Transcription
Pre and PostExposureProphylaxis forHIVNatella Rakhmanina, MD, PhDProfessor of PediatricsGeorge Washington UniversitySenior Technical AdvisorElizabeth Glaser Pediatric AIDSFoundation
HIV Infection Sources Exposureto HIV-infected blood, genitalsecretions, rectal secretions, breast milk orother bodily fluid visibly contaminated withblood through: unprotected sex protected sex with condom failure intravenous drug use sexual assault selected oral mucosa and skin exposures
Estimated Risks for HIVTransmission, USATypes of exposureEstimated RiskNeedle-sharing exposure to aninfected source0.67% (1 in 150)Receptive anal intercourse withan infected source0.5% (1 in 200) / 3.0% (6 in 200)Receptive vaginal intercourse with 0.1% (1 in 1000) / 0.2% (2 in 1000)an infected sourceInsertive anal intercourse with aninfected source0.065% (1 in 1500)Insertive vaginal intercourse withan infected source0.05% (1 in 2000)Oral sex with ejaculation with aninfected sourceConflicting data-however, risk isconsidered to be lowNew York State Department of Health AIDS Institute: HIV Prophylaxis following Non-Occupational Exposure. Albany, NY:Available at: xposure.pdf.
Estimated Risks for HIVTransmission, BHIVA-BASHH,UK
Pre-Exposure Prophylaxis (PreP) Preventionof mother-to-childtransmission (PMTCT)- gold standard- 98% efficient! Occupational PreP Non-occupational PreP
PreP QuizThe most effective non-occupational PrEP is(select one correct answer):a.b.c.d.e.Not to have sexNot to have sexNot to have sexNot to have sexAll of the above
USABHIVABASHH, UK
PreP Approaches Personsat high risk for HIV based onbackground incidence ( 2%) or recentdiagnosis of incident STI Individuals who have used PEP 2 times in thepast year People who inject drugs and who shareinjection equipment, inject 1 or more times aday, or inject cocaine or methamphetamines PreP should be part of an integrated riskreduction strategy Regular assessment of the patients’ risk isrequired
PreP CDC GuidelinesPreP should be considered for: Sexually-active adult MSM (men who have sexwith men) at substantial risk of HIV acquisition(IA) Adult heterosexually active men and womenwho are at substantial risk of HIV acquisition (IA) Adult injection drug users (IDU) at substantial riskof HIV acquisition (IA) Heterosexually-active women and men whosepartners are known to have HIV infection (i.e.,HIV-discordant couples) consideringconception and pregnancy (IIB)Preexposure Prophylaxis for the Prevention of HIVInfection in the US, 2014 Clinical Practice Guideline
PreP in the USA Asthe first country to approve PrEP in 2012, USAhas the most experience to date on PrEPimplementation PrEPprescriptions in the US show very lowinitiation of PrEP among youth 25 years - 7.6%of all prescriptions
PreP Choice Daily oral PrEP with the fixed-dose combination ofTenofovir Disoproxil Fumarate (TDF) Emtricitabine(FTC) (Truvada ) - safe and effective in reducingthe risk of sexual HIV acquisition in adultsAcute and chronic HIV infection must be excludedby symptom history and HIV testing immediatelybefore PrEP is prescribedHIV infection should be assessed at least every 3months while patients are using PrEPRenal function should be assessed at baseline andmonitored at least every 6 months while on PrEP
Sweden – TAF for PreP
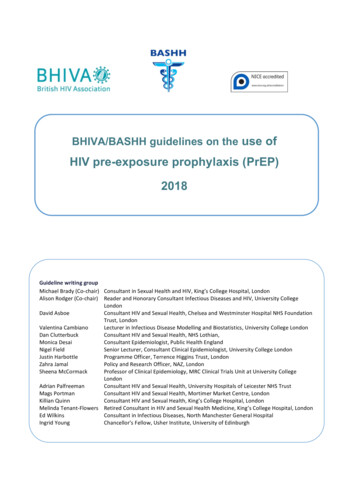
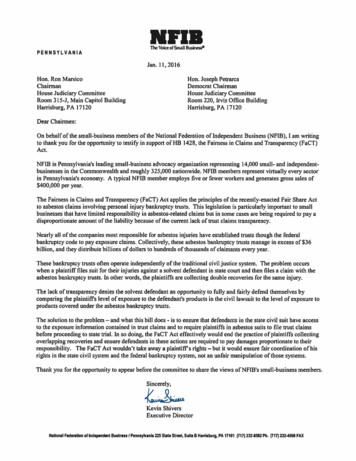
Gender matters! Tobuild up to protective levels, PrEP takes20 days in vaginal tissue versus only 7 daysin rectal tissue20 days forvaginal protection7 days forrectal protection
Truvada (TDF/FTC) for PrePJ Int AIDS So.j Int AIDS Soc. 2016; 19(7Suppl 6): 21107.
PreP for Adolescents oCurrently the data on the efficacy and safety of PrEP foradolescents 18 years are limitedRegistration trials on the way in the USA and South Africa forpatients 18 yrs of age:ATN 113 (Clinical trial NCT01769456), USA, MSM aged 15-17 yrsCHAMPS PillsPlus (Clinical trials NCT02213328), South Africa,females and males 5-19 years of ageHIV Prevention Trials Network (HPTN) 082, women and males16-25 yrs in South Africa and ZimbabweIMPAACT 2009, adolescents and women, South Africa,Zimbabwe, Malawi, and Uganda including 18 years of ageThe behavioral intervention as well as ongoing risk reductioncounseling sessions have been found to be highly acceptableamong a sample of racially diverse YMSM (J HIV AIDS Soc Serv2013;12(3-4))
PreP Considerations inAdolescents 18 years old horizontally infected MSM with history ofsustained non-adherence, profound immunesuppression, high viremia, untreated perianal wartsbrings in partner of 2 years for PreP discussion17 years old perintally infected young woman withexcellent control of her disease and undetectableviremia, on oral contraceptives presents with her HIVnegative boyfriend to discuss if they can stop usingcondoms19 years old young woman who has a relationship with19 years old young man living with HIV who hasintermittent adherence and moderate degree of HIVviremia, tells you that she wants to have his baby* All scenarios are adapted from real clinical situations
Challenges and Opportunities Registration/Insurancecoverage Provider/patient readiness/comfort Repeat HIV and toxicity testing Adherence/compliance support Viral resistance testing requirements Comprehension prevention package
Do it Right DC
Hot Line rep-pre-exposure-prophylaxis/
Post Exposure Prophylaxis - PEPPEP considered for following exposures: Occupational(OPEP) Non-occupational (NPEP)
Examples of NPEP in Pediatric Practice 17 years old boy tells his mother that he was atthe private tattoo party yesterday, where needlewas reused, and now has two new tattoos18 years old girl reports that she was raped bylast night by her older cousin and she just heardthat he might be HIV positive14 years old boy is referred because there aremultiple syringes with needles found at homefrom his visiting uncle who is using IV drugs daily,he has been stuck by one of them this morning* All scenarios are adapted from real clinical situations
CDC PEP Guidelines, 2016
NPEP Guidelines Tenofovir Emtricitabine(Truvada ) plusRaltegravir or Dolutegravir - need to bestarted within 72 hours after exposure!!!! Superior effectiveness of three drugs inreducing chances for viral replicationand establishment of reservoir Concerns about HIV drug resistance tocommonly used HIV medications*CDC HIV Postexposure Guidelines, 2016.
Conclusions Thoroughhistory and evaluation of riskfactors are crucial for PreP Individualized approach is veryimportant PEP and PreP both require close followup and repeat testing and evaluations Recurrent PEP and PreP both needenhanced counseling on risk reduction
PrEP and SexualHealth EducationVeronica Urquilla, MSWDC Department ofHealth/HAHSTAYouth and Young Adults STDPrograms Manager
Why are we teaching this tostudents? Purpose of health education is to promotepositive health behaviorsSexual health education should providestudents with all the options they can choosefrom to stay healthyPatient and their clinician will decide if PrEP isright for them- so educate all youth about itPrEP is a highly effective tool in preventing HIVtransmissionHigh rates of STIs indicate youth are havingunprotected sex
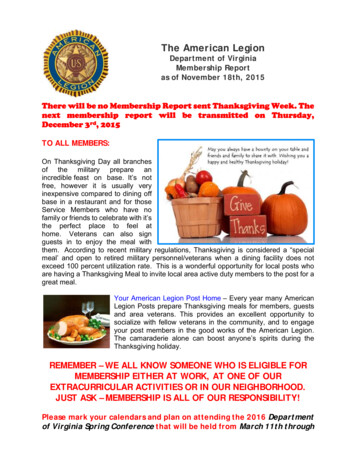
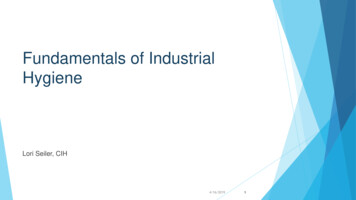
Reported Number of Chlamydia Cases by Year of Reportand Age at Diagnosis2011201220131,0181,5132014Year of 812,500165Number of Reported Cases3,0002,737District of Columbia, 2011-20152015
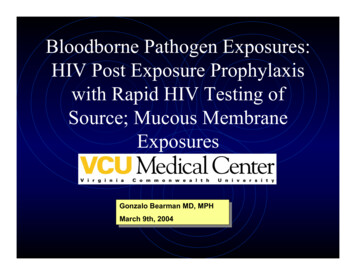
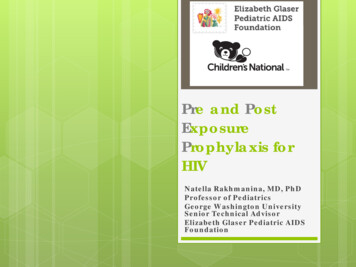
Reported Number of Gonorrhea Cases by Year of Reportand Age at DiagnosisDistrict of Columbia, 201220132014Year of Report0- 1415-1920-2425-29144113204384911004220052Number of Cases Reported9008738141,0002015
Where do I fit PrEP into healtheducation?
MS Category 3: Human Body andPersonal Health AccessingInformation3.3.13Identify school,medical, andcommunity basedsupport services forsexual healthservices, includingSTI/HIV testing/treatment,contraception, andabortion. Decision Making3.5.17Analyze the short-termand long-termconsequences ofadolescent sexualactivity including thevarious costs of STI/HIVtesting/ treatment,unplanned pregnancy,and parenting.
MS Category 3: Human Bodyand Personal Health Healthy Behaviors 3.7.27**Define and describe STI/HIV, protectionmethods (e.g., male/insertive andfemale/receptive condoms; dental dams;finger cots; and PreExposure Prophylaxis),symptoms, confidential testing, treatment,risks, and modes of transmission.
High School Category 3 AccessingInformation3.3.14Identify and locatecommunity healthclinics, private healthclinics, urgent carefacilities and hospitalemergency rooms.Analyze the cost andaccessibility thereof. Communication3.4.17Adapt healthmessages andcommunicationtechniques to promoteprevention, treatment,and testing for STIs andHIV for high schoolaged youth.
High School Category 3 Healthy BehaviorsDecision Making 3.5.19Demonstrate the abilityto select professionalhealth services basedon the type of careneeded, the nature ofthe problem, and thekinds of questions thatneed answeringIdentify andrecommend behaviorsthat enhance andsupport the optimalfunctioning of bodilysystems, including thefunctions of the body’simmune system3.7.23
Advocacy3.8.28 Research DC minorconsent laws,compare andcontrast these lawsto other states, anddescribe adolescentsexual health rightsgenerally Advocacy3.8.29 Analyze the data onSTI and HIV ratesamong youth.Discuss barriers toprevention, testing,and treatmentincluding legal,economic, andcultural barriers.
Examples Have students use the PrEP locator to findlocations near themBrainstorm benefits and barriers to taking a pilleverydayReview PrEP studiesDon’t set PrEP aside integrate it into discussionaround preventionDiscussion possible progression from PrEP pillsimilar to oral contraception to other forms ofbirth control ( depo, nuva ring, IUD withhoromone)
Need some help? Learn more about ov/hiv/basics/prep.html DOH,CNMC, Planned Parenthood andother community based organizationscan help with introducing PrEP to youth
Thank you!
Individuals who have used PEP 2 times in the past year People who inject drugs and who share injection equipment, inject 1 or more times a day, or inject cocaine or methamphetamines PreP should be part of an integrated risk-reduction strategy Regular assessment of the patients' risk is required