Transcription
MASSHEALTH: THE BASICSFACTS AND TRENDSPREPARED BYCENTER FOR HEALTH LAW AND ECONOMICSUNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOLUpdated July 2015JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE
TABLE OF CONTENTS EXECUTIVE SUMMARY2 INTRODUCTION4 ELIGIBILITY AND ENROLLMENT7 SPENDING20 COST DRIVERS28 CONCLUSIONS30JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 1
MASSHEALTH: THE BASICSEXECUTIVE SUMMARYMassHealth is an essential healthsafety net for 1.8 million of thestate’s adults and children The Massachusetts Medicaidprogram (commonly referred to as“MassHealth”) provides healthinsurance to more than one in fourMassachusetts residents. Since thefull implementation of theAffordable Care Act (ACA),enrollment has risen from 1.4million to 1.8 million as of March2015. More than half of peoplewith disabilities, more than half ofchildren of low-income families,and nearly two-thirds of residentsof nursing facilities rely onMassHealth to help them pay forhealth care. Forty percent of allbirths are covered by MassHealth. MassHealth covers services thatcommercial insurance typicallycovers, plus other benefits likelong-term services, additionalbehavioral health care, and nonemergency medical transportation.JULY 2015MassHealth covers a broad cross-section ofthe populationMassHealth supports workers’access to private insurance Children and adults without disabilitiesrepresent three-quarters of totalMassHealth membership, adults andchildren with disabilities comprise aboutone-sixth of MassHealth members, andseniors make up another 9 percent. Morethan 60 cents of every MassHealth dollarspent is for the care of members withdisabilities and for seniors. For more than one-fifth of itsmembers, MassHealth coverage issecondary to other insurance suchas Medicare or employersponsored insurance. MassHealthbenefits help make employeroffered insurance more affordablefor eligible low-wage workers andtheir children by paying for theemployee share of the premiumand by covering most of the costof copayments and deductibles. Inaddition, MassHealth benefitsmake it possible for many peoplewith disabilities to remain in theworkforce. Implementation of ACA coverage provisionshas shifted the makeup of MassHealthmembership more toward people withoutdisabilities, particularly adults. Still, manypeople with disabilities qualify through thestate’s CommonHealth program, whichoffers benefits to persons with disabilitiesthat are not generally available throughemployers or Medicare. TheCommonHealth program can supplementother private insurance or Medicare toprovide benefits that are critical tomaintaining independence, such aspersonal care assistance (PCA) services. The coordination of public andprivate sources of coveragecontribute to Massachusetts’slowest-in-nation percentage ofpopulation who do not havehealth insurance.MASSACHUSETTS MEDICAID POLICY INSTITUTE 2
MASSHEALTH: THE BASICSEXECUTIVE SUMMARY (continued)MassHealth enrollment has continued to grow even as thenumber of uninsured leveled off MassHealth enrollment has steadily grown since 1997, andthe number of Massachusetts residents without insurancesteadily declined from 2004 to 2010. Enrollment continued to grow after the recession endedand to the present day, even though the number ofuninsured has stabilized since 2010. During ACA implementation, approximately 200,000 peoplewere temporarily enrolled in Medicaid while the stateresolved technical problems with the Health Connector’snew, ACA-required eligibility and enrollment system. With the implementation of the ACA, roughly 130,000persons formerly covered under Commonwealth Carethrough the Health Connector were shifted to MassHealth’snew CarePlus program on January 1, 2014.Most members receive their health care in a managed carearrangement Nearly half of members are enrolled in a MassHealthmanaged care organization (MMCO), including nearly350,000 with CarePlus coverage, a new option related tothe ACA expansion.JULY 2015The biggest driver of total MassHealth spending in recentyears has been the jump in MassHealth membership due toeconomic trends and the ACA expansion, not the amountspent for each member Spending on the program has grown, driven by increases inenrollment. Per capita spending for all enrollees combinedhas grown by just 1.3 percent per year since 2007 and hasbeen virtually unchanged since 2010.MassHealth spending trends reflect policy toward providingmore care in community-based settings and less in facilitiesand inpatient settings The share of spending on community-based long-termservices and supports (15%) now exceeds that spent onnursing facilities (13%); both the share and dollar value ofspending on hospital inpatient care declined from statefiscal year 2013 to state fiscal year 2014.MassHealth is an important source of income forphysicians, hospitals and other providers that low-incomeindividuals of all ages depend on for their care Community health centers and nursing homes receive halfof their total patient revenues from MassHealth. Providersof long-term services and supports also rely greatly onMassHealth revenue.MASSACHUSETTS MEDICAID POLICY INSTITUTE 3
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMASSHEALTH OVERVIEW MassHealth is Medicaid (Title XIX of the Social Security Act) and the State Children’s HealthInsurance Program (CHIP, Title XXI). Federally- and state-funded and state-administered A central part of the Massachusetts health care safety net– MassHealth provides health care coverage to one-quarter of the Commonwealth’sresidents, including many of its most vulnerable.– It pays providers for treatments that would otherwise go uncompensated, or not beprovided at all.– It provides a valuable service to employers by covering some of the highest costs of theiremployees and dependents with disabilities.– It brings billions of federal dollars into the state to help finance physical and behavioralhealth care and long-term care for low-income people.– It was the financial engine for the publicly subsidized insurance expansion created by the2006 state health reform law, and continues to supplement federal coverage subsidiesunder the Affordable Care Act (ACA).– It plays an important role in supporting people who are affected by economic downturns.MASSHEALTH PRESENTSCHALLENGES It requires a great amount of public funding to support it. Many of its benefits and eligibility provisions are legal entitlements, which constrains thestate’s options for managing spending during difficult economic times. State systems struggled to adapt to the requirements and expansion authorized by the ACA,resulting in the need to enroll thousands of applicants with “Temporary Medicaid” statusduring state fiscal year 2014, until their eligibility could be positively determined.THE FOLLOWING CHARTS Present an overview of MassHealth eligibility, enrollment and spending. Demonstrate that MassHealth– Provides health insurance that is an essential gateway to health care for more than onequarter of the Massachusetts population;– Is an important source of income for providers who serve low-income patients; and– Has seen modest recent growth in per capita costs while enrollment continues to grow.JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 4
ELIGIBILITY ANDENROLLMENTINTRODUCTIONSPENDINGCOST DRIVERSCONCLUSIONSMASSHEALTH PROVIDES COVERAGE SIMILAR TO COMMERCIALINSURANCE, PLUS SOME ADDITIONAL BENEFITSMassHealth Covers typical commercial benefits, plus:Long-term services and supports (facility and community)*Diversionary behavioral health services (to avert hospitalization)Dental servicesTransportation to medical appointments* Typical Commercial Insurance Coverage Hospital servicesPhysician servicesWell child visitsAncillary services (lab, radiology, etc.)Mental health/substance use treatmentPrescription drugsVision, hearing, medical equipment* Services are available to most but not all MassHealth members.JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 5
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSWaiversWHAT IS AWAIVER?States may request approval from the federal government to waive certain parts of federal Medicaid law, to testprogram innovations or gain more flexibility in how they deliver and pay for Medicaid services. MassHealth has twotypes of waivers, which are authorized under Sections 1115 and 1915c of the Social Security Act.1115DEMONSTRATIONWAIVERThe MassHealth program operates under the authority of an 1115 demonstration waiver for all members under age65, except those who are eligible based on institutional status and a small number of others. The waiver was firstimplemented in 1997, and has evolved through five extensions to expand coverage, support the safety net, provideincentives for delivery system innovations and serve as a platform for health care reform. An important condition ofall 1115 waivers is that they be “budget neutral,” meaning the federal government will contribute no more to awaiver program than it would to a Medicaid program operating under standard rules.1915c HOME &COMMUNITYBASED SERVICES(HCBS) WAIVERSHCBS waivers permit states to provide long-term services and supports in a home or community setting to memberswhose disabilities qualify them for an institutional level of care. Services include home health care, personal care,habilitation, respite, physical and occupational therapy, group adult care, home modification, assistive technologyand others. Many of the services are authorized and overseen by state agencies such as the Executive Office of ElderAffairs, the Department of Developmental Services and the Department of Mental Health, and MassHealth obtainsfederal matching funds on expenditures made. The state must demonstrate that providing the HCBS waiver servicesdoes not cost more on average than providing those services in an institution. In addition, the programs haveenrollment limits. MassHealth has 10 HCBS waivers, which are an important component of the Commonwealth’s“Community First” policy. The waiver programs are targeted to specific populations: Elders age 60 and over with physical disabilities (Frail Elder Waiver) Adults age 22 and over with intellectual disabilities (Community Living, Intensive Supports, Adult Supports Waivers) Adults age 22 and over with acquired brain injuries (ABI Residential, ABI Non-Residential, Traumatic Brain InjuryWaivers) Adults and Elders age 18 and over with physical disabilities who are moving from a facility back to the community(Money Follows the Person Community Living and Residential Supports Waivers) Children age 0 to 8 with autism (Children’s Autism Spectrum Disorder Waiver)JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 6
ELIGIBILITY ANDENROLLMENTINTRODUCTIONSPENDINGCOST DRIVERSCONCLUSIONSMASSHEALTH ELIGIBILITY UNDER ACA400%ELIGIBLE FORTAX CREDITSFOR QUALIFIEDHEALTH PLANCHILDREN300%NOUPPERLIMITNOUPPERLIMITADULTS AGES 21 THROUGH 8AGE IN YEARS19-20DisabledFormerChildren &Foster CareYoung Adults Youth up tothrough Age 20Age 26MassHealth StandardMassHealth CommonHealthConnector Care/Qualified Health Plan (QHP)NOUPPERLIMITFPL*AllOther**MassHealth CarePlusMassHealth Family AssistanceMedicallyFrail Eligiblefor CarePlusbut ElectStandardHIVPositiveDisabled Individuals Parents ofPregnantReceivingChildrenAll AgesServices up to Age 19from DMHIndividualswithBreast orCervicalCancerHCBSWaiverGroup*FPL income as percent of federal poverty level** Includes members previously eligible for Commonwealth Care and for MassHealth Basic and Essential.NOTE: Several MassHealth programs are no longer available effective 1/1/2014 including: MassHealth Basic and Essential, Insurance Partnership, Healthy Start, Prenatal, CommonwealthCare and the Medical Security Program. Populations previously covered by these programs will now be covered by MassHealth Standard, CarePlus and Connector Care.NOTE: In general, the eligibility level for seniors age 65 and older is 100% of FPL and assets of up to 2,000 for an individual or 3,000 for a couple. More generous eligibility rules applyfor seniors residing in nursing facilities or enrolled in special waiver programs.JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 7
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMORE STRINGENT MASSHEALTH ELIGIBILITY FOR SENIORS,THOUGH MOST ALSO HAVE MEDICAREPOPULATIONINCOME /ASSETSCOVERAGELiving in community,with or without Medicare eligibility,citizen or lawfully present immigrant100% FPLAssets at or below 2,000MassHealth Standard or Family Assistance (based onimmigration status); wide range of medical services,plus for Standard, coverage of Medicare cost sharingand premiumsLiving in community, undocumented noncitizen100% FPLAssets at or below 2,000MassHealth Limited – Emergency services onlyLiving in community,eligible for Medicare100% FPLAssets at or below 7,280MassHealth Senior Buy-In, covers non-prescriptiondrugs, Medicare premiums, copays and deductibles.Does not cover other MassHealth Standard services.Living in community,eligible for Medicare 100% – 135% FPLAssets at or below 7,280MassHealth Buy-In covers Part B premiums only.People who are meeting a spend-down deductiblemay qualify for MassHealth Standard.Living in or waiting forfacility-based long-term careNo specific income limitAssets at or below 2,000MassHealth Standard Covering Long-Term Care,patient must pay income minus a monthly personalneeds allowance towards nursing facility care.NOTE: Seniors canqualify for MassHealth through the Frail Elder Waiver with income up to 300% of the SSI benefit rate. Asset limits listed are for individuals;the amounts for couples are higher. See orms/saca-1-english-mb.pdfJULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 8
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMANY DOORS TO MASSHEALTHIndividual applies directly,by phone, on paper form,with assistance at aMassHealth EnrollmentCenter or Health Connectorwalk-in center or throughthe MA Health Connectorwebsite (see below)Health care providersassist patients withapplications HospitalsCommunity health centersNursing homesOther providersState social servicesagencies facilitateapplications Department ofDevelopmental Services Department of MentalHealth Mass. RehabilitationCommission Department ofTransitional Assistance Department of Childrenand Families Other agenciesCommunity organizationsand advocacy groups thatprovide health care referralsor other services assistclients with applications andfollow-up Community actionprograms Community developmentcorporations Aging services accesspoints Health Care For All Other communityorganizations designatedas Enrollment AssistersMAHealthConnector.orgAn integrated eligibility system that allows individuals to shop and apply for health insurance while determining eligibilityfor MassHealth and other health insurance programs. (The Virtual Gateway, formerly the online portal for MassHealthapplications, is still available to apply for other public programs and provides information on MassHealth eligibility)JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 9
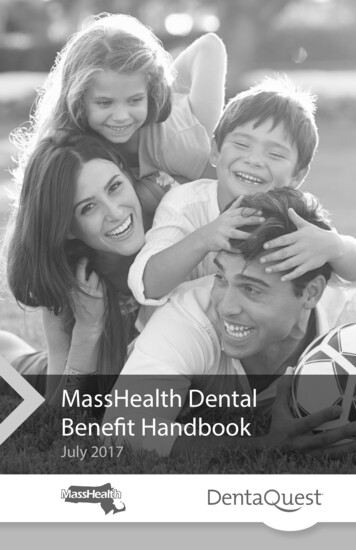
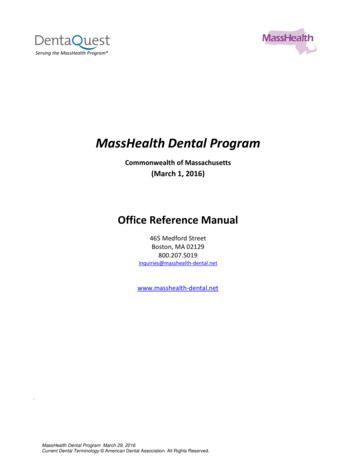
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMASSHEALTH IS IMPORTANT TOMANY POPULATION GROUPSPERCENT OF SELECT MASSACHUSETTS POPULATIONS COVERED BY MASSHEALTH, 2013All non-elderly adults*Non-elderly adults earning 100% FPL and 300% FPL*13.1%34.6%Non-elderly adults earning 100% FPL49.8%All children40.4%Children in families earning 100% FPL and 300% FPL50.3%Children in families earning 100% FPL72.5%Births (child born in last 12 months)Medicare beneficiariesPeople with disabilities (require assistance with self-care)Nursing home residents (2011 data)39.8%31.3%Among the Massachusettspopulation, nearly three-quartersof poor children ( 100 percentFPL) and half of near-poorchildren (100-300 percent FPL),half of poor adults and peoplewith disabilities and nearly twothirds of nursing home residentsare MassHealth members. Nearlya third of people covered byMedicare rely on MassHealth toassist with premiums and costsharing and to cover services,such as long-term services andsupports, that Medicare does notcover.57.7%62.9%* Because of the wording of the survey question from which these data are drawn, these estimates are likely to include some CommonwealthCare enrollees in addition to adults enrolled in MassHealth. The MassHealth population between 100% and 300% of FPL consists mostly of peoplewith disabilities, as well as smaller numbers of members in specific circumstances (pregnant, HIV positive, working for small employers eligible forsubsidies, parents of MassHealth-eligible children up to 133% FPL).SOURCES: Author’s calculationsusing the 2013 American Community Survey (ACS). Nursing home data from Kaiser Family Foundation, “Overview ofNursing Facility Capacity, Financing, and Ownership in the United States in 2011,” June 2013. Data for “all children” and “all non-elderly adults”calculated from 2013 ACS population data and MassHealth Snapshot report, enrollment as of 12-31-13.JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 10
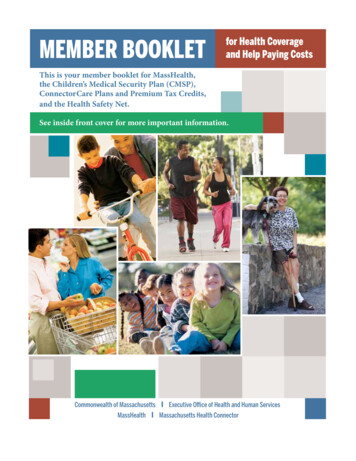
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMASSHEALTH COVERS CHILDREN,ADULTS & SENIORS, AND OFTENSUPPLEMENTS OTHER INSURANCEPERCENT OF TOTAL MASSHEALTH ENROLLMENT (1.8 Million), MARCH 201510,335OTHER 1%SENIORS IN COMMUNITY142,4091% 16,3328%NON-DISABLEDCHILDRENCHILDREN WITHDISABILITIES588,34632%14%SENIORS INNURSING FACILITIES252,420ADULTS WITHDISABILITIES31,510 2%43%793,599SOURCE: MassHealth,JULY 2015March 2015 Snapshot Report.NON-DISABLED ADULTSMassHealth members range fromthe very young to the very old.Members with disabilities,representing 16 percent ofmembership, receive coverage forlong-term care services fromMassHealth that are not usuallyavailable through other healthinsurance sources.Non-disabled adults are a largerportion of MassHealth membersthan in the past because of theACA-related introduction ofMassHealth CarePlus.About one-fifth of MassHealthmembers have coverage throughMedicare or an employer, andMassHealth acts as secondarycoverage. In some circumstances,MassHealth also pays members’premiums and cost sharing for theiremployer-sponsored or Medicarecoverage, if it is more economicalthan paying for full MassHealthbenefits.MASSACHUSETTS MEDICAID POLICY INSTITUTE 11
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSACA IMPLEMENTATION HAS DRIVEN RECENT MASSHEALTHENROLLMENT GROWTH; NON-DISABLED ADULTS UNDER 65 NOWARE NEARLY HALF OF MEMBERSDISTRIBUTION OF MASSHEALTH ENROLLMENT, 2013-2015(NUMBER OF 0,00018%1,000,000800,0008%SENIORS IN COMMUNITY14%ADULTS WITH DISABILITIES2%CHILDREN WITH DISABILITIES44%NON-DISABLED ADULTS1,595,6401,600,0001,400,000SENIORS IN NURSING NE 2013JUNE 2014MARCH 2015NON-DISABLED CHILDREN200,0000From June 2013 to March 2015,MassHealth grew by over 450,000members. Much of that growthoccurred among adults withoutdisabilities, many of whom becameeligible for the first time in January2014, when the ACA’s Medicaidexpansion took effect. This groupgrew by over 360,000 during thisperiod, and now accounts for 44percent of total MassHealthmembership, an increase from 32percent in 2013.It is notable that other populationsgrew as well, even though theireligibility was not impacted by theACA. Between June 2013 andMarch of 2015, the number ofseniors grew by 13,000 or 9percent, while the number ofchildren covered by MassHealthincreased by 66,000 or 12 percent.SOURCE: MassHealth,March 2015 Snapshot Report. Figures exclude applicants assigned “Temporary Medicaid” status. Non-disabled adults includethose who, prior to January 2014, were eligible because they were long-term unemployed.JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 12
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSTHE ACA HAS EXTENDED ELIGIBILITY TO MORENON-DISABLED ADULTS, CHANGING THE MAKEUPOF THE MASSHEALTH-ELIGIBLE POPULATIONMASSACHUSETTS, December 2013MASSACHUSETTS, March 20159%10%38%32%15%20%32%NON-DISABLED CHILDRENSOURCES: MassHealthJULY 2015The Medicaid expansionauthorized by the ACA broughtoverall growth in MassHealthenrollment, heavily influenced bynewly eligible adults, whichaltered the distribution ofMassHealth membership. Thoughtheir share of MassHealthmembers fell, the absolutenumber of non-disabled childrengrew somewhat. The number ofmembers in the other categoriesgrew very slightly, if at all, duringthis period.44%NON-DISABLED ADULTSADULTS & CHILDREN WITH DISABILITIESSENIORSSnapshot Report, March 2015, with data from December 31, 2013 and March 31, 2015.MASSACHUSETTS MEDICAID POLICY INSTITUTE 13
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMASSHEALTH PROVIDES COVERAGE TO MORETHAN ONE IN FOUR MASSACHUSETTS RESIDENTSPERCENTAGE OF POPULATION ENROLLED IN MEDICAID, as of 12/31/201440%STATE HAS IMPLEMENTED ACA MEDICAID EXPANSION (INCLUDES MASS. AS OF 3/31/2015)35%STATE HAS NOT IMPLEMENTED ACA MEDICAID EXPANSION30%25%20%15%This high level of MassHealthparticipation combines withMassachusetts’s higher-thanaverage level of employersponsored coverage to lead to thestate’s lowest-in-nation HDEORMAARWVVTCANYNMDC5%0%States that exercised the ACAoption to expand their Medicaidprograms to cover most residentswith incomes up to 138 percent ofthe federal poverty level tend tocover a larger portion of theirresidents in Medicaid than statesthat did not expand.Massachusetts is among theexpansion states, and MassHealthnow covers more than onequarter of people inMassachusetts.StateCalculations based on Medicaid enrollment data from Centers for Medicare and Medicaid Services, “Medicaid & CHIP: January 2015Monthly Applications, Eligibility Determinations and Enrollment Report” (March 20, 2015); enrollment as of 12/31/2014 and includes CHIP.Massachusetts enrollment is as of March 2015 from MassHealth Snapshot Report. Population estimates for July 1, 2014 from the U.S.Census Bureau.SOURCES:JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 14
ELIGIBILITY ANDENROLLMENTINTRODUCTIONSPENDINGCOST DRIVERSCONCLUSIONSMASSHEALTH ENROLLMENT HAS CONTINUED TO GROW EVEN ASTHE NUMBER OF UNINSURED LEVELED OFFTRENDS IN MASSHEALTH ENROLLMENT AND UNINSURED, 2007–20142,000,000MASSHEALTH 1220132014MassHealth figures monthly averages from the Office of Medicaid. Uninsured numbers for 2007-2011 from the Division of HealthCare Finance and Policy, from a survey in that year, for 2012-2013 from the American Community Survey (ACS) via the Center for HealthInformation and Analysis (CHIA), and for 2014 from a CHIA survey.SOURCES:JULY 2015Since the MassHealth waiverbegan in 1997, MassHealthmembership has steadily grown,and the number of Massachusettsresidents without insurancesteadily declined from 2004-2010.Commonwealth Care, introducedin 2007, also played a role inrecent declines in the number ofuninsured.Since 2010, the number ofuninsured has stabilized or slightlyincreased, while MassHealthenrollment has continued togrow. Much of this growth can beattributed to recent economictrends. Since 2009, thepercentage of Massachusettsresidents living below the povertyline grew from 10.8 to 11.9, andthe percentage of residents withhealth insurance from anemployer declined from 67.1 to62.8 (U.S. Census Bureau).MASSACHUSETTS MEDICAID POLICY INSTITUTE 15
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMEDICAID ENROLLMENT HAS GROWN BOTH NATIONALLY AND INMASSACHUSETTS BECAUSE OF ECONOMIC AND POLICY FACTORSU.S. AND MASSACHUSETTS MEDICAID ENROLLMENT GROWTH180(INDEX YEAR 2007 100)170MASSACHUSETTS160U.S.Medicaid enrollment grewsteadily, both in Massachusettsand across the country, throughthe economic recession and itsaftermath. Enrollment jumpeddramatically in 2014, with theACA-authorized 20132014SOURCES: dicaid-enrollment-in-thousands/#graphfor notes and sources.June data for all years, except 2014 U.S. from July (source: lment-report.pdf). MassHealth Data from Snapshot Reports, June data.JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 16
ELIGIBILITY ANDENROLLMENTINTRODUCTIONSPENDINGCOST DRIVERSCONCLUSIONSNEARLY THREE-QUARTERS OF MASSHEALTHMEMBERS ARE ENROLLED IN MANAGED CAREMASSHEALTH ENROLLMENT BY PAYER TYPE, MARCH 2015MCO551,19130%19%347,246CAREPLUS MCO1% 17,7912% 37,195FFS, PREMIUMASSISTANCEAND LIMITED*501,33827%21%380,189*MassHealth Limited provides coverage for emergency medical services for 103,000 undocumented non-citizens.SOURCE: MassHealth, March 2015 Snapshot Report.JULY 2015PCC PLANONE CARESCOFor persons under age 65,MassHealth offers two options formanaged care: enrolling in one offive private managed careorganizations (MCOs) or in theMassHealth-administered PrimaryCare Clinician (PCC) Plan. Peoplewith disabilities under 65 whoqualify for MassHealth andMedicare may enroll in One Careas a managed care option. Seniorsmay enroll in managed care viaSenior Care Options (SCO). Newenrollees under the ACA, as well asthose who had been in MassHealthBasic and Essential prior to 2014,are enrolled in a new managedcare option called CarePlus.Those in fee for service (FFS)include seniors not enrolled inSCO, people with other coverageas primary (e.g., Medicare oremployer-sponsored insurance)and people who live in aninstitution.MASSACHUSETTS MEDICAID POLICY INSTITUTE 17
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMANAGED CARE: PROGRAM FEATURESMANAGED CARE PROGRAMPOPULATIONS SERVEDCOVERED SERVICESManaged Care Organizations(MCO)MassHealth Standard,Family Assistance andCarePlus members under 65Medical and behavioral health services are covered by acapitated payment to health plans. Long-term services andsupports (LTSS) and dental benefits are not included in MCObenefit but available through MassHealth Fee-For-Service.LTSS benefits are not part of the CarePlus benefit package.Primary Care Clinician Plan(PCC)MassHealth Standard andFamily Assistance membersunder 65Behavioral health services are covered by capitated payment toa behavioral health plan. Medical services, which are notcapitated, are managed by a primary care clinician, and dentaland LTSS benefits are available through MassHealth Fee-forService. Some primary care clinicians receive capitatedpayments as part of the Primary Care Payment ReformInitiative. As of 10/23/15 CarePlus members will be able tochoose PCC Plan.One CareAges 21-64 eligible forMassHealth and MedicareFull spectrum of services are covered by capitated payment toone health plan (includes LTSS, dental and behavioral health).Senior Care Options (SCO)65 eligible for MassHealthand MedicareFull spectrum of services covered by capitated payment to onehealth plan (includes LTSS, dental and behavioral health).JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 18
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSMCOs SERVE A LESS MEDICALLY COMPLEXPOPULATION THAN THE PCC PLANMASSHEALTH MCO AND PCC PLAN ENROLLMENT BY POPULATION TYPE, March 20151,000,000Total: 3%400,000Total: 380,1893%CHILDREN WITH DISABILITIES55%NON-DISABLED CHILDREN14%ADULTS WITH DISABILITIES28%NON-DISABLED ADULTS300,000200,000NON-DISABLED ADULTS —CAREPLUS39%100,0000MCOPCCMassHealth members withdisabilities and other medicallycomplex care needs are morelikely to enroll in the Primary CareClinician (PCC) Plan than with anMCO. MCOs serve a less complexpopulation: with the advent ofCarePlus, more than 60 percent ofMCO enrollees are non-disabledadults and one-third are nondisabled children.In the PCC Plan, about oneenrollee in six is a person with adisability. Many long-termunemployed members whoformerly were enrolled inMassHealth Basic and Essentialare now in the CarePlus managedcare plan. Many of thesemembers are more likely thanother adults to have behavioralhealth needs.TYPE OF MANAGED CARENOTE:Chart shows enrollment for members under age 65.MassHealth, March 2015 Snapshot Report.SOURCE:JULY 2015MASSACHUSETTS MEDICAID POLICY INSTITUTE 19
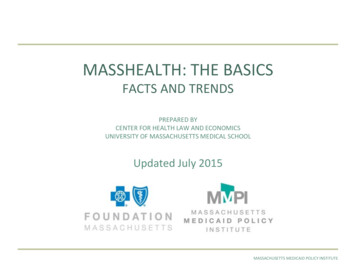
INTRODUCTIONELIGIBILITY ANDENROLLMENTSPENDINGCOST DRIVERSCONCLUSIONSNOMINAL MASSHEALTH SPENDING HAS GROWN BY MORE THANHALF SINCE 2007; WHEN ADJUSTED FOR MEDICAL INFLATIONSPENDING WAS GRADUAL UNTIL 2014MASSHEALTH SPENDING, SFY 2007-2014(BILLIONS OF DOLLARS) 12CURRENT DOLLARS 11 10.9 9.8 10 9.1 9.3 8.8 9 8.9 8.1 7.7 8 7.0 7 7.7 7.4 7.8 7.4 7.9 8.0INFLATION-ADJUSTED DOLLARS 7.0 6 52007200820092010201120122013STATE FISCAL YEAR2014MassHealth spending hasincreased in nominal terms from 7 billion in state fiscal year (SFY)2007 to 10.9 billion in SFY 2014.Adjusting for medical inflation,the average annual increase fromSFY 2007-2013 was approximately2 percent, but jumped to anincrease of over 11 percent fromSFY 2013 to SFY 2014.These are gross spendingamounts, meaning that theyinclude both state and federalrevenues; the federal governmentreimburses Massachusetts forabout half of its MassHealthspending.The spending amounts includepayment for medical benefitsprovided by MassHealth, and donot include the cost of Medicaidreimbursable services from otherstate agencies or supplementalpayments to hospitals.MassHealth Budget Office. Inflation adjustment uses the Medical Consumer Price Index for the Boston area,f
MASSHEALTH: THE BASICS EXECUTIVE SUMMARY MassHealth is an essential health safety net for 1.8 million of the state’s adults and children The Massachusetts Medicaid program (commonly referred to as “MassHealth”) provides health insurance to more than one in four Mass