Transcription
Massachusetts Approach to MedicaidManaged Long-Term Service andSupportsREPRESENTATIVE JEFFREY SÀNCHEZHOUSE CHAIRMAN, JOINT COMMITTEE ON PUBLICH E A LT HNeed for LTSS Reforms in Massachusetts2y Current utilization of LTSSy Projected Growth in Demandy Burden falls largely on stateMedicaid (MassHealth)y MassachusettsMh tt iis hihigh-costht statet t fforLTSS1
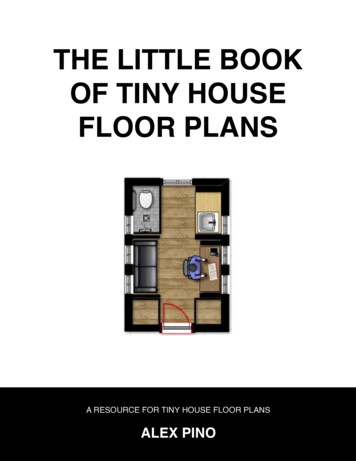
Massachusetts has experience expanding Medicaid managedcare / Mixed Results with MMLTSSMassHealth Coverage3Managed Care Organizations:yBoston Health NetyNetwork HealthyFallon Community Health PlanyNeighborhood Health PlanyHealth New EnglandPrimary Care Clinician Plan:yMassHealth-administered managed care planDual Eligible:yEligible for Medicare coverage due to ageyEligible for Medicare coverage due todisability or other reasonsyMost in FFSySeniors are eligible for SCO & PACEOther FFS:yPatients being assigned to an MCOyBeneficiaries with third party coverageyMembers with access to limited benefitsSource: MassHealth Strategic Planning Document 2012-2015 , April 2013Chapter 305 of the Acts of 2008: Legislative Mandate to ExpandManaged Care Options for Dual Eligibles4“Notwithstanding any general or special law to the contrary, theexecutive office of health and human services shall maximizeenrollmentllt off eligibleli ibl persons iin ththe MMassHealthH lth SSeniori CCare OOptionstiprogram, the Program of All Inclusive Care for the Elderly, theEnhanced Community Options Program and the Community Choicesprogram, or comparable successor programs, and shall develop dualeligible plans. For the purposes of this section, “dual eligible plans”shall be plans that offer similar coverage to Medicaid and Medicareeligible disabled persons under age 65.” – Section 38 of Chapter 3052
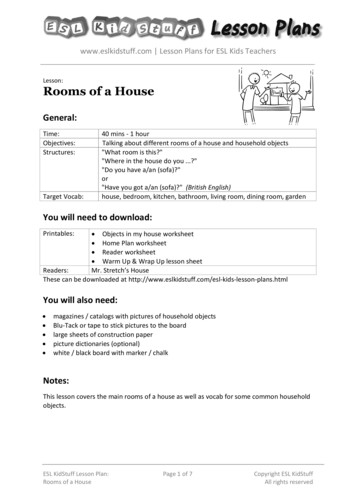
Overview of the Massachusetts Dual Eligible PopulationAged 21-64Key Characteristicsyyyyyyyy5Approximately 115,000 dual eligiblebeneficiaries ages 21 to 64More likelylik l to report poor healthh l h status, anddbe a member of a racial or ethnic minority.65% have behavioral health diagnosis60% have multiple chronic conditions (e.g.COPD, diabetes, cardiovascular disease)14% diagnosed with a developmentaldisability96% live in community settingNearly four-fifths of duals living in thecommunity received a low level of supportservices.3 times more likelyy to have 3 or morelimitations in their activities of daily living,such as dressing, bathing, and eating.Factors Contributing to SubOptimal CareyyyyyyyyAmong the most complex care needs of anypopulationhigh rate of medical service utilization,particularly ER visits and hospitalizationsCare is fragments, not patient-centered.These individuals are presently excludedfrom existing MassHealth managed careoptions and are ineligible for additionalbehavioral health services.Care if based on inefficient FFS providerpayment systemLacks incentives for care management andcoordinationLack access to full range of servicesLimited range of inpatient and outpatientbehavioral health services under Medicaidstate plan and MedicareDuals Identified as a Significant Driver of HealthCare Costs6Source: Dual Eligibles in Massachusetts: A Profile of Health Care Services and Spending for Non-Elderly Adults Enrolled in Both Medicare andMedicaid3
The Massachusetts Approach: OneCarey Massachusetts's approach to the7dual eligible population evolvedinto the state Demonstration planwhich we call OneCarey Informed by simultaneous effortsto adopt broader health carepayment and delivery reforms, inparticular initiative related to:{ Accountable Care Organizations{ Patient-Centered MedicalHomes{ Shift from Fee-for-Service toAltAlternativeti / GlGlobalb lPPaymenttMethodologiesy Supported by key provisions ofAffordable Care Act and 1115Waiver Demonstration renewalOneCare: MassHealth Medicare8Key Objectives of OneCare Ease access to comprehensivecare Deliverer person-centered care Promote independence in thecommunity Improve quality of care andreduce health disparities Eliminate cost-shifting betweenMedicare and MassHealth Operationalize primary-carebehavioral health integration Move patients from FFS toGlobal payments Achieve cost savings for boththe state and federalgovernments throughimprovements in care andcoordinationCovered Services throughOneCare Medicare Parts A, B and D Medicaid State Plan Services Long-Term Services andSupports Diversionary Behavioral HealthServices Community Supports Dental and Vision Additional services to facilitatewellness, self-management andindependent livingEligibility Dually eligible individuals aged21 to64 at time of enrollmentwith the exception of those: Enrolled in PACE, SCO orserviced by HBCS waiver Residing in ICF/MR (facilityfor individuals withintellectual disabilities) Covered under othercomprehensive privateinsurance plan Residing outside of adesignatedgservice area underthe Demonstration4
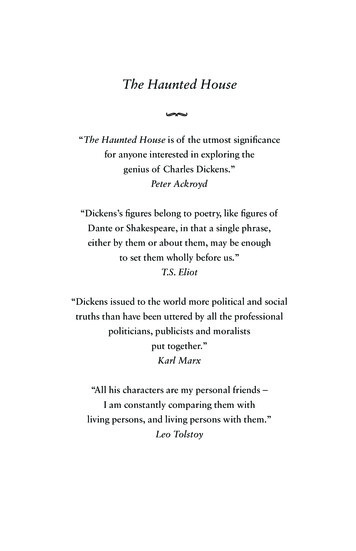
OneCare Plans – Integrated Care Organizations9OneCare Plans - Integrated Care Organizations (ICOs) single accountable entity responsible forthe delivery and management of all medical and behavioral health and LTSS services.y OneCare Plan Contracting and Financing: y{{{yKey OneCare Plan Operation Capacities:{{{{yOne Care plans will receive a combined global payment from the federal and state governments to provide all theservices of Medicare Parts A, B and D, and MassHealthMedicaid payment based on rating category assigned to enrollee according to clinical status, need for LTSS andbehavioral health servicesOneCare plans negotiate separately with providers to determine payment rates for network careInternal capacity or contract out to provide all services in an enrollee’s care plan through a network of providerDemonstrate core competencies across disability populations,Possess prior experience with integration of behavioral health services, serving the homeless and other uniquepopulationsEnsure cultural competency and ADA compliance of the care team and contracted providersOneCare Plans must provide enrollees: {{{{{Integrated Medicare and MassHealth benefitsPPerson-centeredd care withi h integrationii across medical,di l behavioralb h i l healthh l h andd LTSS needsdInterdisciplinary Care Teams, including Care Coordinators and Independent Living and Long Term Services andSupports (IL- LTSS) CoordinatorsIndividualized Care Plans directed by the enrollee and informed by a comprehensive in-person assessment ofmedical, behavioral, and functional needs to be conducted within first 90 daysContinuity of care.OneCare: Care Team and Care Plan10 Unique among the stateproposals, OneCare plans arerequired to contract withIndependent Living-LongTerm Services and Support(LTSS) Coordinators fromcommunity-basedorganizations independent ofthe demonstration health plansPrimary CareProviderClinical CareManager Plans are encouraged to becreative and inclusive incontracting for care teamservices Care teams can pursuecreativei strategiesi to maintaini ienrollee wellness and meetcare goals through appropriateuse of global payment Care must be evidence-basedsupported by accepted practiceguidelines, yet balanced withindividual care needsCareCoordinatorCenteredon thePersonBehavioralHealthProviderPid (as(needed undercare sDesignated byEnrollee5
Issues to Consider in DevelopingYour Own State Plan6y Risk-adjustmenty EnrollmentEllty Rate Developmenty Early and Continual StakeholderEngagementy CoordinatingC di i IntegratedId CareCffor DDualslPopulation with Other Health CareDelivery ReformsCase Study: Bromley-Heath HousingDevelopment76
Case Study: Bromley-Heath HousingDevelopment8Applying the Results: Looking To PediatricAsthma9y Pediatric Asthma Pilot{Based on CommunityA hAsthmaInitiativeI i i i atBoston Children’sHospital{Bundled payment{Access to additionalAddi ilservicesAsthmaAthPilPilot:t PPre- andd PostP tIntervention Results, Phase 17
Learning from the Past: Successful Public HealthEfforts10y Tobacco cessation andpreventionSocietal/Policy FactorsCommunity Factorsy HIV/AIDS preventionInstitutionalTransformationy Like prevention, healthIndividual Factorscare delivery does notexist in a vacuumExtent and Qualityof Health Care andOutcomesSome Final Words11“We are trying to construct a more inclusive society.We are going to make a country in which no one isleft out.”-FranklinFranklin Delano Roosevelt8
Medicare and MassHealth Operationalize primary-care behavioral health integration Move patients from FFS to Global payments Medicare Parts A, B and D Medicaid State Plan Services Long-Term Services and Supports Diversionary Behavioral Health Services Community Supports