protectiveequipment (i.e., gloves, gown, eye protection).Doxycycline 100mgtwice daily, andrifampin 600 mg oncedaily, for three weeks.Person who manipulates (or is 5 feet fromsomeone manipulating) enriched material(e.g., a Brucella isolate, positive blood bottle)or reproductive clinical specimen (e.g.,amniotic fluid, placental products), outside ofa certified Class II biosafety cabinet.Enrichedmaterial (e.g., aBrucella isolate,positive bloodbottle) orreproductiveclinical specimen(e.g., amnioticfluid, placentalproducts)Person who manipulates enriched material(e.g., a Brucella isolate, positive blood bottle)or reproductive clinical specimen (e.g.,amniotic fluid, placental products), within acertified Class II biosafety cabinet, withoutappropriate personal protective equipment(i.e., gloves, gown, eye protection).All persons present during the occurrence ofaerosol-generating events (e.g., centrifugingwithout sealed carriers, vortexing, sonicating,spillage/splashes) with manipulation ofenriched material (e.g., a Brucella isolate,positive blood bottle) or reproductive clinicalspecimen (e.g., amniotic fluid, placentalproducts) on an open bench.For patients withcontraindicationsto doxycycline orrifampin: TMPSMZ, in addition to
Presumptive laboratory evidence, but without definitive laboratory evidence, of Brucella infection Confirmed—A clinically compatible illness with definitive laboratory evidence of Brucella infection Please refer to the CSTE Laboratory Criteria for Diagnosis section for specifications regarding "presumptive"