Transcription
The KneeOrthopedics and NeurologyJames J. Lehman, DC, MBA, FACOUniversity of Bridgeport College ofChiropractic
The KneeInternal derangement of the knee (IDK) This a common provisional diagnosis forany patient with mechanical symptoms ofthe knee. (Evans) IDK might also stand for “I don’t know” An appropriate diagnose enhances thepatient’s opportunity to heal with lessdisability and improved function
The Knee Consists of two joints1. Patellofemoral2. Tibiofemoral
The KneeAnatomy of the anteromedial aspect
The Knee 1.2.3.4.Knee pain may rise from:JointPeriarticular tissuesHipFemur
The KneeAnatomy of the anterolateral aspect
The Knee Pain is the most common presentingsymptom of knee pathology and the causestend to be related to age, according toEvans.
The KneeKnee stability depends on the following fourligaments1.2.3.4.Tibial collateralFibular collateralAnterior cruciatesPosterior cruciates
The Knee Lacks stability Not a hinge joint Minor derangements in knee cause“traumatic arthritis” better known asdegenerative joint disease or DJD Menisci provide very little stability
The KneeStability is provided by soft tissues Ligaments Capsule Muscles
The KneeParts of knee that might be injured LigamentsMuscle tendonsCapsuleMeniscusCartilageBoneBursaeAny combination of these
The KneeArticulations FemurPatellaTibiaNot the fibula
The KneeMotions Flexion (130-150 degrees) Extension (0 degrees) Rotation (Internal/External) with flexion butnot extension (10 degrees)
The KneeThigh muscles that attach to medial side of tibia nearthe pes anseurine Gracilis (obturator n) Sartorius (femoral n) Semitendinosus (tibial n)
The KneeThigh muscles that attach to medial side of tibia nearthe pes anseurine
The KneeThigh muscles that attach to medial side of tibia nearthe pes anseurine
The KneePalpation of tibial tubercle and pes anseurineinsertion and bursa
The KneeClinically significant bursae
The KneeSciatic nerve innervates Hip jointBiceps femorisSemitendinosusSemimembranosusIschial head of the adductor magnus
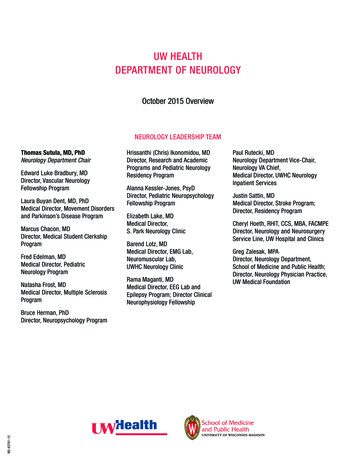
Normal Knee JointFemoral nerve neuropathy Quadriceps weakness and atrophy Loss of patellar reflex Sensory changes over anterior thigh andmedial aspect of lower leg Neurological examination should includemensuration of quadriceps (4 inches or10cmsuperior to the knee Evans and 3 inchesHoppenfeld)
The KneeMensuration of quadriceps for atrophy
Knee Joint Disease May present weakness and atrophy of thequadriceps
The KneeClinically significant bursae PrepatellarSuperficial infrapatellarDeep infrapatellarPes anserine or anseurinehttp://orthoinfo.aaos.org/fact/thr report.cfm?thread id 205&topcategory Knee
The KneeOsgood-Schlatter’s Syndrome Knee pain with young athletes Tenderness at insertion of infrapatellartendon into the tibial tubercle Avulsion of tibial tubercle Infrapatellar tendon loses rigidity and apalpable defect is palpable
The KneeOsgood-Schlatter’s Syndrome
The KneeAbduction Stress TestAlso known as Valgus Stress Test Assessment for medial collateral ligamentinjury Medial meniscus may also be injured withMCL injury Valgus stress to the extended knee Positive test with pain above, below, or atmedial joint line
The KneeAbduction Stress Test
The KneeAdduction Stress TestAlso known as the Varus Stress Test Assessment for lateral collateral ligamentMechanism of injury varus force withflexed kneeUsually ruptures at fibular insertion or itmay avulse at fibular styloidPossible peroneal palsy
The KneeAdduction Stress Test Usually torn in conjunction withposterolateral ligament complex1.Lateral capsule2.Arcuate ligament3.Popliteus tendon
The KneeAdduction Stress Test
The KneeApley’s Compression TestAlso known as Apley’s Distraction Test and Apley’sGrinding Test Assessment for collateral ligament injuryand meniscus tears Medial meniscus is injured more often thanthe lateral Apley’s and McMurray tests are mostcommonly used to diagnose meniscal tears
The KneeApley’s Compression Test
The KneeApley’s Distraction Test
The KneeChildress Duck Waddle Test Assessment for medial and lateral meniscustears Most common type of meniscal tear is the“bucket-handle” along the longitudinal axis The second most common is a tear along itstransverse axis.
The KneePalpation of the medial meniscus anterior portionand the coronary ligaments
The KneeInternal rotation enhances palpation of medialmeniscus
The KneePalpation of the lateral meniscus and its coronaryligaments
The KneeChildress Duck Waddle Test Test with patient standing with feet apart. Internally & externally rotate and squat. Positive test pain, inability to fully flexthe knee, or a clicking sound on eitherposterior side of the joint Internal test medial meniscus tear External test lateral meniscus tear
The KneeDrawer Test 1.2.3.4.5.6.7.Assessment for injury to some degree of:Anterior cruciate ligamentPosterolateral capsulePosteromedial capsuleMedial collateral ligamentIliotibial bandArcuate-Popliteus complexPosterior cruciate ligament
The KneePosition for eliciting the anterior drawer sign
The KneeA positive anterior drawer test tear of anteriorcruciate ligament
The KneeA positive posterior drawer test tear of posteriorcruciate ligament
The KneeLateral Pivot Shift ManeuverAlso known as Test of McIntosh 1.2.3.4.5.Assessment for injury to some degree of:Anterior Cruciate LigamentPosterior capsuleArcuate-popliteus complexLateral collateral ligamentIliotibial band
The KneeLateral Pivot Shift ManeuverAlso known as Test of McIntosh Test includes:1. The pivot shift test begins with knee inextension2. The jerk test begins with knee in flexion3. The Losee test begins with the knee inflexion(See page 789)
The KneeMcMurray Sign Assessment for medial or lateral meniscusinjury Injuries to menisci are most common withmales younger than 45 Caused by a twisting force with knee flexedor semi-flexed
The KneeMcMurray Sign Sign is present if at some point in the arc, apainful click or snap is heard The arc includes both external and internalrotation with flexion and then extension ofthe hip and knee Internal rotation lateral meniscus External rotation medial meniscus
The KneeMcMurray Test
The KneeMcMurray Test
The KneeMcMurray Test
The KneeMcMurray Test
The KneeNoble Compression Test Assessment for iliotibial band frictionsyndrome Test with patient supine Flex hip and knee to 90 degrees Thumb pressure to lateral femoral condyle If extension of knee with pressure overcondyle produces pain near 30 degrees it isa positive test
The KneeClarke’s Sign Assessment for chondromalacia patellae1. Post traumatic fracture2. Tracking disorders with patellofemoralarthralgia3. Primary malacia is usually bilateral withunknown etiology
The KneeClarke’s Sign Knee fully extended Compress quadriceps at superior pole ofpatella Patient gently contracts quadriceps Sign is present when patient experiencespain and is unable to continue Severity may be differentiated by amount ofpain and presence or absence of crepitation
The KneeFouchet’s Sign Assessment for patellar tracking disorder,peripatellar syndrome, or patellofemoraldysfunction. Procedure involves compression of patella againstfemur Sign is present with point tenderness and pain atthe patellar margin Transverse rub audible or palpable grating andpain confirm presence of sign
The KneePatellar femoral grinding test
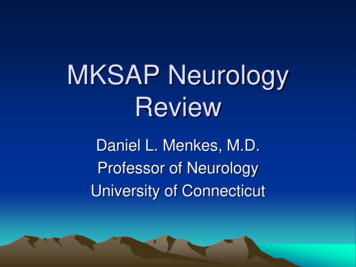
The FootHelbing’s Sign Assessment for Pes Planus or flat foot Sign is present when there is medial curvingof Achilles tendon, as viewed from theposterior aspect. Helbing’s sign indicates foot pronation
Pes PlanusTalar head displaces medially and plantarward
Pes Planus1.Medial prominence of head of talus2. Callosity of over head of talus
Helbing’s Sign PresentOs Calcis in valgus and in pes planus
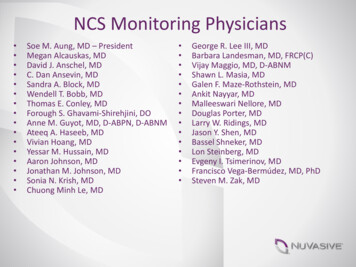
The FootStrunsky’s Sign Assessment for metatarsalgia Sign is present when passive flexion of toesproduces pain with patient supine and lowerextremity extended. Pain is located in the anterior arch of thefoot.
Palpation of the Metatarsals
Palpation of Metatarsals
Transverse Arch of FootLocated immediately behind the metatarsal heads
1. Metatarsal Head Callosities2. Dropped second metatarsal head with associatedplantar callus formation
Claw ToesFrequently accompany metatarsalgia
Orthopedics and Neurology James J. Lehman, DC, MBA, FACO University of Bridgeport College of Chiropractic. The Knee . Hoppenfeld) The Knee Mensuration of quadriceps for atrophy. Knee Joint Disease May present weakness and atrophy