Transcription
pasdfghjklzxcvNurses Research Publication forContinuing fghjklzxcvbnmEKG Interpretation 2011 Nurses Research Publications PO Box 480, Hayward, CA 94543-0480Office 510-888-90701
HOW TO USE THIS COURSEThank you for choosing Nurses Research Publication home study for your continuingeducation. This course may be completed as rapidly as you desire. However there is a one-yearmaximum time limit.If you have downloaded this course from our website you will need to log back on to payand complete your test. After you submit your test for grading you will be asked to complete acourse evaluation and then your certificate of completion will appear on your screen for you toprint and keep for your records. Satisfactory completion of the examination requires a passingscore of at least 70%. No part of this course may be copied or circulated under copyright law.Instructions:1. Read the course objectives.2. Read and study the course.3. Log back onto our website to pay and take the test. If you have already paid for thecourse you will be asked to login using the username and password you selectedwhen you registered for the course.4. When you are satisfied that the answers are correct click grade test.5. Complete the evaluation.6. Print your certificate of completion.If you have a procedural question or “nursing” question regarding the materials, call(510) 888-9070 for assistance. Only instructors or our director may answer a nursingquestion about the test.Thank you again for choosing our course2
TABLE OF CONTENTSPAGESHow to Take This Course2Objectives4Chapter I: Physiology of the Heart and Circulatory System Campaign5Chapter II: The Electrocardiogram and the Normal EKG17Chapter III49Arrhythmia DeterminationChapter IV Arrhythmias and Select Disease Conditions58Chapter V The 12-Lead EKG65Conclusion78References78Course Exam793
Course ObjectivesAt the end of this course, each student will be able to:1. Perform satisfactorily on an objective examination (70% or better) at the end of thiscourse in relation to all material presented in this course.2. Name and discuss the four most important anatomical structures of the heart that relate tothe EKG.3. Recognize one of the four most dangerous arrhythmias presented in the course, whichcould be dangerous to a person, including the two most frequently used treatmentmethods.4. Interpret correctly the basic arrhythmias presented in this program by using the step-bystep approach outlined in the course.NOTICE: Medicine is an ever-changing science. As new information is gained, changes in thetreatments and drug therapies are required. The author(s), editor, and publisher of this text haveused every possible reliable source in order to verify information in this text, to be sure that theinformation is accurate and the most current and acceptable information available at the time ofpublication. However due to human error and/or changes in medical science, neither the editorsnor publishers nor any other party involved in the preparation of publication of this text, warrantthat the information contained herein is in every respect accurate of complete and they are noresponsible for any errors or omission or for the results obtained from sue of such information.Readers are encouraged to confirm the information contained herein with other sources. Forexample, and in particular, readers should check the product information sheet for any drugsmentioned in this text that you plan to administer.4
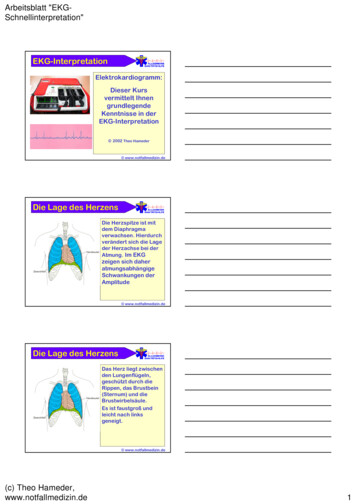
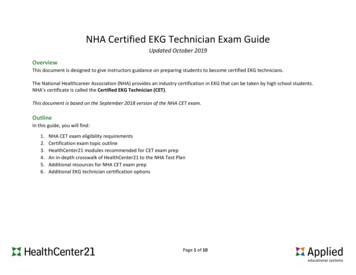
Chapter I: Physiology of the Heart and Circulatory System CampaignAnatomy and Physiology UpdateA. The ThoraxThe first part of this course is a review of the anatomical structures and the physiology of thecardiovascular system in relationship to the nursing care of the patient with a related disorder. Ifyou need to review the structures and/or function that we will be discussing, please refer to anybasic anatomy textbook. However, it is not required that you use any other reference. Allinformation needed to pass the test at then of this course will be including in the text.We will list the most important structures of the thorax and entire CV system only so that youcan relate these to the clinical approach that we will use. Following is an illustration of thethorax and the heart in relationship to other structures noticed upon visual examination. Thethorax has a characteristic shape, size and movement.5
Thorax – Be sure you can identify the following:a. Sternum – mid-chest, flat, non-protrudingb. Ribs – slope of ribs, intercostals spaces, costal marginsc. Heart – heartbeat, in some cases, can be visible as a pulsation in the thorax at lower costalmargind. Shoulder- should be relaxed, and at a 90-degree angle, look for abnormal angles andmusculature that might indicate overuse of accessory musclese. Neck veins – should not normally be visiblef. Clavicle – clavicular line horizontal, no protrusions during breathingg. Respirations – normal respiration should look unlabored and comfortableB. The HeartGross Structures1. Musculature-pericardium, fibrous and serous epicardium, visceral serous pericardium,myocardium, heart muscle.2. Muscle cell (microscopic structures) – central nucleus, sarcoplasm, sarcolemma,sarcomere, intercalated discs.6
Chambers – Right side of the Heart1. Right atrium – the thin-walled atrium, low relative pressure receives blood from superiorand inferior vena cavae, the coronary sinus and thebesian veins, and the outflow of bloodthrough tricuspid valve.2. Right ventricle – relatively thing muscle wall, crescent-shaped, papillary muscles,chordate tendineae, low pressure, outflow though the pulmonic valve to the pulmonaryartery.Left Side of the Heart1. Left atrium – thicker muscle, medium pressure of blood, inflow of blood through fourpulmonary veins. Outflow is the through mitral valve.2. Left ventricle – largest muscle mass, high pressure blood flow, papillary muscles, springlike pump action. Outflow of blood through the aortic valve and the aorta.Cardiac Anatomy:The human heart is a hollow, four-chambered, muscular pump. It is the major organ in themediastinum. The pericardium is the outermost layer of the heart. It consists of parietal andvisceral layers. The pericardial sac, normally containing 5 to 20 cc of fluid, protects themyocardium and prevents friction during the pumping action of the heart.Muscle tissue, the myocardium, makes up the walls of the heart chambers. The left ventricularmyocardium is 5 to 7 times thicker than the right. The inner surface of the myocardium is linedwith endocardium, as are the cardiac valves and blood vessels.The heart is divided into chambers by intraventricular and intra-atrial septa. Fibrous tissuesseparate the atria from the ventricles on the right and left sides of the heart. The tricuspid andmitral valves, tighter called the atrioventricular (A-V) valves, allow for the passage of bloodfrom the atria to the ventricles.Heart ValvesAtrioventricular Valves:1. Tricuspid – has three leaflets, controlled by papillary muscles; chordate tendineae.2. Mitral valve – two cusps, controlled by papillary muscles and the chordate tendineae.Semilunar Valves:1. Pulmonic valve – three leaflet valve, formed by fibrous ring, tendinous tubercle midpointfree edges.2. Aortic valve – three leaflets, also formed by fibrous ring, tendinous tubercle midpointfree edges.7
Vasculature of the Heart1. Right Coronary Artery – most branches of this artery anastomse distally with left anteriordescending.2. Left Coronary Artery – divides into two main branches, left ant. Descending and leftcircumflex artery.3. 3. Great cardiac vein – largest system, forms coronary sinus, drains left ventricleprimarily.4. Anterior cardiac veins – empty directly into right atrium.5. Thebesian Veins – smallest system, empty into right atrium.Conduction System of the Heart1.2.3.4.5.6.7.SA (Sino-atrial node)Atrial preferential pathways; anterior intermodal, middle, posterior intermodal.AV (Atrio-ventricular node)4. Bundle of HISLeft Bundle BranchRight Bundle BranchPurkinje Fibres8
Contractility of Heart MuscleElectrical conduction in the heart is unique and remarkable.Heart muscle possesses the following properties:1.2.3.4.Automaticity – pacemaker abilityConductivity – each cell has ability to conduct impulses to the next cell.Contractility – ability to contract (make each cell shorter or longer)Irritability – each call has ability to contract on its own, to send out impulses to othercells without first being stimulated from another source.9
These properties make the myocardium different from other muscle cells in the body. Thenormal activity of the heart conducts impulses from one point (SA node) to another point(individual muscle cells) thus stimulating a uniform and effective contraction f the heart.Various factors affect the activity of the cardiac muscles. The availability of oxygen, after load,nervous control, muscle condition, and other factors can affect the force of the contraction of theheart. Drugs can also affect the contraction of the heat. Certain drugs depress the heart activelyand others can cause excitation. The nurse should be aware of all the factors that influence heartactivity.Blood Flow Through the Heart (refer back to fig. 1)Blood flow through the heart is shown in the illustration. Blood is shown as it enters the heart,circulates, and then leaves the heart. In relation to the psychical assessment performed by mostnurses, keep in mind the changes in circulation which will be assessed. Impeded flow my causeextra heart sounds and/or physical changes. Also, reduced flow will usually cause changes thatcan be assessed by the nurse.Physical Characteristics Important to Blood Flow:1. Diameter of the blood vessels.2. Cross-section areas of the chambers and vessels.3. Length of the vessels.Qualities of blood:1.2.3.4.5.6.7.8.HeartPulmonary vesselsLarge ArteriesSmall ArteriesArteriolesCapillariesSmall VeinsLarge Veins18%12 8%5%2%5%25%25%Velocities of Blood Flow:The velocity of blood flow is directly related to the amount of circulating blood volume and thearea of the vessels.Blood returns to the heart from the general circulation. Almost 50% of all blood in the body is inthe systemic veins of the body. This system includes small veins and venules and blood in thepulmonary circulation. The small veins usually offer little resistance to blood flow. The largeveins do offer much resistance to the flow of blood to the heart. This is an important nursingimplication, as the patient who is more active will have better flow of blood back to the heart.With reduced activity, the blood tends to pool I the large vessels and can lead to severe venous10
stasis. Blood returns to the heart via the superior and inferior vena cavae, and into the rightatrium.From the right atrium blood flows to the right ventricle and is then propelled into pulmonarycirculation. After blood is aerated with fresh oxygen, it is returned to the left side of the heartinto the left atrium.From the left atrium the blood is ejected into the left ventricle. The left ventricle then pumps theblood out of the heart into the general circulation. The aorta is the first vessel to carry blood,and, at that same time, coronary arteries are fed oxygenated blood to circulate though the heart.The above is only a brief outline of the circulation of blood. Be sure you can trace the bloodthrough the heart. Be sure that you can name all the valves and chambers of the heart as bloodflows through. You should also be able to list the major arteries of the body. When you performthe assessment, it will be necessary for you to know these vessels and their location.Myocardium:Following is a review of the physiology of muscle contraction.Gross Structures:1. Myocardium – heart muscle2. Epicardium- visceral serous pericardium3. Pericardium- parietal and visceral layers4. Muscle cellsa. Central nucleus of cellb. Sarcoplasm – proteinaceous fluidc. Sarcolemma – cell membraned. Sarcomere – contractile until of muscleMuscle contraction is dependent upon the availability of calcium and other electrolytes. Thenervous system sends impulses to the muscle cells. These impulses stimulate release of calcium(Ca ) in the muscle cells. Calcium forms a link between ATP and ADP (energy sources) toinitiate the contraction of the muscle cell. As these energy bonds are formed with in the musclecell, the sarcomere is shortened. Shortening of the sarcomere causes shortening of the musclefiber (cell), and hence the contraction of the entire muscle. When the calcium in the cell is usedup, the sarcomere returns to its normal length and so does the muscle. This is known as diastole.The muscle must replenish its calcium and energy. Cardiac muscle has special properties thatnot all other muscles have. As mentioned earlier in the text, the properties are:1.2.3.4.Contractility: the action of muscle fibers to shorten in length (contraction)Conductivity: each muscle cell can pass electrical impulses from cell to cell.Automaticity: ability to contract without direct stimulation by nervous systemIrritability: ability to respond in a specific way to changing conditions of body tissues.11
Muscle FunctionIn the body many conditions must be met before a muscle will have the ability to contract. Weknow that fluids and electrolytes are important as well as the condition of the body.Listed below are other factors that must be considered:1.2.3.4.5.6.Overall muscle condition.The availability of oxygen to the muscle.Afterload conditions.Nervous control of the muscle.Electrical activation of the muscle.Frank Starling Law: the longer the muscle is stretched during diastole, to a point, thestronger the contraction in the next systole.7. Cardiac output can be increased by the increased availability of sites for electrochemicalbonding when the sarcomere is stretched, up to a point.8. Decreased end-diastolic volume: (hemorrhage, dehydration, etc.) sarcomeres too short toperform properly and cardiac output decreased.9. All or none principle: the nervous innervations must reach a threshold strong enough totrigger the muscle; even with this minimum nerve impulse, the muscle will contract to itsfull potential.The preceding material is review of the anatomy and physiology of muscle contraction. If thisreview “jogs” your memory, then the purpose was accomplished. It is important that you keep inmind the basic principles of muscle physiology. These principles will help you understand someof the following normal and abnormal ECG tracings.Anatomy Related to the ECGRepresented next is the electrical pathway of the impulses through the heart. Each wave on theECG is related to a portion of those impulses. When the heart muscle is stimulated by theelectoral impulses, blood is ejected from eh corresponding chamber of the heart.a. Basic Facts:1. Fluid bathes the inside and outside of the cell membrane.2. The fluid is an electrolyte solution carrying ( ) and (-) ions.3. Current will flow between ions of opposite polarity.4. When cells are at rest, the extracellular fluid is mostly positive, therefore, there willbe no current flow.5. When the cell membrane is stimulated, current will flow.6. K goes in and out freely at all times.7. CL- is equal on both sides of the cell.8. K is limited outside the cell.9. Process is diffusion gradient change and the negative chargers inside the cell attractNA ion to enter cell’s interior.12
b. Cellular Physiology Terminology1. Vector - Symbolic representation of physical force.2. Electric Tension - Latent energy resulting from the collection of ( ) and (-) ions.3. Resting Membrane Potential – (polarized state) in a polarized cell there are anequal number of ( ) and (-) chargers. Normal resting membrane potential is 85mv to -95mv.4. Depolarization - is when the polarized state has been interrupted by a stimulus,the result is that Na ions rush inside the cell and some K leaves the cell, and thecell’s polarity changes.5. Repolarization - is the state where the cell returns to its polarized state and thepolarity reverses.6. Action potential - the rapid sequence of depolarization and repolarization.7. Selective Permeability - with all living cells, the membrane passes somesubstance but blocks others.8. Sodium pump - a metabolic pump that pumps Na out of a cell, and pumps K to cell’s interior, this occurs only in diastole.C. Cellular Activity1. Resting Cella. Has equal number of ( ) and (-) charges.b. Repolarized.Example: - --- - K 2. Depolarized Cella. Exchange of Na and K and polarity reversesNa (-)K 13
3. Repolarized Cella. Reversal of polarity and exchange of Na and K K ( )Na D. Uniqueness of Pacemaker Cell vs. Non-Pacemaker Cell1. SA NodePacemaker cells have one phase of action potential. The reason is because of a time –dependent decay in K conductance. This, plus passive diffusion of Na back into the cell,causes a threshold to be reached. (Constant Na leakage, and constant K moving) Allaction is self-initiated.2. Phases of Action Potential:Phase 0This is the portion from the threshold to peak action potential (i.e. the exchange of Na andK in the cells).Phase 1Initiate stage of repolarization, it has a brief origin (initial phase due to influx of C1- ion).Phase 2During the next 0.1 second, the repolarization process slows. This period does not exist inskeletal muscle. This allows cardiac muscle to have a more sustained contraction (isometriccontraction; plateau phase).Phase 3Sudden acceleration of the rate of repolarization as K leaves the cell in response to theinflux of Na .Phase 4This represents the resting potential.14
E. Membrane Responsiveness1. DefinitionThe relationship of resting membrane potential at excitation to the rate of depolarizationduring phase 0 of the action potential; normal resting membrane potential is 85 to 90 mv.Maintenance of Membrane PotentialIs dependent upon the integrity of the cell membrane; injury, ischemia, chemical intoxicationand also radical temperature changes can alter membrane potential.F. Refractory Periods1. Relative Refractory PeriodSome cells are polarized and others are not. A strong stimulus can produce a response in thepolarized cells (after P wave complex by T wave).2. Absolute Refractory PeriodWhen cells are refractory and unable to accept any stimulus.G. VectorsA vector is a symbolic representation of a physical force. It has direction and magnitude,characterized by an arrow, (Plus or Minus). Vector size varies; it depends upon muscle mass.H. AxisAn axis is a center point or center line (symbolic). Normal flow of current is in the heart isprimarily from the base to the apex. This preponderant flow of current is known as the axis.Axis is the sum total of all the small vectors.I. Conduction System Components15
Electrical Conduction System of the Heart:The electrical conduction system of the heart is composed of sinoatrial (SA) node, internodalatrial conduction tracts, interatrial conduction tract, atrioventicular (AV) node, bundle of HIS,right and left bundle branches, and Purkinje network. The AV node and the bundle of HIS formthe AV junction. The bundle of HIS, the right and left bundle branches, and the Purkinjenetwork are also known as the HIS-Purkinje system of the ventricles. As its sole function, theelectrical conduction system of the heart transmits minute electrical impulses from the SA node(where they are normally generated) to the atria and ventricles, causing them to contract.The SA node lies in the wall of the right atrium near the inlet of the superior vena cava andconsists of pacemaker cells that generate electrical impulses automatically and regularly. TheAV node lies partly in the right side of the interatrial septum in front of the opening of thecoronary sinus tricuspid valve.Electrical Basis of the EKG (Based on the pathway depicted in the figure above.)The electrocardiogram, ECG, is a graphic record of the direction and magnitude of the electricalactivity that is generated by the depolarization and repolarization of the atria and ventricles. Thiselectrical activity is readily detected by the electrodes attached to the skin. In the next section wewill go into more detail about the EKG tracing and the normal EKG. This will lay a foundationfor interpretation of arrhythmias to come later.We use EKG – ECG interchangeably. They mean the same thing. EKG was a term originatedfrom old English, and is still used today. Some facilities prefer one term over the other. Use theterm that is preferred at your facility.16
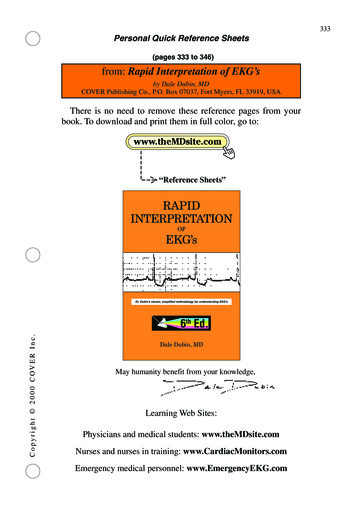
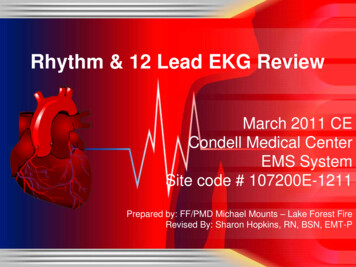
Chapter II: The Electrocardiogram and the Normal EKGPart I: The ECG Paper and the Normal ECG TracingIn order to begin to understand the interpretation of EKC’s one must have an understanding ofthe EKG paper. Shown in the illustration below are a sample of EKG paper and an enlargementof the markings. The time intervals are shown as well as the measurements of each block on thepaper. You will be able to make fairly accurate measurements of the patient’s heart rate andother measurements by counting blocks up and down on the paper.The EKG paper records time sequences (horizontal deflections) and amplitude (verticaldeflections) of the electrical activity of the heart. The horizontal lines measure time intervals andheart rate. Each of the small squares equal 0.4 second of time. Five small squares equal 0.20seconds. Fifteen of the 0.20 squares represent 3 seconds. These 3 – second time intervals aremarked on the paper by darker lines as shown below.Conversion table for heart RateListed here is a quick guide for determination of heart rate:Number of Small Spaces:Rate Per 818872146250530017
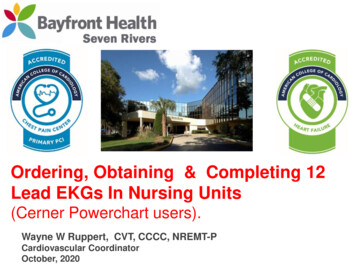
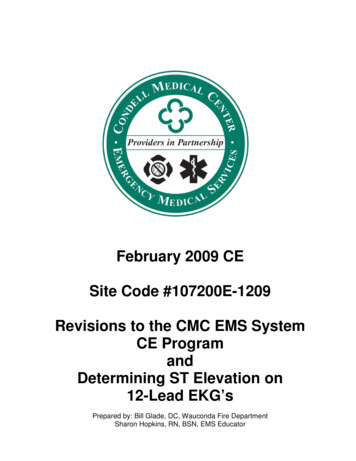
Components of Normal Sinus RhythmP Wave:The P wave represents depolarization of the right and left atria.Onset of the P Wave is identified as: the first abrupt or gradual deviation from the baseline. Thepoint where the wave returns to the baseline marks the end of the P Wave. A QRS complexnormally follows each P Wave. A normal sinus P Wave indicates that the electrical impulseresponsible for the P Wave originated in the SA node and that normal depolarization of the rightand left atria has occurred.1. SA node is the pacemaker site.2. The first part of the normal sinus P Wave represents depolarization of the right atrium;the second part represents depolarization of the left atrium.3. During the P Wave, the electrical impulses progress from the SA node through theintermodal atrial conduction tracts and most of the AV node.4. The DIRECTION of the P Wave in lead II is positive (upright).5. The DURATION is 0.10 seconds or less.6. The AMPLITUDE is 0.5 to 2.5 mm high, in lead II (rarely over 2mm high)7. The SHAPE is normally smooth and rounded.8. The P-R INTERVAL is normally 0.12 to 0.20 seconds; abnormal is greater than 0.20seconds.18
QRS ComplexA QRS Complex represents depolarization of the right and left ventricles.The pacemaker site of a normal QRS complex is the SA node or an ectopic pacemaker in theatria of AV junction. (The origin of the QRS is originally from the SA node, and then spreadsdown through the atria to the AV node, etc.) The onset of the QRS Complex is identified as thepoint where the first wave of the complex just begin to deviate, abruptly or gradually, from thebaseline.This end of the QRS Complex is the pone there the last wave of the complex begin to flatten out,sharply or gradually, at, above, or below the baseline. This point the junction between the QRScomplex and the S-T segment is called the “JUNCTION” or “J POINT.” A normal QRSComplex indicates that the electrical impulse has progressed normally from the bundle of HIS tothe Purkinje network through the right and left bundle branches, and that normal depolarizationof the right and left ventricles has occurred. Of course, there can be several “normal” variationsof the QRS Complex. These will be discussed later in the course.1. The Q Wave is the first negative deflection in the QRS Complex not preceded by an RWave.2. The R Wave is the first positive defection in the QRS Complex.3. The S Wave is the first negative deflection that extends below the baseline in the QRSComplex that follows the R Wave.4. The DURATION of the QRS Complex is 0.06 to 0.10 seconds in adults and 0.08 or lessin children.19
T WaveA T Wave represents ventricular repolarization.Repolarization of the ventricles begins at the epicardial surface of the ventricles and progressesinwardly through the ventricular walls to the endocardial surface. The T Wave occurs during thelast part of the ventricular systole. The onset of the T Wave is the first or abrupt or gradualdeviation from the S-T segment; or from the point where the slope of the S-T segment appears tobecome abruptly of gradually steeper. If the S-T segment is absent, the T Wave begins at the endof the QRS Complete (or the J Point). The point where the T Wave returns to the baseline marksthe end of the T Wave. Often the onset and end of the T Wave are difficult to determine withcertainty.1.2.3.4.The DURATION of the T Wave is 0.10 to 0.25 seconds or greater.The AMPLITUDE of the T Wave is less than 5 mm.The SHAPE of the T Wave is sharply or bluntly rounded and slightly asymmetrical.A T Wave always follows a QRS Complex.The U WaveThe U Wave probably represents the final state of repolarization of the ventricles.The U Wave probably represents repolarization of a small segment of the ventricles, such as thepapillary muscles or ventricular septum, after most of the right and left ventricles have beenrepolarized. Although uncommon, and not easily identified, the U Wave can best be seen when20
the heart rate is slow. A U Wave indicates that the repolarization of the ventricles has occurred.An abnormally tall U wave may be present in hypokalemia, cardiomyopathy, left ventriclehypertrophy, diabetes, and may follow administration of digitalis and quinidine.1. The ONSET of the U wave is identified as the first abrupt or gradual deviation from thebaseline or the downward slope of the T Wave.2. The END of the U Wave is the point where it returns to the baseline or downward slopeof the P Wave.3. The DIRECTION of the U Wave is positive (upright), the same as that of the precedingnormal T Wave in lead II. An abnormal U Wave may be flat or inverted.4. The DURATION of the U Wave is normally not determined and the duration is normallynot significant, except in rare cases.5. The AMPLITUDE of a normal U Wave is usually less than 2mm and always smaller thanthat of the preceding T Wave in lead II.6. The U Wave always FOLLOWS the peak of the T Wave and occurs before the next PWave.The EKG LeadsThe 12-lead EKG will be discussed in greater detail later in this course. However, at this timewe will present an introduction to the EKG leads simply to help explain the basics of EKGinterpretation that will follow. Later, the specifics of leads and lead placement will be discussed.An EKG lead consists of two surface electrodes of opposite polarity (posi
7 Chambers – Right side of the Heart 1. Right atrium – the thin-walled atrium, low relative pressure receives blood from superior and inferior vena cavae, the cor