Transcription
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.SECTION THREE: THE PATIENT’S ELECTRONIC RECORDOR PAPER CHARTCHAPTER 8The Patient’s ElectronicMedical Record or Chartc0008OUTLINEChapter ObjectivesVocabularyAbbreviationsPurposes and Use of a Patient’s Electronic MedicalRecord or Paper ChartThe Patient Electronic Medical Record or Paper Chart asa Legal DocumentMilitary TimeConfidentialityThe Electronic Medical RecordGuidelines to Follow When Entering Information intothe Patient’s Electronic Medical RecordThe Paper ChartGuidelines to Follow When Writing in a Patient’s PaperChartThe Chart BinderThe Chart Rack for Paper ChartsPatient Identification LabelsStandard Patient Chart FormsPreparing the Patient’s Paper ChartStandard Patient Chart Forms Initiated in the AdmittingDepartmentStandard Patient Chart Forms Included in the AdmissionPacketStandard Patient Chart Form Initiated by the PhysicianSupplemental Patient Chart FormsClinical Pathway Record FormAnticoagulant Therapy RecordCHAPTER OBJECTIVESp0010 On completion of this chapter, you will be able to:o0010o0015o00201. Define the terms in the vocabulary list.2. Write the meaning of the abbreviations in the abbreviations list.3. List six purposes for maintaining an electronicmedical record (EMR) or paper chart for eachpatient.Diabetic RecordConsultation FormOperating Room RecordsTherapy RecordsParenteral Fluid or Infusion RecordGraphic Record FormFrequent Vital Signs RecordConsent FormsSurgery or Procedure Consent FormProcedure for Preparing Consent FormsMethods of Error Correction on Paper Chart FormsMonitoring and Maintaining the Patient’s ElectronicMedical RecordHealth Unit Coordinator Duties for Monitoring andMaintaining the Patient’s Electronic Medical RecordMaintaining the Patient’s Paper ChartHealth Unit Coordinator Duties for EffectiveMaintenance of the Patient’s Paper ChartSplitting or Thinning the ChartReproduction of Chart Forms that Contain PatientInformationKey ConceptsReview QuestionsSurfing for Answers4. Demonstrate knowledge of military time by convert- o0025ing military time to standard time and standard timeto military time.5. List five guidelines to be followed by all personnel o0030when entering information into a patient’s EMR.6. Describe how the patient’s medical records are orga- o0035nized and identified when paper charts are used, andlist five guidelines to be followed by all personnelwhen writing on a patient’s paper chart.11810008-GILLINGHAM-9781455707201
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.CHAPTER 57. Identify four standard patient chart forms that areinitiated in the admitting department.8. State the purpose of seven standard chart formsincluded in a patient’s electronic or paper admissionpacket, and list information that is included on thehistory and physical form.9. Define what is meant by a supplemental chart form,and provide at least two examples of supplementalchart forms.10. Explain the importance of accurately charting vitalsigns in a timely manner, and explain the correctionof three types of errors on a graphic record.11. Describe the purpose of a consent form, and list fiveguidelines to follow in the preparation of a consentform.12. List four types of permits or release forms thatpatients may be required to sign during a hospitalstay.13. Describe the methods for correcting a labeling errorand a written entry error on a patient’s paper chartform.14. List seven health unit coordinator (HUC) duties inmonitoring and maintaining the patient’s EMR.15. List eight HUC duties in maintaining a patient’spaper chart.16. Explain the purpose and process of splitting or thinning a patient’s chart, stuffing charts, and reproducing chart forms.VOCABULARYp0095 Admission Packet A preassembled packet of 140chart forms to be used on admission of a patient to thenursing unit.Allergy An acquired, abnormal immune response to asubstance that does not normally cause a reaction; suchsubstances may include medications, food, tape, andmany other items.Allergy Bracelet A plastic bracelet (usually red) that is wornby a patient that indicates allergies he or she may have.Allergy Label A label affixed to the front cover of a patient’s paper chart that indicates the patient’s allergy.Identification Labels Labels that contain individual patient information for identifying patient records or other personal items.Name Alert A method of alerting staff when two or morepatients with the same or similarly spelled last namesare located on a nursing unit.Old Record A patient’s paper record from previous admissions, stored in the health information managementdepartment, that may be retrieved for review when a patient is admitted to the emergency room, nursing unit,or outpatient department; older microfilmed recordsalso may be requested by the patient’s doctor.Split or Thin Chart Portions of the patient’s current paperchart are removed when the chart becomes so full that itis unmanageable.Standard Chart Forms Forms included in all inpatient paper charts that are used to regularly enter informationabout patients.Stuffing Charts Placing extra chart forms in patients’ papercharts so they will be available when needed.The Patient’s Electronic Medical Record or Chart119Supplemental Chart Forms Patient chart forms used only p0145when specific conditions or events dictate their use.WALLaroo A locked workstation that is located on the wall p0150outside a patient’s room; it stores the patient’s paperchart or a laptop computer, and when unlocked it formsa shelf to write on.ABBREVIATIONSt0015Note: These abbreviations are listed as they are commonly p0155written; however, they also may be seen in uppercase or lowercase letters and with or without periods.AbbreviationMeaningH&Phistory and physicalHxhistoryID labelsidentification labelsMARmedication administration recordNKAno known allergiesNKFAno known food allergiesNKMAno known medication allergiesNKDAno known drug allergiesEXERCISE 1b0010Write the abbreviation for each term listed.1.2.3.4.5.6.7.8.historyno known allergiesidentification labelshistory and physicalmedication administration recordno known medication allergiesno known drug allergiesno known food allergiesEXERCISE 2Write the meaning of each abbreviation listed.1.2.3.4.p0160ID POSES AND USE OF A PATIENT’SELECTRONIC MEDICAL RECORD ORPAPER CHARTs0010The patient’s electronic medical record (EMR) or paper chart p0260serves many purposes, but for a health unit coordinator (HUC),the electronic record or chart is seen mainly as a means of communication between the doctor and the hospital staff.The EMR or chart is also used for planning patient care, for p0265research, and for educational purposes. As a legal electronicrecord or documentation, the medical record protects thepatient, the doctor, the staff, and the hospital or health carefacility. Careful entries and notations by doctors and other personnel provide an electronic or written record of the patient’sillness, care, treatment, and outcomes of hospitalization. Ifthe patient is readmitted to the hospital or health care facility,the paper chart may be retrieved from the health information10008-GILLINGHAM-9781455707201
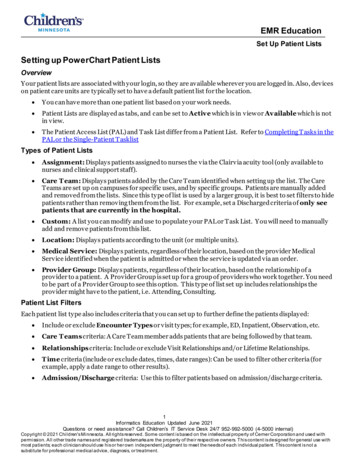
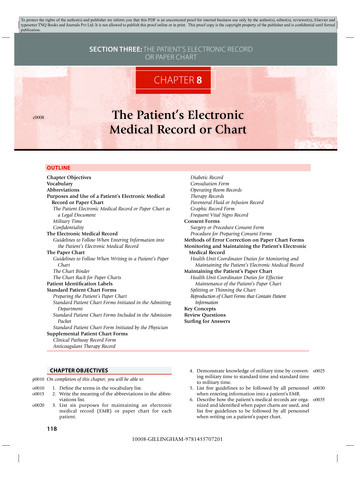
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.120SECTION THREETHE PATIENT’S ELECTRONIC RECORD OR PAPER CHARTmanagement system (HIMS) department, also commonlycalled the medical records department. The advantage of theEMR is that all previous health information is immediatelyavailable on the computer.HIGH PRIORITYb0020Purposes of a Patient’s Electronic Medical Recordor Paper Chart Means of communication Documentation and planning of patient care Research Education Legal record or documentation History of patient illnesses, care, treatment,and outcomess0015 The Patient Electronic Medical Record or PaperChart as a Legal Documentp0305 When a patient is discharged, health information management personnel will analyze and check the EMR for completeness and will notify the appropriate nurses and/or doctorswhen they must go into the computer to complete the records.The patient’s previous EMR will be available on computer tothe patient’s doctor, or if the patient is readmitted to the hospital. The Security Rule, a key part of the Health Insurance Portability and Accountability Act (HIPAA), protects a patient’selectronically stored information (see Chapter 6).The paper chart must be sent to HIMS as soon as possible.p0310Health information management personnel will analyze andcheck the chart for completeness. When records are not complete or signatures are missing, those chart forms are flagged,and the appropriate nurses and/or doctors are notified thatthey must come to HIMS to complete or sign the chart forms.Doctors and nurses must go to HIMS to see or completep0315old patient records if the patient has not been readmitted tothe hospital. Completed paper charts are indexed and storedwhere they are available for retrieval as needed.Older paper records are microfilmed (documents are placedp0320on film in reduced scale) and stored. On request, health information management personnel may retrieve microfilmed records.The length of time that the record must be stored depends onthe laws of the state. Unless a patient has been readmitted tothe hospital, HIMS will not send an old record to nursing units.The patient’s electronic or paper medical record may be subp0325poenaed and may serve as evidence in a court of law. As a legaldocument, it must be maintained in an acceptable manner.s0020 Military Timep0330 Military time is a system that uses all 24 hours in a day (eachhour has its own number) rather than repeating hours andusing AM and PM. When military time is used, there are alwaysfour digits, the first two digits representing hours and the secondtwo representing minutes. For example, 1:45 AM is recorded as0145, and 1:45 PM is recorded as 1345; the colon is not neededwhen military time is used (Table 8-1). The hours after midnight are recorded as 0100, 0200, and so forth. Thirty minutesafter midnight is written as 0030. Twelve noon is recorded as1200, and the hours that follow are arrived at by adding theTABLE 8-1 Standard and Military TimeComparisonsStandardTime12:15 AM12:30 AM12:45 AM1:00 AM2:00 AM3:00 AM4:00 AM5:00 AM6:00 AM7:00 AM8:00 AM9:00 AM10:00 AM11:00 AM12:00 00070008000900100011001200StandardTime1:00 PM1:15 PM1:30 PM1:45 PM2:00 PM3:00 PM4:00 PM5:00 PM6:00 PM7:00 PM8:00 PM9:00 PM10:00 PM11:00 PM12:00 60017001800190020002100220023002400hours after noon to 1200. Thus 1:00 PM is 1200 100 1300, 2PM is 1200 200 1400, and so forth. See Figure 8-1 for a comparison of standard and military times. Military time is usedwith the EMR and paper chart systems and eliminates confusionbecause hours are not repeated, and AM or PM is unnecessary.S K IL L S CH AL L E N G Eb0025To practice converting standard time to military time,complete Activity 8-1 in the Skills Practice Manual.Confidentialitys0025As was discussed in Chapter 6, the EMR or paper chart is con- p0340fidential, and the HUC is a custodian of all patient medicalrecords (electronic or paper) on the unit. Any informationprovided by the patient to the health care facility and the medical staff is confidential. All health care personnel are requiredto have a code and a password to gain access to a patient’sEMR. Portions of the patient’s EMR may be available only tothe patient’s doctor and nurses.HIGH PRIORITYAll access to a patient’s electronic medical record (EMR) ismonitored and recorded in the system. This serves to protect patient confidentiality and is a way to trace any errorsor modifications made in the patient’s EMR.THE ELECTRONIC MEDICAL RECORDb0030s0030The patient’s EMR may be accessed by health care personnel p0350after entering a user ID and a password. Once logged in, thehealth care personnel are able to access and should access onlythe EMR of the patients in their specific nursing unit. Healthcare personnel choose the patient’s name from the nursing unitcensus displayed on the screen; this will allow them to view10008-GILLINGHAM-9781455707201
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.CHAPTER 8Af0010s0035 Guidelines to Follow When Entering Informationinto the Patient’s Electronic Medical Recordo0170 1. All entries into the EMR must be accurate.o0175 2. Handwritten progress notes, electrocardiograms, consents,anesthesia records, and outside records and reports must bescanned into the EMR.o0180 3. Errors made in care or treatment must be documented andcannot be falsified.o0185 4. All entries into the EMR must include the date and time(military or standard) of the entry.o0190 5. Abbreviations may be used in keeping with the health carefacility’s list of “approved abbreviations.”THE PAPER CHARTs0045 Guidelines to Follow When Writing in a Patient’sPaper Chartp0385 All persons who write in the paper chart follow standard guidelines. The HUC has minor charting tasks but is responsible forpatient charts and so should be aware of the following basic rules:o0195o0200121BFigure 8-1 A, A 24-hour clock showing military time. B, Military time.and enter information into the patient’s EMR. An icon willbe displayed next to a patient’s name when there is a task orcommunication for the nurse or HUC written by the patient’sdoctor. A name alert flag may be placed on the patient’s EMRwhen two or more patients with the same or similarly spellednames are located on the unit. If an order has been writtenstating that the patient’s admission is not to be published,NINP (no information, no publication) is noted on the EMRor the patient may be listed as a “confidential patient.”s0040The Patient’s Electronic Medical Record or Chart1. All paper chart form entries must be made in ink. Thisis to ensure permanence of the record. Black ink is preferred by many health care facilities because it producesa clearer picture when the record is microfilmed, faxed,or reproduced on a copier.2. Written entries on paper chart forms must be legible andaccurate. Entries may be made in script or printed. Diagnostic reports, history and physical examination reports,and surgery reports are usually computer generated.3. Recorded entries on the paper chart may not be obliter- o0205ated or erased. The method for correcting errors is outlined later in this chapter.4. All written entries on paper chart forms must include o0210the date and time (military or standard) of the entry.5. Abbreviations may be used in keeping with the health o0215care facility’s list of “approved abbreviations.”The Chart Binders0050Forms that constitute the patient’s paper chart are usually kept p0415together in a three-ring binder. The binder may open from thebottom, or it may be a notebook that opens from the side, thetop, or the bottom (Fig. 8-2).The chart forms in the binder are sectioned off by dividers p0420placed in the chart according to the sequence set forth by thehealth care facility (Fig. 8-3).Paper charts are identified for each patient with a label p0425that contains the patient’s name and the doctor’s name. Theroom and bed number may be written on the outside of thechart binder. Many health care facilities use colored tape onthe outside of the chart to assist doctors in identifying theirpatients’ charts. An allergy label is affixed to the chart binderif the patient has a medication, food, adhesive tape, or othertype of allergy. Labels or tape affixed to chart binders are alsoused to alert the hospital staff of special situations. For example, a name alert, a piece of tape with name alert recordedon it, may be placed on the chart binder to remind staff thatanother patient with the same or a similarly spelled last nameis housed on the unit. When an order indicates that a patient’sadmission is not to be published, NINP is often recorded onthe chart binder to remind staff members that no informationabout a particular patient is to be issued.The Chart Rack for Paper Chartss0055Many types of chart racks are available on the market. One type p0430allows patient paper charts to be placed in a chart rack in whicheach slot on the rack holds one patient chart. Slots are labeledwith the room and bed numbers; they usually are numberedin the same sequence as the rooms on the nursing unit (Fig.8-4). Another type of chart storage is a WALLaroo, a locked10008-GILLINGHAM-9781455707201
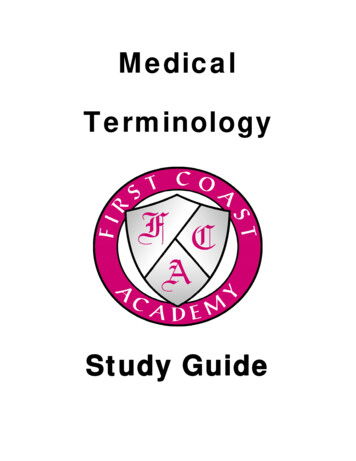
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.122SECTION THREETHE PATIENT’S ELECTRONIC RECORD OR PAPER CHARTf0025Figure 8-4 Chart rack.f0015Figure 8-2 Patient’s chart with dividers.other belongings. Labels may be generated from the computerand printed on a label printer.STANDARD PATIENT CHART FORMSPreparing the Patient’s Paper Chartf0020Figure 8-3 Patient chart binders properly labeled.workstation that is located on the wall outside the patient’sroom. It stores a patient’s paper chart or a laptop computerand when unlocked forms a shelf to write on (Fig. 8-5).HIGH PRIORITYb0035s0060Health care facilities that have implemented the electronic medical record are utilizing the WALLaroo locatedjust outside the patient’s room as a computer workstation.PATIENT IDENTIFICATION LABELSp0440 A packet of patient identification labels is printed from thecomputer when the patient is admitted and as needed duringthe hospital stay. Information on the identification labels usually includes the following: the patient’s name, age, sex, accountnumber, health record number, admission date, and attendingphysician’s name; a bar code may be included for identification purposes (Fig. 8-6). When the EMR is implemented, identification labels are kept in a “label book”; and when papercharts are used, they are kept in each patient’s chart. The identification labels are used on consents, specimens, clothing, ands0065s0070Each health care facility has specific standard forms that are p0445placed in all patients’ paper charts. These forms are preassembled, clipped together (by the HUC or by volunteers),and filed in a drawer or on shelves near the HUC area. Somehospitals use computerized chart forms. These chart forms canbe printed for individual patients with patient identificationinformation printed on the forms. These assembled forms areoften referred to as an admission packet.On a patient admission, the HUC obtains an admission p0450packet from the drawer or shelf and labels each form with thepatient’s identification (ID) label. If the forms are computerized, the HUC chooses the patient’s name on the computer andprints the forms with the patient’s identification informationprinted on them. Forms that need dates and days of the weekare filled in and are then are placed behind the proper chartdivider in a chart binder (Box 8-1, Twelve Standard Chart Forms).HIGH PRIORITYWhen the electronic medical record (EMR) is implemented, information details are directly entered orscanned into the patient’s EMR. Patient identificationlabels are placed in a binder that contains labels and facesheets for all patients on that nursing unit.S K IL L S CH AL L E N G Eb0040b0045To practice preparing a patient’s paper chart, completeActivity 8-2 in the Skills Practice Manual.Standard patient chart forms are included in all inpatient p0465paper charts and may vary in different hospitals. When theEMR is implemented, information is entered into the computer on similar electronic forms. The following standardchart forms are the most commonly used presently.10008-GILLINGHAM-9781455707201
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.CHAPTER 8The Patient’s Electronic Medical Record or Chart123f0030Figure 8-5 A workstation with storage for the patient’s paper chart is called a WALLaroo.Patient’s nameAccount numberDate of admissionAge - SexBar codef0035Williams, John175-09-02Medical record #0078376SurgType of serviceDOA 01/14/20XXDOB 05/07/39Date of birth67Y MDr. Hy HopesAttending doctorMC/BCBSInsurance0Figure 8-6 Patient identification label.BOX 8-1b0085TWELVE STANDARD CHART FORMSInitiated in the Admitting Department1. Face sheet or information form2. Admission and service agreement form3. Patients’ rights4. Advance directive checklistInitiated by the Physician5. History and physical form (H&P)Included in the Admission Packet6. Physician’s order form7. Physician’s progress record8. Nurse’s admission record9. Nurse’s progress notes or flow sheets10. Medication administration record (MAR)11. Nurse’s discharge planning form12. Physician’s discharge summarycare facilities, the form originates in the admitting departmentand is then sent to the unit to be placed in the patient’s chart.When the EMR is implemented, the information is entereddirectly into the patient’s EMR. Several face sheets (at least five)are kept in the binder containing patient labels when EMR isused and in each patient’s chart when paper charts are used.Face sheets are taken by the attending physician and by consulting physicians to be used for billing purposes. The HUCcan generate copies of the face sheet on the computer. The facesheet is also used on the nursing unit to locate informationwhen staff must call the family or call consulting physicians.2. Admission and Service Agreement Form ( may also becalled Conditions of Admission [COA])The admission and service agreement form (Fig. 8-8) is signed p0475by the patient in the admitting department and is then sentto the admitting unit to be scanned into the patient’s EMR orplaced in the patient’s paper chart. The form provides legalpermission to the hospital and doctor to treat the patient andalso serves as a financial agreement.3. Patients’ Rightss0075 Standard Patient Chart Forms Initiated in theAdmitting Departments0080 1. Face Sheet or Information Formp0470 The face sheet or information form (Fig. 8-7) contains information about the patient, such as name, address, telephonenumber, name of employer, admission diagnosis, health careinsurance policy information, and next of kin. In most healths0085s0090The Joint Commission requires that all hospitals have a bill p0480of rights and a notice of the facility’s privacy practices. Copiesmust be given to each patient or legal guardian of the patienton admission. In addition, a copy of the bill of rights shouldbe posted at entrances and other prominent places throughout the hospital. The patients’ bill of rights varies in wordingamong hospitals, but all are based on the basic ethical principles outlined in Chapter 6.10008-GILLINGHAM-9781455707201
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.124SECTION THREETHE PATIENT’S ELECTRONIC RECORD OR PAPER CHARTOpportunity Medical CenterAccount # Admit Date Admit Time Reg Init0114940801/14/XX1430Brought ByEGPrimary Care Phys.John BauerAdmitting PhysicianJohn BauerPatient Last NameFirstInfo Provided ByWifeMiddleRoom #406CityStateApt. No.SinclaireAgeN/ABirth Date05/07/3967Patient EmployerBirthplace GenderOhioMDischargeDateTimeServiceSurgRaceC294 W Filmore StDriver’s License #TypeFormer NameWilliams, JohnPatient AddressMR Number30897811PatientRel Prefdo notSocial Security #111-11-1111Zip CodeNJPatient Phone #90376-9009222-222-2222MSOccupation Accident? Date/TimeMTeacherN/AEmployer PhoneEmployer AddressRetired May 2005Spouse NameCitySpouse AddressElaine Ann9030 W. 3 AveEmergency ContactPeoriaRelationshipJean SoundersHome Phonedaughter102-202-2002StateSpouse PhoneOhio200-330-3333Cell PhoneWork PhoneN/A102-101-1001Admit Type ICD9Admitting DiagnosisAdmit SourceSurgMVA - diabetesPrimary Insurance PlanPrimary Policy #MedicareAuthorization #ClinicPrimary Policy Holder111-11-1111ASecondary Policy # Authorization #Insurance Plan #2Pacific CareSecondary Policy Holder22020111Insurance Plan #3Tertiary Policy #Guarantor NameRel to PtGuarantor OccupationEmployerAuthorization #Tertiary Policy HolderGuarantor PhoneMailing AddressEmployer PhoneEmployer AddressBilling Remarks:MVAPrincipal Diagnosis:Code: 050Secondary Diagnosis: DiabetesCode: 268Operations and Procedures:PhysicianDateCodeConsulting Physician:Final Disposition:DischargedTransferredLeft AMAExpiredAutopsyYesNoI certify that my identification of the principal and secondary diagnosisand the procedures performed is accurate to the best of my knowledge.Opportunity Medical Centerf0040Attending PhysicianDateFigure 8-7 Face sheet or information form. (Copyright 2004, Elsevier Inc. All Rights Reserved.)10008-GILLINGHAM-9781455707201
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier andtypesetter TNQ Books and Journals Pvt Ltd. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formalpublication.CHAPTER 8125The Patient’s Electronic Medical Record or ChartMEDICAL TREATMENT AGREEMENT(Conditions of Admission)Williams, John175-09-020078376SurgDOA 01/14/20XXDOB 05/07/3967Y MDr. Hy HopesMC/BCBS0Patient or the patient’s legal representative agrees to the following terms of hospital admission:1. MEDICAL TREATMENT :The patient consents to the treatment, services and procedures which may be performed during this hospitalization or on an outpatientbasis, which may include but are not limited to laboratory procedures, X-ray examinations, medical and surgical treatments orprocedures, anesthesia, or hospital services rendered under the general or specific instructions of the responsible physicians or otherhealth care providers. The hospital may establish certain criteria which will automatically trigger the performance of specific tests which thepatient agrees may be performed without any further separate consent. This Medical Treatment Agreement covers E-ICU services andoutpatient services provided by the hospital’s extended treatment facilities, including services at other Banner facilities. Where thehospital routinely provides services for inpatients at an outpatient facility in close proximity to the hospital, the patient consents totransport to the outpatient facility for the requested services. This Medical Treatment Agreement is effective for this inpatientadmission/outpatient visit and/or for recurring outpatient services of the same type for a period of one year following its execution. Forobstetrical patients this Medical Treatment Agreement covers both outpatient and inpatient services and also covers and applies toboth the obstetrical patient and the newborn(s). Photographs or videotapes may be made of diagnostic and surgical procedures fortreatment and/or training purposes.2. LEGAL RELATIONSHIP BETWEEN HOSPITAL AND HEALTH CARE PROVIDERS:The patients will be treated by his/her attending physician or health care providers and be under his/her care and supervision.Physicians and other health care providers furnishing services to the patient, including but not limited to the emergencyroom physician, hospitalist, radiologist, pathologist, and anesthesiologist, are generally not employees or agents of thehospital. These providers may bill separately for their services. Questions about whether a health care provider is an agent oremployee of the hospital should be directed to Administration during normal business hours, and the Administrator On Call orthe Chief Nursing Officer/Designee after hours, weekends, and holidays.3. MONEY AND VALUABLES:VALUABLES AND MONEY SHOULD BE RETU
CHAPTER 8 The Patient’s Electronic Medical Record or Chart 119 10008-GILLINGHAM-9781455707201 To protect the rights of the author(s) and publisher we inform you that this PDF