Transcription
Physiology and Anatomy ofBlood VesselsPrepared byDr. Naim Kittana, PhDAn-Najah National UniversityFaculty of Medicine and Health SciencesDepartment of Biomedical Sciences
Disclosure The material and the illustrations are adopted from thetextbook “Human Anatomy and Physiology / Ninth edition/Eliane N. Marieb 2013”Dr. Naim Kittana, PhD2
Blood vessels Blood is carried in a closed system of vessels that beginsand ends at the heart The three major types of vessels are arteries, capillaries,and veins Arteries carry blood away from the heart, veins carry bloodtoward the heart Capillaries contact tissue cells and directly serve cellularneedsDr. Naim Kittana, PhD3
Structure of Blood Vessel Walls The walls of all blood vessels, except small capillaries, havethree distinct layers, or tunics (“coverings”), that surround acentral blood-containing space, the vessel lumenDr. Naim Kittana, PhD4
simplesquamousepitheliumsmoothmuscle tissueBlood Vessel StructureconnectivetissueDr. Naim Kittana, PhD5
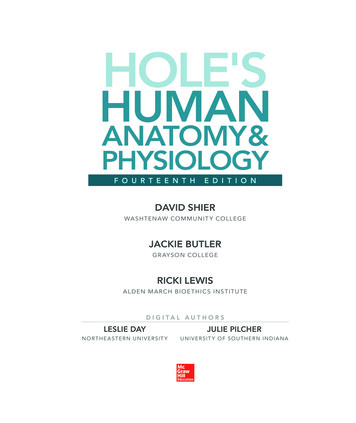
Tunica intima Endothelium Subendothelial layerInternal elastic laminaTunica media(smooth muscle andelastic fibers)External elastic laminaTunica externa(collagen sement membraneEndothelial cellsCapillaryDr. Naim Kittana, PhD6
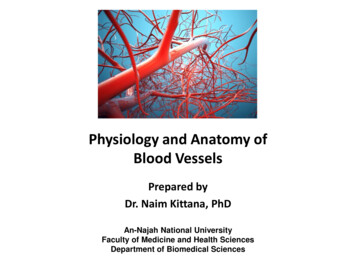
Structure of Blood Vessel WallsArteryVeinDr. Naim Kittana, PhD7
TunicsTunica interna (tunica intima)– Endothelial layer that lines the lumen of all vessels– In vessels larger than 1 mm in diameter, a subendothelialconnective tissue basement membrane is presentTunica media– Smooth muscle and elastic fiber layer, regulated bysympathetic nervous system– Controls vasoconstriction/vasodilation of vesselsDr. Naim Kittana, PhD8
TunicsTunica externa (tunica adventitia)– Collagen fibers that protect and reinforce vessels Larger vessels contain vasa vasorum: system of tiny bloodvessels vessels of the vessels”—that nourish the moreexternal tissues of the blood vessel wallDr. Naim Kittana, PhD9
ArteryveinDr. Naim Kittana, PhD10
Venous systemArterial systemThe relationshipHeartof blood vesselsto each otherand to lymphaticvessels11Dr. Naim Kittana, PhD
Arteries1. Carry blood away from the heart.2. Thick-walled to withstand hydrostatic pressure of the bloodduring ventricular systole.3. Blood pressure pushes blood through the vesselDr. Naim Kittana, PhD12
Elastic (Conducting) d arteries near the heart;the aorta and its major branches– Large lumen allow lowresistance conduction of blood– Contain elastin in all three tunics– Withstand and smooth out largeblood pressure fluctuations– Allow blood to flow fairlycontinuously through the bodyDr. Naim Kittana, PhD13
Muscular (Distributing) Arteries and ArteriolesVenoussystemMuscular arteries – distal toelastic arteries; deliver blood tobody organs– Have thick tunica mediawith more smooth muscleand less elastic tissue– Active in vasoconstrictionDr. Naim Kittana, PhDArterialsystemHeart14
ArteriolesVenoussystem- The smallest arteries- Lead to capillary beds- Control flow into capillary bedsvia vasodilation andconstrictionDr. Naim Kittana, PhDArterialsystemHeart15
CapillariesCapillaries are the smallest blood vessels– Walls consisting of a thin tunica interna, one cell thick– Allow only a single RBC to pass at a time– Pericytes on the outer surface stabilize their wallsThere are three structural types of capillaries: continuous,fenestrated, and sinusoidsDr. Naim Kittana, PhD16
Capillaries Average capillary length is 1 mm and average lumendiameter is 8–10 μm, just large enough for red bloodcells to slip through in single file.Dr. Naim Kittana, PhD17
Most tissues have a rich capillary supply, but there areexceptions.- Tendons and ligaments are poorly vascularized.- Cartilage lack capillaries, but receive nutrients from bloodvessels in nearby connective tissues,- The avascular cornea and lens of the eye receive nutrientsfrom the aqueous humor.Dr. Naim Kittana, PhD18
Capillaries There are three structural types of capillaries: Continuous Fenestrated SinusoidsDr. Naim Kittana, PhD19
Continuous CapillariesContinuous capillaries are abundant in the skin and muscles,and have:– Endothelial cells that provide an uninterrupted lining– Adjacent cells that are held together with tightjunctions– these junctions are usually incomplete and leave gapsof unjoined membrane called intercellular clefts– Intercellular clefts are just large enough to allowlimited passage of fluids and small solutesDr. Naim Kittana, PhD20
Continuous CapillariesDr. Naim Kittana, PhDFigure 19.3a21
Continuous CapillariesThe unique continuous capillaries of the brain:– The tight junctions of the continuous capillaries arecomplete and extend around the entire perimeter of theendothelial cells, constituting the structural basis of theBlood Brain Barrier22
Fenestrated Capillaries Found wherever active capillary absorption or filtrateformation occurs (e.g., small intestines, endocrine glands,and kidneys) Characterized by:– An endothelium riddled with pores (fenestrations)– Greater permeability to solutes and fluids than othercapillaries23
Sinusoid Capillaries (Sinusoids) Highly modified, leaky, fenestrated capillaries with largelumens Found in the liver, bone marrow, lymphoid tissue, and insome endocrine organs Allow large molecules (proteins and blood cells) to passbetween the blood and surrounding tissues Their endothelial lining has fewer tight junctions andlarger intercellular clefts than ordinary capillariesDr. Naim Kittana, PhD24
Sinusoid Capillaries (Sinusoids)Dr. Naim Kittana, PhD25
Capillary Beds A microcirculation of interweaving networks of capillaries,consisting of:– Vascular shunts: metarteriole– thoroughfare channelconnecting an arteriole directly with a postcapillaryvenule– True capillaries – 10 to 100 per capillary bed, capillariesbranch off the metarteriole and return to thethoroughfare channel at the distal end of the bedDr. Naim Kittana, PhD26
PrecapillarysphinctersTerminal arterioleVascular shuntMetarterioleThoroughfare channelTrue capillariesPostcapillary venule(a) Sphincters open—blood flows through true capillaries.Terminal arteriolePostcapillary venule(b) Sphincters closed—blood flows through metarteriolethoroughfare channel and bypasses true capillaries.Dr. Naim Kittana, PhD27
Veins Carry blood to the heart.Thinner-walled than arteries.Possess one-way valves that prevent backwards flow of blood.Blood flow due to body movements, not from blood pressure.Dr. Naim Kittana, PhD28
One-Way Valves in VeinsValve (open)Valve (closed)VeinDr. Naim Kittana, PhD29
Relative proportion of blood volume throughout thecardiovascular systemDr. Naim Kittana, PhD30
Vascular Anastomoses Blood vessels form special interconnections Most organs receive blood from more than one arterialbranch They provide alternate pathways, called collateral channels,for blood to reach a given body region They are also common in abdominal organs, the heart, andthe brainDr. Naim Kittana, PhD31
Physiology of CirculationDr. Naim Kittana, PhD32
Blood Flow Blood flow is the volume of blood flowing through a vessel, anorgan, or the entire circulation in a given period (ml/min). If we consider the entire vascular system, blood flow isequivalent to cardiac output (CO),Dr. Naim Kittana, PhD33
Blood pressure (BP)– Force per unit area exerted on the wall of a blood vessel bythe blood Expressed in mm Hg Measured as systemic arterial BP in large arteries nearthe heart– The pressure gradient provides the driving force that keepsblood moving from higher to lower pressure areasDr. Naim Kittana, PhD34
Resistance (peripheral resistance)– Opposition to flow– Measure of the amount of friction blood encounters– Generally encountered in the peripheral systemic circulationThree important sources of resistance– Blood viscosity– Total blood vessel length– Blood vessel diameterDr. Naim Kittana, PhD35
Systemic Blood Pressure Any fluid driven by a pump through a circuit of closed channelsoperates under pressure, and the nearer the fluid is to thepump, the greater the pressure exerted on the fluidDr. Naim Kittana, PhD36
Systemic Blood Pressure The pumping action of the heart generates blood flow Pressure results when flow is opposed by resistance Systemic pressure– Is highest in the aorta– Declines throughout the pathway– Is 0 mm Hg in the right atrium The steepest drop occurs in arteriolesDr. Naim Kittana, PhD37
Systolic pressureMean pressureDiastolicpressureblood pressure is pulsatile—it rises and falls in a regularfashion—in the elastic arteries near the heart.Dr. Naim Kittana, PhD38
ResistanceFactors that remain relatively constant:– Blood viscosityThe “stickiness” of the blood due to formed elements andplasma proteins– Blood vessel lengthThe longer the vessel, the greater the resistanceencounteredDr. Naim Kittana, PhD39
Resistance Small-diameter arterioles are the major determinants ofperipheral resistance Abrupt changes in diameter or fatty plaques from atherosclerosisdramatically increase resistance– Disrupt laminar flow and cause turbulence Resistance varies inversely to vessel radiusDr. Naim Kittana, PhD40
Venous Blood Pressure Arterial pressure pulsates with each contraction of the leftventricle Venous blood pressure is steady and changes very little duringthe cardiac cycle. The pressure gradient in the veins, from venules to thetermini of the venae cavae, is about 15 mm Hg The pressure gradient in the arteries gradient from the aortato the ends of the arterioles is about 60 mm Hg. Venous pressure is normally too low to promote adequatevenous returnDr. Naim Kittana, PhD41
Systolic pressureMean pressureDiastolicpressureblood pressure is pulsatile—it rises and falls in a regularfashion—in the elastic arteries near the heart.Dr. Naim Kittana, PhD42
Factors contributing to venous return: The muscular pump: As the skeletal musclessurrounding the deepveins contract and relax,they “milk” blood towardthe heart Once blood passes eachsuccessive valve, it cannotflow backDr. Naim Kittana, PhD43
Factors contributing to venous return: The respiratory pump As we inhale, abdominal pressure increases, squeezing localveins and forcing blood toward the heart. At the same time, the pressure in the chest decreases,allowing thoracic veins to expand and speeding blood entryinto the right atrium.Dr. Naim Kittana, PhD44
Factors contributing to venous return: Sympathetic venoconstriction: Reduces the volume of blood in the veins—the capacitancevessels venous volume is reduced and blood is pushedtoward the heart.Dr. Naim Kittana, PhD45
Factors influencing blood pressureFillingpressureBlood volumeVenous toneCardiacoutputHeart rateContractilityArterial VascularfunctionDr. Naim Kittana, PhD46
Baroreceptor reflex arcDr. Naim Kittana, PhD47
48Direct and indirect (hormonal)mechanisms for renal control of bloodpressure
Factors that increase Mean arterial pressure (MAP)49
Superficial Pulse Points- arteries, not veinstemporal60 steriortibialfemoral Temporal arteryFacial arteryCommon carotid arteryBrachial arteryRadial arteryFemoral arteryPopliteal arteryPosterior tibial arteryDorsal pedis arteryDorsal pedisDr. Naim Kittana, PhD50
Homeostatic Imbalances Tachycardia: abnormally fast heart rate ( 100 bpm)– If persistent, may lead to fibrillation Bradycardia: heart rate slower than 60 bpm– May result in grossly inadequate blood circulation– May be desirable result of endurance trainingDr. Naim Kittana, PhD51
Circulatory Shock Any condition in which– Blood vessels are inadequately filled– Blood cannot circulate normally Results in inadequate blood flow to meet tissue needsDr. Naim Kittana, PhD52
Classification of Circulatory Shock Hypovolemic shock: results from large-scale blood loss Vascular shock: results from extreme vasodilation anddecreased peripheral resistance Cardiogenic shock: results when an inefficient heartcannot sustain adequate circulationDr. Naim Kittana, PhD53
Hypertension Hypertension (HTN) results fromincreased peripheral vasculararteriolar smooth muscle toneleading to increased arteriolarresistance and reducedcapacitance of the venoussystem. The cause of elevated vasculartone is unknown HTN is a risk factor for chronickidney disease, MI, heart failure,stroke and blindnessDr. Naim Kittana, PhD54
Etiology of HTN Essential HTN: 90% of patients with unknown cause Predisposing factors: diabetes, obesity, stressful lifestyle, highintake of sodium, smoking , race, and family historyClassification of Blood PressureSystolic mm HgDiastolic mm HgNormal 120and 80Pre-hypertensive120-139or80-90Stage I140-159or90-99Stage II 160or 100Hypertensiveemergency 180or 12055Dr. Naim Kittana, PhD
Physiology and Anatomy of Blood Vessels Prepared by Dr. Naim Kittana, PhD An-Najah National University Faculty of Medicine and Health Sciences Department of Biomedical Sciences . The material and the illustrations are adopted from the textbook "Human Anatomy and Physiology / Ninth edition/