Transcription
2020 ACC/AHA Guideline for the Managementof Patients with Valvular Heart DiseaseDeveloped in collaboration with and endorsed by the American Association forThoracic Surgery, American Society of Echocardiography, Society forCardiovascular Angiography and Interventions, Society of CardiovascularAnesthesiologists, and Society of Thoracic Surgeons
Citation This slide set is adapted from the 2020 ACC/AHA Guideline for the Management ofPatients with Valvular Heart Disease. Published on Dec 17, 2020, available at: Journalof the American College of Cardiology J Am Coll Cardiol. Dec 17, 2020. Epublished DOI:10.1016/j.jacc.2020.11.018 and Circulation. doi: 10.1161/CIR.0000000000000923 The full-text guidelines are available on the ACC website 020.11.018 and the AHA website 000000000000923
2020 Writing Committee Members*Catherine M. Otto, MD, FACC, FAHA, Co-ChairRick A. Nishimura, MD, MACC, FAHA, Co-ChairRobert O. Bonow, MD, MS, MACC, FAHAChristopher McLeod, MBCHB, PhD, FAHABlasé A. Carabello, MD, FACC, FAHAPatrick O’Gara, MD, MACC, FAHA†John P. Erwin III, MD, FACC, FAHAVera H. Rigolin, MD, FACC, FAHAFederico Gentile, MD, FACCThoralf M. Sundt III, MD, FACC, FAHAHani Jneid, MD, FACC, FAHAAnnemarie Thompson, MDEric V. Krieger, MD, FACCChristopher ToleyMichael Mack, MD, MACC*Writing committee members are required to recuse themselves from voting on sections to which their specific relationships with industrymay apply; see Appendix 1 for detailed information. †ACC/AHA Representative. †ACC/AHA Joint Committee on Clinical PracticeGuidelines Liaison.3
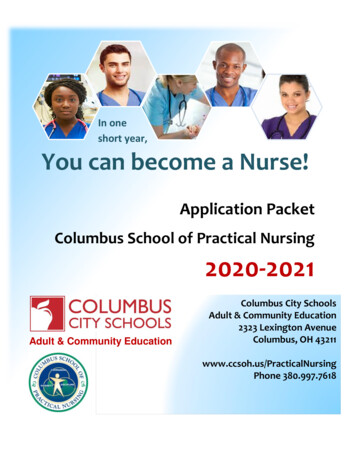
Table 2. ACC/AHA Applying Class ofRecommendation and Level ofEvidence to Clinical Strategies,Interventions, Treatments, orDiagnostic Testing in Patient Care(Updated May 2019)*4
Top 10 Take-Home Messages2020 Valvular Heart Disease Guidelines5
Top 10 Take Home Messages1. Disease stages in patients with valvular heartdisease should be classified (Stages A, B, C,and D) on the basis of symptoms, valveanatomy, the severity of valve dysfunction,and the response of the ventricle andpulmonary circulation.6
Top 10 Take Home Messages2. In the evaluation of a patient with valvular heart disease, history andphysical examination findings should be correlated with the results ofnoninvasive testing (i.e., ECG, chest x-ray, transthoracicechocardiogram). If there is discordance between the physicalexamination and initial noninvasive testing, consider further noninvasive(computed tomography, cardiac magnetic resonance imaging, stresstesting) or invasive (transesophageal echocardiography, cardiaccatheterization) testing to determine optimal treatment strategy.7
Top 10 Take Home Messages3. For patients with valvular heart disease and atrial fibrillation (exceptfor patients with rheumatic mitral stenosis or a mechanicalprosthesis), the decision to use oral anticoagulation to preventthromboembolic events, with either a vitamin K antagonist or a non–vitamin K antagonist anticoagulant, should be made in a shareddecision-making process based on the CHA2DS2-VASc score. Patientswith rheumatic mitral stenosis or a mechanical prosthesis and atrialfibrillation should have oral anticoagulation with a vitamin Kantagonist.8
Top 10 Take Home Messages4. All patients with severe valvular heartdisease being considered for valveintervention should be evaluated by amultidisciplinary team, with either referralto or consultation with a Primary orComprehensive Valve Center.9
Top 10 Take Home Messages5. Treatment of severe aortic stenosis with either atranscatheter or surgical valve prosthesis should bebased primarily on symptoms or reduced ventricularsystolic function. Earlier intervention may beconsidered if indicated by results of exercise testing,biomarkers, rapid progression, or the presence ofvery severe stenosis.10
Top 10 Take Home Messages6. Indications for transcatheter aortic valve implantation areexpanding as a result of multiple randomized trials oftranscatheter aortic valve implantation atrio versus surgicalaortic valve replacement. The choice of type of intervention fora patient with severe aortic stenosis should be a shared decisionmaking process that considers the lifetime risks and benefitsassociated with type of valve (mechanical versus bioprosthetic)and type of approach (transcatheter versus surgical).11
Top 10 Take Home Messages7. Indications for intervention for valvular regurgitationare relief of symptoms and prevention of theirreversible long-term consequences of leftventricular volume overload. Thresholds forintervention now are lower than they werepreviously because of more durable treatmentoptions and lower procedural risks.12
Top 10 Take Home Messages8. A percutaneous edge-to-edge mitral repair is ofbenefit to patients with severely symptomatic primarymitral regurgitation who are at high or prohibitive riskfor surgery, as well as to a select subset of patientswith severely symptomatic secondary mitralregurgitation despite guideline-directed managementand therapy for heart failure.13
Top 10 Take Home Messages9. Patients presenting with severe symptomatic isolatedtricuspid regurgitation, commonly associated withdevice leads and atrial fibrillation, may benefit fromsurgical intervention to reduce symptoms andrecurrent hospitalizations if done before the onset ofsevere right ventricular dysfunction or end-organdamage to the liver and kidney.14
Top 10 Take Home Messages10. Bioprosthetic valve dysfunction may occurbecause of either degeneration of the valveleaflets or valve thrombosis. Catheter-basedtreatment for prosthetic valve dysfunction isreasonable in selected patients for bioprostheticleaflet degeneration or paravalvular leak in theabsence of active infection.15
General Principles16
Table 3. Evaluation of Patientswith Known or Suspected VHDReasonInitial evaluation: AllTestTTE*IndicationEstablishes chamber size and function, valve morphologyand severity, and effect on pulmonary and systemicpatients with known orsuspected valve diseasecirculationHistory andEstablishes symptom severity, comorbidities, valve diseasephysicalpresence and severity, and presence of HFECGEstablishes rhythm, LV function, and presence or absence ofhypertrophy*TTE is the standard initial diagnostic test in the initial evaluation of patients with known or suspected VHD17
Table 3. Evaluation of Patientswith Known or Suspected VHDReasonFurther diagnostic testing: InformationTestChest x-rayIndicationImportant for the symptomatic patient; establishes heart size andrequired for equivocal symptom status,presence or absence of pulmonary vascular congestion, intrinsicdiscrepancy between examination andlung disease, and calcification of aorta and pericardiumechocardiogram, further definition of valveTEEProvides high-quality assessment of mitral and prosthetic valve,disease, or assessing response of the ventriclesincluding definition of intracardiac masses and possible associatedand pulmonary circulation to load and toabnormalities (e.g., intracardiac abscess, LA thrombus)exerciseCMRProvides assessment of LV volumes and function, valve severity,and aortic disease18
Table 3. Evaluation of Patientswith Known or Suspected VHDReasonFurther diagnostic testing:TestPET CTInformation required for equivocalsymptom status, discrepancy betweenIndicationAids in determination of active infection orinflammationStress testingGives an objective measure of exercise capacityCatheterizationProvides measurement of intracardiac and pulmonaryexamination and echocardiogram,further definition of valve disease, orassessing response of the ventricles andpulmonary circulation to load and topressures, valve severity, and hemodynamic response toexercise and drugsexercise19
Table 3. Evaluation of Patientswith Known or Suspected VHDReasonTestIndicationFurther risk stratification: Biomarkers Provide indirect assessment of filling pressures andmyocardial damageInformation on future risk ofthe valve disease, which isTTE strainHelps assess intrinsic myocardial performanceCMRAssesses fibrosis by gadolinium enhancementimportant for determinationof timing of intervention20
Table 3. Evaluation of Patientswith Known or Suspected VHDReasonFurther risk stratification:TestStress testingIndicationProvides prognostic markersInformation on future risk ofthe valve disease, which isProcedural risk Quantified by STS (Predicted Risk of Mortality) andTAVI scoresimportant for determination oftiming of interventionFrailty scoreProvides assessment of risk of procedure and chance ofrecovery of quality of life21
Table 3. Evaluation of Patientswith Known or Suspected VHDReasonPreprocedural testing:TestIndicationDental examinationRules out potential infection sourcesCT coronary angiogram or invasive coronaryProvides an assessment of coronary anatomyTesting required beforevalve interventionangiogramCT: peripheralAssess femoral access for TAVI and other transcatheterproceduresCT: cardiacAssesses suitability for TAVI and other transcatheterproceduresCMR indicates cardiac magnetic resonance; CT, computed tomography; ECG, electrocardiogram; HF, heart failure; LV, left ventricular; PET, positronemission tomography; STS, Society of Thoracic Surgeons; TAVI, transcatheter aortic valve implantation; TEE, transesophageal echocardiography;TTE, transthoracic echocardiography; and VHD, valvular heart disease.22
Table 4. Stages of VHDStageDefinitionDescriptionAAt riskPatients with risk factors for development of VHDBProgressivePatients with progressive VHD (mild to moderate severity and asymptomatic)CAsymptomaticAsymptomatic patients who have the criteria for severe VHD:severeC1: Asymptomatic patients with severe VHD in whom the LV or RV remainscompensated spaceC2: asymptomatic patients with severe VHD with decompensation of LV or RVDSymptomatic severe Patients who have developed symptoms as a result of VHD23
Diagnosis and Follow-up24
Diagnostic Testing: Routine Follow-upTable 5. Frequency of Echocardiograms in Asymptomatic Patients with VHD and Normal LV FunctionType of Valve LesionStageAortic Stenosis*Aortic RegurgitationMitral StenosisMitral RegurgitationProgressive Every 3–5 y (mild Every 3–5 y (mildEvery 3–5 y Every 3–5 y (mild severity)(Stage B)severity; Vmax 2.0–2.9severity)(MV area 1.5 cm2)m/s) Every 1–2 y moderateseverity; Vmax 3.0–3.9 Every 1–2 y (moderateseverity) Every 1–2 y (moderateseverity)m/s)Patients with mixed valve disease may require serial evaluations at intervals earlier than recommended for single-valve lesions. Theseintervals apply to most patients with each valve lesion and do not take into consideration the etiology of the valve disease.*With normal stroke volume.25
Diagnostic Testing: Routine Follow-upTable 5. Frequency of Echocardiograms in Asymptomatic Patients with VHD and Normal LV FunctionType of Valve LesionStageAortic Stenosis*Aortic RegurgitationMitral StenosisSevere Every 6–12 mo Every 6–12 mo Every 1–2 y (MV area 1.0– Every 6–12 moasymptomatic (Vmax 4 m/s)Mitral Regurgitation1.5 cm2)(Stage C1) Dilating LV: Morefrequently Every year (MV area 1.0Dilating LV: More frequentlycm2)Patients with mixed valve disease may require serial evaluations at intervals earlier than recommended for single-valve lesions. Theseintervals apply to most patients with each valve lesion and do not take into consideration the etiology of the valve disease.*With normal stroke volume.26
Basic Principles of Medical Therapy27
Secondary Prevention of Rheumatic FeverCOR LOERecommendation1. In patients with rheumatic heart disease,1C-EOsecondary prevention of rheumatic feveris indicated.
Table 6. Secondary Prevention ofRheumatic FeverAntibiotics for PreventionDosage‡Penicillin G benzathine1.2 million U intramuscularly every 4 wk*Penicillin V potassium200 mg orally twice dailySulfadiazine1 g orally once dailyMacrolide or azalide antibiotic (for patients allergic toVariespenicillin and sulfadiazine)†‡ In patients with documented valvular heart disease, the duration of rheumatic fever prophylaxis should be 10 years or until the patient is 40 years of age (whichever islonger). Lifelong prophylaxis may be recommended if the patient is at high risk of group A streptococcus exposure. Secondary rheumatic heart disease prophylaxis isrequired even after valve replacement.*Administration every 3 wk is recommended in certain high-risk situations.†Macrolide antibiotics should not be used in persons taking other medications that inhibit cytochrome P450 3A, such as azole antifungal agents, HIV protease inhibitors,and some selective serotonin reuptake inhibitors.Adapted from Gerber et al29
Table 7. Duration of SecondaryProphylaxis for Rheumatic FeverTypeDuration After Last Attack*Rheumatic fever with carditis and residual heart10 y or until patient is 40 y of age (whichever is longer)disease (persistent VHD†)Rheumatic fever with carditis but no residual heart10 y or until patient is 21 y of age (whichever is longer)disease (no valvular disease†)Rheumatic fever without carditis5 y or until patient is 21 y of age (whichever is longer)*Lifelong prophylaxis may be recommended if the patient is at high risk of group A streptococcus exposure. Secondary rheumatic heart diseaseprophylaxis is required even after valve replacement. †Clinical or echocardiographic evidence. Adapted from Gerber et al30
IE ProphylaxisCOR2aLOEC-LDRecommendation1. Antibiotic prophylaxis is reasonable before dental procedures that involvemanipulation of gingival tissue, manipulation of the periapical region of teeth, orperforation of the oral mucosa in patients with VHD who have any of the following:a. Prosthetic cardiac valves, including transcatheter-implanted prostheses andhomografts.b. Prosthetic material used for cardiac valve repair, such as annuloplasty rings,chords, or clips.c. Previous IE.d. Unrepaired cyanotic congenital heart disease or repaired congenital heartdisease, with residual shunts or valvular regurgitation at the site of oradjacent to the site of a prosthetic patch or prosthetic device.e. Cardiac transplant with valve regurgitation attributable to a structurallyabnormal valve.31
IE ProphylaxisCORLOERecommendation2. In patients with VHD who are at high risk of IE,antibiotic prophylaxis is not recommended for nondental3: NoB-NRBenefitprocedures (e.g., TEE, esophagogastroduodenoscopy,colonoscopy, or cystoscopy) in the absence of activeinfection.32
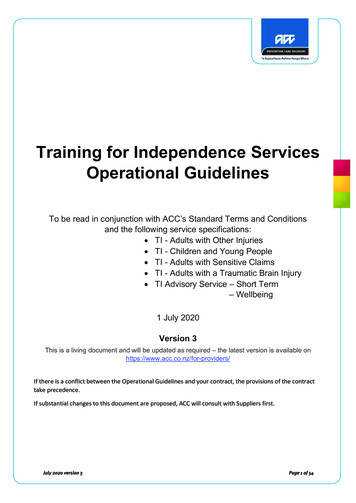
Anticoagulation for AF in Patients With VHDCORLOERecommendations1. For patients with AF and native valve heart disease (except rheumaticmitral stenosis [MS]) or who received a bioprosthetic valve 3 months ago,1Aa non–vitamin K oral anticoagulant (NOAC) is an effective alternative toVKA anticoagulation and should be administered on the basis of thepatient’s CHA2DS2-VASc score.2. For patients with AF and rheumatic MS, long-term VKA oral1C-EOanticoagulation is recommended.33
Anticoagulation for AF in Patients With VHDCORLOERecommendations3. For patients with new-onset AF 3 months after surgical or2aB-NRtranscatheter bioprosthetic valve replacement, anticoagulationwith a VKA is reasonable .4. In patients with mechanical heart valves with or without AF3: HarmB-Rwho require long-term anticoagulation with VKA to preventvalve thrombosis, NOACs are not recommended.34
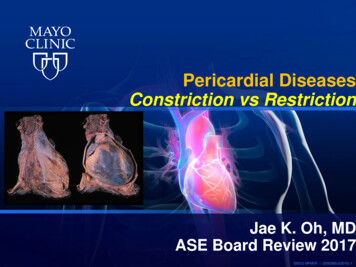
Figure 1.Anticoagulationfor AF in PatientsWith VHD.Colorscorresponds toTable 2.35
Evaluation of Surgical and Interventional RiskCORLOERecommendation1. For patients with VHD for whom intervention is contemplated,individual risks should be calculated for specific surgical and/or1C-EOtranscatheter procedures, using online tools when available, anddiscussed before the procedure as a part of a shared decision-makingprocess.36
Table 8. Risk Assessment for Surgical Valve ProceduresFootnote text located on the next slideCriteriaLow-Risk SAVR (MustLow-Risk Surgical Mitral High Surgical RiskMeet ALL Criteria in This Valve Repair for Primary (Any 1 Criterion in ThisColumn)MR (Must Meet ALLColumn)Criteria in This Column)Prohibitive Surgical Risk(Any 1 Criterion in This Column)STS-predicted risk ofdeath* 3%AND 1%AND 8%ORPredicted risk of death or majormorbidity (all-cause) 50% at 1 yORFrailty†NoneANDNoneAND 2 Indices (moderate tosevere)OR 2 Indices (moderate to severe)ORCardiac or other majororgan system compromisenot to be improvedpostoperatively‡NoneANDNoneAND1 to 2 Organ systemsOR 3 Organ sible procedure-specificimpedimentSevere procedure-specificimpediment37
Table 8. Surgical Risk Assessment*Use of the STS Predicted Risk of Mortality (http://riskcalc.sts.org/stswebriskcalc/#/) to predict risk in a given institution with reasonable reliability is appropriate only ifinstitutional outcomes are within 1 standard deviation of the STS average observed/expected mortality ratio for the procedure in question. The EUROSCORE II riskcalculator may also be considered for use and is available at http://www.euroscore.org/calc.html.†Seven frailty indices: Katz Activities of Daily Living (independence in feeding, bathing, dressing, transferring, toileting, and urinary continence) plus independence inambulation (no walking aid or assistance required, or completion of a 5-m walk in 6 s). Other scoring systems can be applied to calculate no, mild, or moderate to severefrailty.‡Examples of major organ system compromise include cardiac dysfunction (severe LV systolic or diastolic dysfunction or RV dysfunction, fixed pulmonaryhypertension); kidney dysfunction (chronic kidney disease, stage 3 or worse); pulmonary dysfunction (FEV1 50% or DLCO2 50% of predicted); central nervous systemdysfunction (dementia, Alzheimer’s disease, Parkinson’s disease, cerebrovascular accident with persistent physical limitation); gastrointestinal dysfunction (Crohn’sdisease, ulcerative colitis, nutritional impairment, or serum albumin 3.0); cancer (active malignancy); and liver dysfunction (any history of cirrhosis, variceal bleeding,or elevated INR in the absence of VKA therapy).§Examples of procedure-specific impediments include presence of tracheostomy, heavily calcified (porcelain) ascending aorta, chest malformation, arterial coronary graftadherent to posterior chest wall, and radiation damage.38
Table 9. Examples of Procedure-Specific Risk Factors forInterventions Not Incorporated Into Existing Risk ScoresSAVRTAVITechnical or anatomic Prior mediastinal radiation Aorto-iliac occlusive disease precludingtransfemoral approach Ascending aortic Aortic arch atherosclerosis (protuberant lesions)calcification (porcelain aorta may be prohibitive) Severe MR or TR Low-lying coronary arteries Basal septal hypertrophy Valve morphology (e.g.,bicuspid or unicuspid valve) Extensive LV outflow tractcalcificationSurgical MV Repair orReplacementPrior sternotomyTranscatheter Edgeto-Edge Mitral ValveRepair Multivalve disease Prior mediastinalradiationAscending aorticcalcification (porcelainaorta may be prohibitive) Valve morphology(e.g., thickening,perforations, clefts,calcification, andstenosis)Prior mitral valvesurgery39
Table 9. Examples of Procedure-Specific Risk Factors forInterventions Not Incorporated Into Existing Risk ScoresSAVRTAVISurgical MV Repair orReplacementTranscatheterEdge-to-EdgeMitral ValveRepairComorbidities Severe COPD or home Severe COPD orhome oxygenoxygen therapytherapy Pulmonary hypertension Severe RV dysfunction Pulmonaryhypertension Hepatic dysfunction Severe RV Frailty*dysfunction Hepaticdysfunction Frailty* Severe COPD or homeoxygen therapy Pulmonary hypertension Hepatic dysfunction Frailty* Severe COPD orhome oxygentherapy Pulmonaryhypertension Hepaticdysfunction Frailty*40
Table 9. Examples of Procedure-Specific Risk Factors forInterventions Not Incorporated Into Existing Risk ScoresSAVRTAVI STS score 15 Life expectancy 1 y Poor candidate forrehabilitation STS score 15 Lifeexpectancy 1y Poorcandidate forrehabilitationTranscatheter EdgeSurgical MV Repair orto-Edge Mitral ValveReplacementRepairFutility STS score 15 Life expectancy 1y Poor candidate forrehabilitation STS score 15 Life expectancy 1 y Poor candidatefor rehabilitation41
Table 10. Median Operative Mortality Rates forSpecific Surgical Procedures(STS Adult Cardiac Surgery Database, 2019)ProcedureMortality Rate (%)AVR2.2AVR and CABG4AVR and mMitral vValve replacement9Mitral vValve replacement5Mitral vValve replacement and CABG9Mitral vValve repair1Mitral vValve repair and CABG542
The Multidisciplinary Heart Valve Teamand Heart Valve CentersCORLOERecommendations1. Patients with severe VHD should be evaluated by a Multidisciplinary1C-EOHeart Valve Team (MDT) when intervention is considered.2. Consultation with or referral to a Primary or Comprehensive Heart ValveCenter is reasonable when treatment options are being discussed for 1)2aC-LDasymptomatic patients with severe VHD, 2) patients who may benefit fromvalve repair versus valve replacement, or 3) patients with multiplecomorbidities for whom valve intervention is considered.43
PLACEHOLDERTable 11. Structure of Primary andComprehensive Valve Centers44
Periodic Imaging After Valve InterventionCORLOERecommendation1. In asymptomatic patients with any type of valve intervention, abaseline postprocedural TTE followed by periodic monitoring with1C-EOTTE is recommended, depending on type of intervention, length oftime since intervention, ventricular function, and concurrent cardiacconditions.45
Table 12. Timing of Periodic Imaging After ValveInterventionFootnote text located on the next slideValve InterventionMinimal Imaging Frequency†LocationMechanical valve (surgical)BaselinePrimary Valve CenterBioprosthetic valve (surgical)Baseline, 5 and 10 y after surgery,‡ and then annually Primary Valve CenterBioprosthetic valve (transcatheter) Baseline and then annuallyPrimary Valve CenterMitral valve repair (surgical)Baseline, 1 y, and then every 2 to 3 yPrimary Valve CenterMitral valve repair (transcatheter)Baseline and then annuallyComprehensive Valve CenterBicuspid aortic valve diseaseContinued post-AVR monitoring of aortic size ifPrimary Valve Centeraortic diameter is 4.0 cm at time of AVR, as detailedin Section 5.146
Table 12. Timing of Periodic ImagingAfter Valve Intervention*Initial postprocedural TTE is recommended for all patients, ideally 1 to 3 monthsafter the procedure. Annual clinical follow-up is recommended annually for all patientsafter valve intervention at a Primary or Comprehensive Valve Center.†Repeat imaging is appropriate at shorter follow-up intervals for changing signs orsymptoms, during pregnancy, and to monitor residual or concurrent cardiacdysfunction.‡Imaging may be done more frequently in patients with bioprosthetic surgical valves ifthere are risk factors for early valve degeneration (e.g., younger age, renal failure,diabetes).47
Aortic Stenosis48
Table 13. Stages of Valvular Aortic StenosisStageABDefinitionValve Anatomy BAV (or othercongenital valveanomaly) Aortic valve sclerosisProgressive AS Mild to moderateleafletcalcification/fibrosis ofa bicuspid or trileafletvalve with somereduction in systolicmotion or Rheumatic valvechanges withcommissural fusionAt risk of ASValve HemodynamicsAortic Vmax 2 m/swith normal ne Early LVNone Mild AS: aorticdiastolicVmax 2.0–2.9 m/s ormean P 20 mmdysfunctionHgmay be present Moderate AS: aortic Normal LVEFVmax 3.0–3.9 m/s ormean P 20-39 mmHg49
Table 13. Stages of Valvular Aortic StenosisStageDefinitionValve AnatomyC: Asymptomatic Severe ASC1Asymptoma Severe leaflettic severecalcification/ fibrosis orAScongenital stenosis withseverely reduced leafletopeningC2Asymptomatic severeAS with LVsystolicdysfunctionSevere leafletcalcification/fibrosis orcongenital stenosis withseverely reduced leafletopeningValve Hemodynamics Aortic Vmax 4 m/s ormean P 40 mm Hg AVA typically is 1.0 cm2(or AVAi 0.6 cm2/m2) butnot required to definesevere AS Very severe AS is anaortic Vmax 5 m/s ormean P 60 mm Hg Aortic Vmax 4 m/s ormean P 40 mm Hg AVA typically 1.0 cm2(or AVAi 0.6 cm2/m2) butnot required to definesevere ASHemodynamicConsequencesSymptoms LV diastolicdysfunction Mild LVhypertrophy Normal LVEF None Exercisetesting isreasonableto confirmsymptomstatusLVEF 50%None50
Table 13. Stages of Valvular Aortic StenosisStageDefinitionValve AnatomyValve HemodynamicsHemodynamicConsequencesSymptomsD: Symptomatic severe ASD1Symptomatic severehighgradientAS Aortic Vmax 4 m/s or mean LV diastolicSevere leafletdysfunctioncalcification/fibros P 40 mm Hgis or congenital AVA typically 1.0 cm2 (or LV hypertrophystenosis withAVAi 0.6 cm2/m2) but may Pulmonaryhypertensionseverely reducedbe larger with mixed AS/ARmay be presentleaflet opening Exertional dyspnea,decreased exercisetolerance, or HF Exertional angina Exertional syncope orpresyncopeD2Symptomatic severelow-flow,lowgradientAS withreducedLVEF AVA 1.0 cm2 with restingSevere leafletcalcification/fibrosaortic Vmax 4 m/s or meanis with severely P 40 mm Hgreduced leaflet Dobutamine stressmotionechocardiography showsAVA 1.0 cm2 with Vmax 4m/s at any flow rate HF Angina Syncope or presyncope LV diastolicdysfunction LV hypertrophy LVEF 50%51
Table 13. Stages of Valvular Aortic StenosisStageDefinition Valve AnatomyValve HemodynamicsHemodynamicConsequencesSymptomsD: Symptomatic severe ASD3SymptomaticseverelowgradientAS withnormalLVEF orparadoxical lowflowsevere AS AVA 1.0 cm2 (indexedSevere leafletAVA 0.6 cm2/m2) withcalcification/fibrosan aortic Vmax 4 m/s oris with severelymean P 40 mm Hgreduced leafletANDmotionStroke volume index 35mL/m2 Measured when patient isnormotensive (systolicblood pressure 140 mmHg) Increased LV HFrelative wall Anginathickness Syncope or Small LVpresyncopechamber with lowstroke volume Restrictivediastolic filling LVEF 50%52
Initial Diagnosis and Follow-up of ASCORLOERecommendations1. In patients with signs or symptoms of AS or a BAV, TTE is indicated for accuratediagnosis of the cause of AS, assessment of hemodynamic severity, measurement of1ALV size and systolic function, and determination of prognosis and timing of valveintervention.2. In patients with suspected low-flow, low-gradient severe AS with normal LVEF1B-NR(Stage D3), optimization of blood pressure control is recommended beforemeasurement of AS severity by TTE, TEE, cardiac catheterization, or CMR.53
Diagnosis and Follow-up: IinitialDdiagnosis of ASCORLOERecommendations3. In patients with suspected low-flow, low-gradient severe AS with reduced LVEF(Stage D2), low-dose dobutamine stress testing with echocardiographic or invasive2aB-NRhemodynamic measurements is reasonable to further define severity and assesscontractile reserve.4. In patients with suspected low-flow, low-gradient severe AS with normal or reduced2aB-NRLVEF (Stages D2 and D3), calculation of the ratio of the outflow tract to aorticvelocity is reasonable to further define severity.54
Diagnosis and Follow-up:Iinitial Ddiagnosis of ASCOR LOERecommendations5. In patients with suspected low-flow, low-gradient severeAS with normal or reduced LVEF (Stages D2 and D3),2aB-NRmeasurement of aortic valve calcium score by CTimaging is reasonable to further define severity.55
Diagnosis and Follow-up: Eexercise TtestingCORLOERecommendations1. In asymptomatic patients with severe AS (Stage C1), exercise testing is2aB-NRreasonable to assess physiological changes with exercise and to confirm theabsence of symptoms.2. In symptomatic patients with severe AS (Stage D1, aortic velocity 4.0 m/s or3: HarmB-NRmean pressure gradient 40 mm Hg), exercise testing should not beperformed because of the risk of severe hemodynamic compromise.56
Medical Therapy of Patients with ASCORLOERecommendations1. In patients at risk of developing AS (Stage A) and in patients withasymptomatic AS (Stages B and C), hypertension should be treated1B-NRaccording to standard GDMT, started at a low dose, and graduallytitrated upward as needed, with appropriate clinical monitoring.2. In all patients with calcific AS, statin therapy is indicated for primary1Aand secondary prevention of atherosclerosis on the basis of standard riskscore.57
Medical Therapy of Patients with ASCORLOERecommendations3. In patients who have undergone TAVI, renin–angiotensin2bB-Rsystem blocker therapy (ACE inhibitor or ARB) may beconsidered to reduce the long-term risk of all-cause mortality.4. In patients with calcific AS (Stages B and C), statin therapy is3: NoBenefitAnot indicated for prevention of hemodynamic progression ofAS.58
Timing of Intervention of ASCORLOERecommendations1. In adults with severe high-gradient AS (Stage D1) and symptoms of exertional1Adyspnea, HF, angina, syncope, or presyncope by history or on exercise testing, AVR isindicated.2. In asymptomatic patients with severe AS and an LVEF 50% (Stage C2), AVR is1B-NRindicated.3. In asymptomatic patients with severe AS (Stage C1) who are undergoing cardiac1B-NRsurgery for other indications, AVR is indicated.59
Timing of Intervention of ASCORLOERecommendations4. In symptomatic patients with low-flow, low-gradient severe AS1B-NRwith reduced LVEF (Stage D2), AVR is recommended.5. In symptomatic patients with low-flow, low-gradient severe AS1B-NRwith normal LVEF (Stage D3), AVR is recommended if AS isthe most likely cause of symptoms.60
Timing of Intervention of ASCORLOERecommendations6. In apparently asymptomatic patients with severe AS (Stage C1) and lowsurgical risk, AVR is reasonable when an exercise test demonstrates2aB-NRdecreased exercise tolerance (normalized for age and sex) or a fall insystolic blood pressure of 10 mm Hg
severe right ventricular dysfunction or end-organ damage to the liver and kidney. 14. Top 10 Take Home Messages . 10. Bioprosthetic valve dysfunction may occur . ‡ In patients with documented valvular heart disease, the duration of rheumatic fever prophylaxis should be 10 years or until the patient is 40 years of age (whichever is