Transcription
U W H e a lt h S p o r t s R e h a b i l i t a t i o nPlatelet-Rich Plasma RehabilitationGuidelinesWhat is Tendinopathy?Tendons are strong bands of connectivetissue comprised primarily of asubstance called collagen. Mechanically,tendons connect muscle to boneand transmit the force to generatemovement. Muscle and tendon injuriesaccount for a significant percentage ofthe over 100 million physician visitsin the US per year and this numberwill continue to rise as our populationages and remains active1. Previously,tendon injuries and disorders werealmost always considered tendonitis.Tendonitis is an inflammatory process,but recent research has shown that mostof the more chronic tendon problems donot have any inflammatory cells. Theprimary problem in these cases appearsto be a breakdown of the structuralproperties of the tendon collagen. Thusthe correct terminology for this problemis tendinopathy, as opposed to tendonitis.Tendinopathy results from overstressinga tendon. This can be from a singularacute bout of activity, or more often,from repetitive and sustained stressesover many months or even years. Itis possible for different areas of thetendon to be in different stages ofinjury or disorder2. Tendinopathy canultimately lead to chronic degradationof the tendon, and rarely, to the pointof tearing or rupture. There are manycurrent treatment options for thiscondition including, but not limited to,rest, anti-inflammatory medications(e.g., ibuprofen, naproxen), steroidinjections, physical therapy, shockwave therapy, dry needling and surgery.Recent advancements in regenerative(restoration and growth) medicine haveled to the development of platelet-richplasma (PRP) injections as a viabletreatment for various tendinopathies.What is Platelet-RichPlasma (PRP)?PRP is the concentration of plateletsderived from the plasma portion ofone’s own blood3. While platelets arewidely known to play a large rolein clotting processes, their use intreatment of tendon disease is dueto their abundance of enzymes andgrowth factors related to the healingprocess4,5. Tendons have a poor bloodsupply, meaning it is difficult for thesetissues to receive the nutrients needed tostimulate repair1,4,6. An injection of PRPto the injured site provides the tendontissue with healing growth factors thatare otherwise difficult for the bodyto deliver because of the poor bloodsupply. Similar mechanisms have beentheorized for treatment of ligamentinjuries such as medial collateralligament sprains of the knee or cartilagedeterioration, such as osteoarthritis ofthe knee7. The injection can also restarta healing inflammatory process, whichis why patients are often given initialactivity restrictions. Subsequent referralsto physical therapy are often made sothat patients may be taught to loadthe tissue in an appropriate fashion torebuild strength and flexibility.What does the PRPprocedure involve?PRP begins by collecting blood fromthe individual, usually by using asyringe and needle at the arm, similarto a clinic laboratory blood draw. Theamount of blood needed is determinedby the size of the area to be treatedand the concentration of plateletsdesired3. The blood is then placed ina centrifuge where the rapid spinningprocess separates the blood into 3components—the plasma or waterportion of the blood, the PRP layer,and the cellular layer containing redand white blood cells. The PRP layer isthen available for use in the clinic. Afterapplying a local anesthetic (numbingmedicine) to the site of the injection,the PRP is injected into the injuredtissue. Sometimes the injection isperformed in the radiology departmentso that the radiologist physicianmay view the area under ultrasoundguidance to ensure accurate placementof the injection. The patient is educatedabout activity restrictions and is oftengiven devices that limit the amount ofmovement at the area for the next fewdays. The patient is encouraged to restthe area for a few weeks, avoiding anyvigorous or strenuous activities, beforeThe health care team forthe UW Badgers and proudsponsor of UW Athletics6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
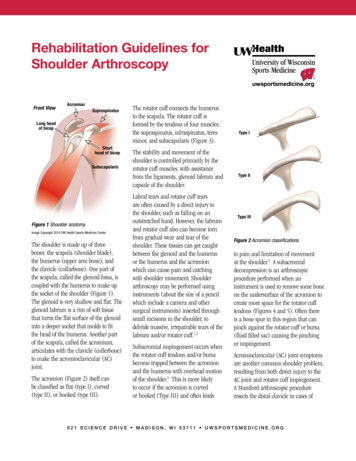
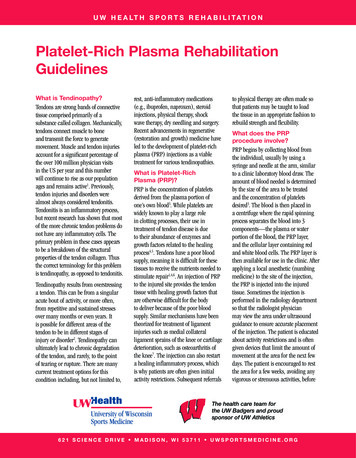
Platelet-Rich Plasma Rehabilitation Guidelinesbeginning the rehabilitation processtwo weeks following the procedure. Thepatient is typically seen by the physicianin the clinic for routine follow-up about1 month after the injection.range of motion. After the early phases,strengthening and neuromuscularcontrol exercises are emphasizedthroughout the affected extremity. In thefinal stages of rehabilitation, the focuswill be on progressive dynamic extremitycontrol and stability during sport specificmovements, such as change of directionand rotational movements.Do I need to do physicaltherapy and rehabilitationafter PRP?A quality post-procedure rehabilitationprogram helps facilitate a successfuloutcome. Initial rehabilitation will focuson protection for healing and gentleThe UW Health Sports Medicinerehabilitation guidelines beloware presented in a criterion basedprogression. General time frames aregiven for reference to the average, butindividual patients will progress atdifferent rates depending on their age,associated injuries, pre-injury healthstatus, rehabilitation compliance andinjury severity. These guidelines arepresented in reference to tendon-relatedprocedures, but general guidelinesand concepts apply with treatmentof ligamentous, joint, and musclepathologies.PRP Process:ABA: Collection of your own blood,B: Utilizing the centrifuge to separate the plateletsand growth factors from the blood,C: The separation of components into 2 vials,D: the injection of the platelet rich plasma to theaffected area.C2D6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
Platelet-Rich Plasma Rehabilitation GuidelinesPHASE I (0 to 3 days after procedure)Appointments No appointments during this time as rehabilitation appointments begin 10-14 daysafter procedureGoals Protection of the affected tendon Pain controlPrecautions Immobilization of the affected joint: Sling for rotator cuff / biceps tendons Wrist splint for medial / lateral epicondyles Partial weight bearing with crutches for patellar / quadriceps tendons Partial weight bearing with crutches and walking boot for Achilles / ankle tendons Partial weight bearing with crutches and walking boot for plantar fasciaSuggested TherapeuticExercises Gentle active range of motion (AROM) exercises out of the immobilizing deviceProgression Criteria 3 days after procedurePHASE II (3 to 10-14 days after procedure)3Appointments No appointments during this time as rehabilitation appointments begin 10-14 daysafter procedureGoals Increase tendon tolerance to daily activities Discontinue immobilizing devicePrecautions Weight bearing as tolerated, gradually weaning from assistive and immobilizaingdevices No overstressing of the tendon through exercise, lifting, or impact activitySuggested TherapeuticExercises Continue with active range of motion exercises out of the device 3 times a day for 5minutes a session. This will be described for you at your physician clinic visit. Lower body exercise for upper body procedures and upper body exercise for lowerbody procedures are allowed. Discuss these parameters with your physician,physical therapist or athletic trainer.Progression Criteria 10-14 days after procedure6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
Platelet-Rich Plasma Rehabilitation GuidelinesPHASE III ( 14 days after procedure to 6-8 weeks after procedure)4Appointments Rehabilitation appointments once every 1 to 2 weeks Physician clinic appointment 1 month after procedureRehabilitation Goals Attain full range of motion Improve strength and endurance Improve balance and proprioceptionPrecautions Avoid high velocity / amplitude / intensity exercise such as throwing, running,jumping, plyometrics or heavy weight lifting Avoid post-activity painSuggested TherapeuticExercises Stretching exercises for the affected muscle-tendon unit at least once a day, 3-4reps, holding for 20-30 seconds Joint mobilization as needed to restore normal joint mechanics Strengthening with emphasis on isometric and concentric activities initially andwith eccentric progression as symptoms allow: theraband drills for the rotator cuff,dumbbell exercises for the wrist and elbow, single leg press for the knee, heel raisesfor the ankle—3-4 sets of 6-12 reps at moderate intensity Balance and proprioception activities: joint reposition drills for the upper extremity;single leg stand and balance board drills for the lower extremity Core strengthening.Cardiovascular Exercises Non-impact activities with progressive resistance, duration, and intensity: upperbody ergometer, elliptical trainer, stationary bike, deep water runningProgression Criteria Full range of motionNo pain with activities of daily livingPain free 5/5 manual muscle testing of affected muscle-tendon unitSymmetric proprioception of the affected limb6 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r g
Platelet-Rich Plasma Rehabilitation GuidelinesPHASE IV (begin after meeting Phase III criteria, usually no sooner than 6-8 weeks afterprocedure)Appointments Rehabilitation appointments are approximately once every 1 to 3 weeks Physician clinic appointment 2-3 months after procedureRehabilitation Goals Good eccentric and concentric multi-plane strength and dynamic neuromuscularcontrol to allow for return to work/sportsPrecautions Post-activity soreness should resolve within 24 hoursSuggested TherapeuticExercises Continued strengthening of the affected area with increases in resistance, repetition,and / or frequency For the upper extremity: progressive training in provocative positions and work/sportspecific positions—including eccentric, endurance, and velocity specific exercises For the lower extremity: impact control exercises with progression from single planeto multi-planar landing and agility drills with progressive increase in velocity andamplitude Sport/work specific balance and proprioceptive drills Continued core strengthening Return to sport programs (throwing, running, etc.) with symptom / criteria basedprogressionsCardiovascular Exercises Replicate sport or work specific energy demandsProgression Criteria Return to sport/work criteria Good dynamic neuromuscular control with multi-plane activities and without pain Approval from the physician and/or sports rehabilitation providerThese rehabilitation guidelines were developed collaboratively between Ken Krogman, MSPT, ATC, Marc Sherry, PT, DPT LAT, CSCS,Dr. John Wilson and the UW Sports Medicine physician group.Updated 04/2014References1. Mishra A, et al. Treatment of Tendon andMuscle Using Platelet-Rich Plasma. ClinCports Med 2009; 28:113-125.2. Cook JL, et al. Is Tendon Pathology aContinuum? A Pathology Model to Explainthe Clinical Presentation of Load-InducedTendinopathy. Br J Sports Med 2009;43:409-416.3. Soomekh DJ, et al. Current Concepts forthe Use of Platelet-Rich Plasma in theFoot and Ankle. Clin Podiatr Med Surg2011; 28:155-170.4. Van Ark M, et al. Injections Treatments forPatellar Tendinopathy. Br J Sports Med.2011; 45:1068-1076.6. Sanchez M, et al. Platelet-Rich Therapiesin the Treatment of Orthopedic SportInjuries. Sports Med 2009; 39(5):345-354.7. Nguyen RT, et al. Applications of PlateletRich Plasma in Musculoskeletal andSports Medicine: An Evidence-BasedApproach. PM R 2011; 3:226-250.5. De Vos RJ, et al. Autologous GrowthFactor Injections in Chronic Tendinopathy:A Systematic Review. British MedicalBulletin 2010; 95:63-77.Copyright 2014 UW Health Sports Medicine Center56 2 1 S c i e n c e D r i v e M a d i s o n , W I 5 3 7 1 1 u ws p o r t sm e d i c i n e . o r gSM-39275-14At UW Health, patients may have advanced diagnostic and /or treatment options, or may receive educational materials that vary from this information. Please be aware that this information is not intended to replacethe care or advice given by your physician or health care provider. It is neither intended nor implied to be a substitute for professional advice. Call your health provider immediately if you think you may have a medicalemergency. Always seek the advice of your physician or other qualified health provider prior to starting any new treatment or with any question you may have regarding a medical condition.
minutes a session. This will be described for you at your physician clinic visit. Lower body exercise for upper body procedures and upper body exercise for lower body procedures are allowed. Discuss these parameters with your physician, physical therapist or athletic trainer. Progression Criteria 10-14 days after procedure